Nonaccidental trauma
| Nonaccidental trauma | |
 | |
|---|---|
| Posterior rib fractures. Image courtesy of RadsWiki |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Nonaccidental trauma is the radiology term for child abuse. It is estimated that in 2001, 903,000 children (Comparison: the incidence of osteosarcoma in the US is 400 cases per year.) were victims of maltreatment including: [1] [2] [3] [4] [5] [6]
- Neglect (57%)
- Medical neglect (2%)
- Physical abuse (19%)
- Sexual abuse(10%)
- Psychologic maltreatment (7%)
Cutaneous injury is the most common injury due to abuse.
Skeletal trauma is the second most common manifestation of abuse.
Virtually every type and location of fracture has been documented in abused children. Fracture is documented in 11%–55% of physically abused children.
- In a large series of abuse-related fractures,
- 76%: long bones
- 8%: skull
- 8%: rib cage
- The American College of Radiology (ACR) and the Section on Radiology of the American Academy of Pediatrics recommend that a high-quality radiographic skeletal survey involve the use of a high-resolution imaging system, with technical factors designed to optimize image contrast and spatial resolution include an appropriate number of well-collimated views of each anatomic region.
- Babygram is not acceptable
Metaphyseal Fracture
- Virtually pathognomonic of abuse
- Distal femur, proximal tibia, distal tibia, and proximal humerus
- Discovered in 39%–50% of abused children less than 18 months of age
- Almost exclusively in children less than 2 years of age
- Generated by manual to-and-fro manipulation of the extremities
- holding and shaking an infant by the feet or hands
- shaking the infant while he is held around the chest, with the limbs whiplashing back and forth
Rib fractures
- Strongly correlated with abuse because the mechanism that generates the fractures is relatively specific.
- Fractures of the first rib are considered virtually diagnostic of child abuse, since they require considerable force.
- Very tight hold around the infant chest generates substantial squeezing force on the immature skeleton
- May result in fractures of the anterior, lateral, and posterior aspects of the rib.
Skull fractures
- Skull fractures result from contact injury
- Object striking the skull
- Skull as it strikes a stationary object (as in a fall)
- Studies have demonstrated that multiple fractures, fractures that cross sutures, and bilateral fractures are more likely to be associated with abuse
Other fractures
- Virtually every type of fracture has been described in the setting of inflicted trauma. Therefore, any fracture is possibly abusive in origin.
- Particular attention should be paid to the patient’s history, the age and developmental abilities of the injured child, and the injury and its mechanism.
The S fractures: specific for nonaccidental truama
- Scapula
- Spinous process
- Sternum
Spinal fractures
- Any spinal fracture without good accidental explanation is suggestive of abuse.
- Thoracolumbar compression fracture may be caused by shaking when a baby is held around the chest and shaken, there is extension and flexion, centered at the thoracolumbar junction.
Spiral fractures
- Spiral fractures wind around a long bone and are the result of torsional forces applied to the bone.
- Distinctly uncommon in infants, who typically sustain accidental injury from falls.
- Once a child is walking, spiral fractures of the tibia (toddler's fracture) are quite common.
Imaging Findings for Nonaccidental trauma
Plain film
Metaphyseal Fracture
- Fracture line is oriented essentially parallel to the physis
- Thicker peripheral rim is more readily visible and appears as a triangular fragment when viewed in profile: corner fracture.
- If the fragment is separated from the remainder of the long bone by a prominent fracture lucency, or if the fracture is viewed at a slightly oblique angle, the thick rim may be visible as a curvilinear: bucket handle.
Rib fractures
- Because the forces are distributed in an area similar to the size of the perpetrator’s hands, fractures are typically seen in similar locations in multiple adjacent ribs and are often bilateral (note: bone scan can demonstrate radiographically occult rib fractures in 10% of abused children).
-
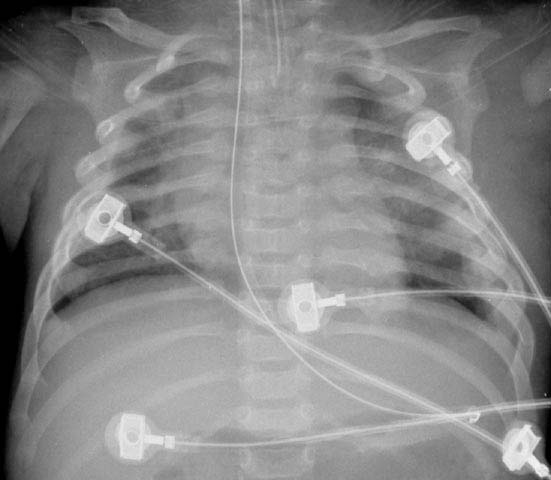
Posterior rib fractures
-

Posterior rib fractures

Skull fractures
- Radiography of the skull is preferred over CT, because fractures parallel or nearly parallel to the section orientation are missed at CT.
- Two views (anteroposterior and lateral) are recommended as part of the skeletal radiographic survey, with additional views taken as necessary, especially if head trauma is suspected
References
- ↑ Barnes PD. Ethical issues in imaging nonaccidental injury: child abuse. Top Magn Reson Imaging. 2002 Apr;13(2):85-93.
- ↑ Kemp AM, Butler A, Morris S, Mann M, Kemp KW, Rolfe K, Sibert JR, Maguire S. Which radiological investigations should be performed to identify fractures in suspected child abuse? Clin Radiol. 2006 Sep;61(9):723-36.
- ↑ Kleinman PL, Kleinman PK, Savageau JA. Suspected infant abuse: radiographic skeletal survey practices in pediatric health care facilities. Radiology. 2004 Nov;233(2):477-85. Epub 2004 Sep 16.
- ↑ Lonergan GJ, Baker AM, Morey MK, Boos SC. From the archives of the AFIP. Child abuse: radiologic-pathologic correlation. Radiographics. 2003 Jul-Aug;23(4):811-45.
- ↑ Mogbo KI, Slovis TL, Canady AI, Allasio DJ, Arfken CL. Appropriate imaging in children with skull fractures and suspicion of abuse. Radiology. 1998 Aug;208(2):521-4.
- ↑ Tenney-Soeiro R, Wilson C. An update on child abuse and neglect. Curr Opin Pediatr. 2004 Apr;16(2):233-7. Review.