Non small cell lung cancer CT: Difference between revisions
No edit summary |
No edit summary |
||
| Line 43: | Line 43: | ||
:*Commonly cause segmental or lobar lung collapse due to central location | :*Commonly cause segmental or lobar lung collapse due to central location | ||
*[[Large cell carcinoma of the lung|Large cell lung carcinoma]] | *'''[[Large cell carcinoma of the lung|Large cell lung carcinoma]]''' | ||
:*Rapid growth | :*Rapid growth | ||
:*Early metastasizes to the mediastinum and brain | :*Early metastasizes to the mediastinum and brain | ||
| Line 50: | Line 50: | ||
:* '''Finger in glove sign''': the bronchus distal to the obstruction is dilated | :* '''Finger in glove sign''': the bronchus distal to the obstruction is dilated | ||
:* '''Crazy-paving sign''': appearance of ground-glass opacity with superimposed interlobular septal thickening and intralobular reticular thickening. | :* '''Crazy-paving sign''': appearance of ground-glass opacity with superimposed interlobular septal thickening and intralobular reticular thickening. | ||
==Gallery== | ==Gallery== | ||
Revision as of 21:50, 24 February 2016
|
Non Small Cell Lung Cancer Microchapters |
|
Differentiating Non Small Cell Lung Cancer from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Non small cell lung cancer CT On the Web |
|
American Roentgen Ray Society Images of Non small cell lung cancer CT |
|
Directions to Hospitals Treating Non small cell carcinoma of the lung |
|
Risk calculators and risk factors for Non small cell lung cancer CT |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Maria Fernanda Villarreal, M.D. [2]
Overview
Computed tomography is the method of choice for the diagnosis of non-small cell lung cancer. On CT, characteristic findings of non-small cell lung cancer, include: ground-glass opacity, rounded or spiculated mass, local nodal involvement, intraluminar obstruction, and lobar collapse.[1][2]
CT
- Computed tomography is the method of choice for the diagnosis of non-small cell lung cancer
- In some cases, non-small cell lung cancers require further evaluation with MRI
- Common features of CT scan for the diagnosis of non-small cell lung cancer, include:[3]
- Assessment of the main bronchi
- Evaluation of the entire thorax
- Detection of chest wall invasion
- Assessment of hiliar and mediastinal invasion/adenopathy
- Determination of non-small cell lung cancer staging
- Precise determination of size and tumor dimensions
- Detection of liver, bone, adrenal and brain metastasis
- On CT, characteristic findings of non-small cell lung cancer, include:[3]
- Lung adenocarcinoma
- Lung adenocarcinomas are typically peripherally located
- Usually measure <4 cm in diameter, very few show cavitation
- Peri-hilar and mediastinal involvement
- Ground glass opacity (slow growth), usually lesions double the size within a year
- Subtype of adenocarcinoma
- Single pulmonary nodule or mass
- Multicentric or diffuse disease
- Localized area of parenchymal consolidation
- Bubble-like areas of low attenuation within the mass are a characteristic finding
- Hilar and mediastinal lymphadenopathy is uncommon
- Persistent peripheral consolidation with associated nodules
- Centrally located within the lung
- Usually measure larger than 4 cm in diameter
- Frequent cavitation
- Commonly cause segmental or lobar lung collapse due to central location
- Rapid growth
- Early metastasizes to the mediastinum and brain
- Finger in glove sign: the bronchus distal to the obstruction is dilated
- Crazy-paving sign: appearance of ground-glass opacity with superimposed interlobular septal thickening and intralobular reticular thickening.
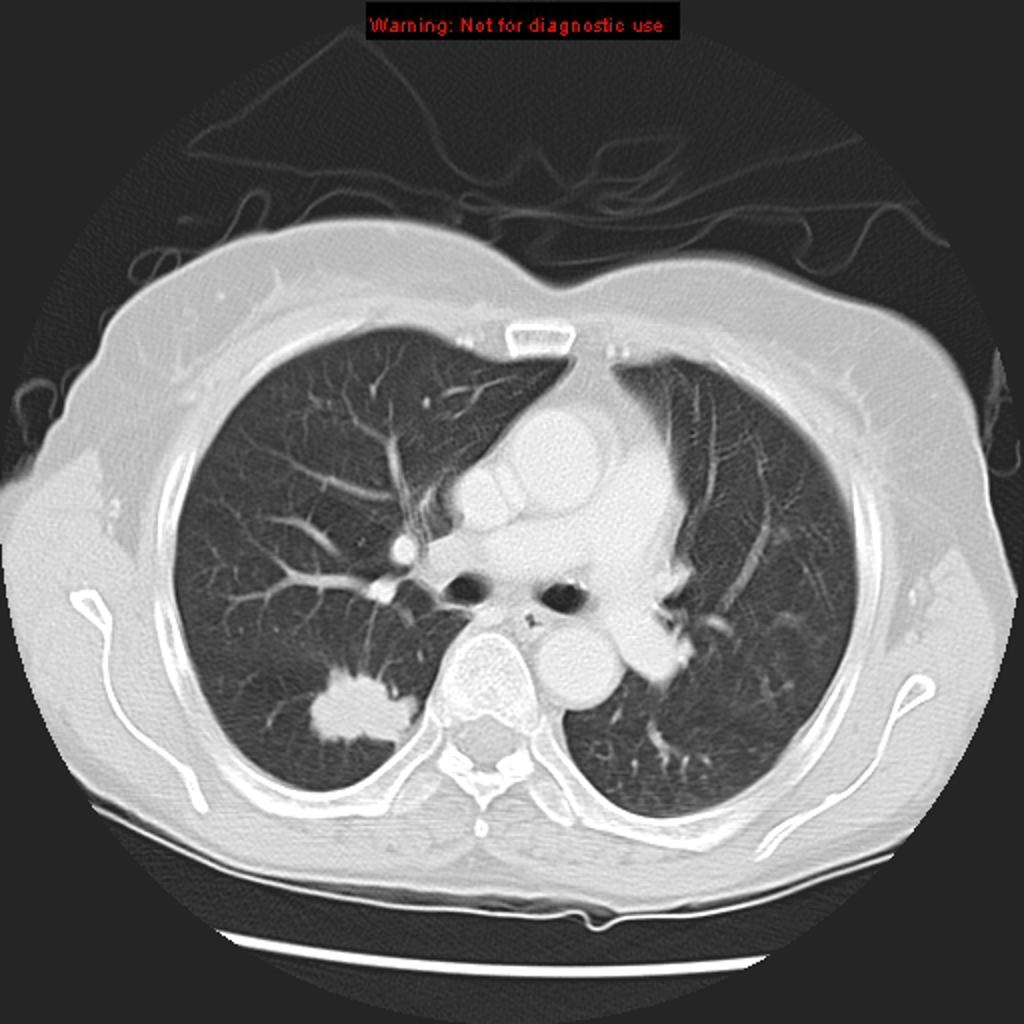
Gallery
-
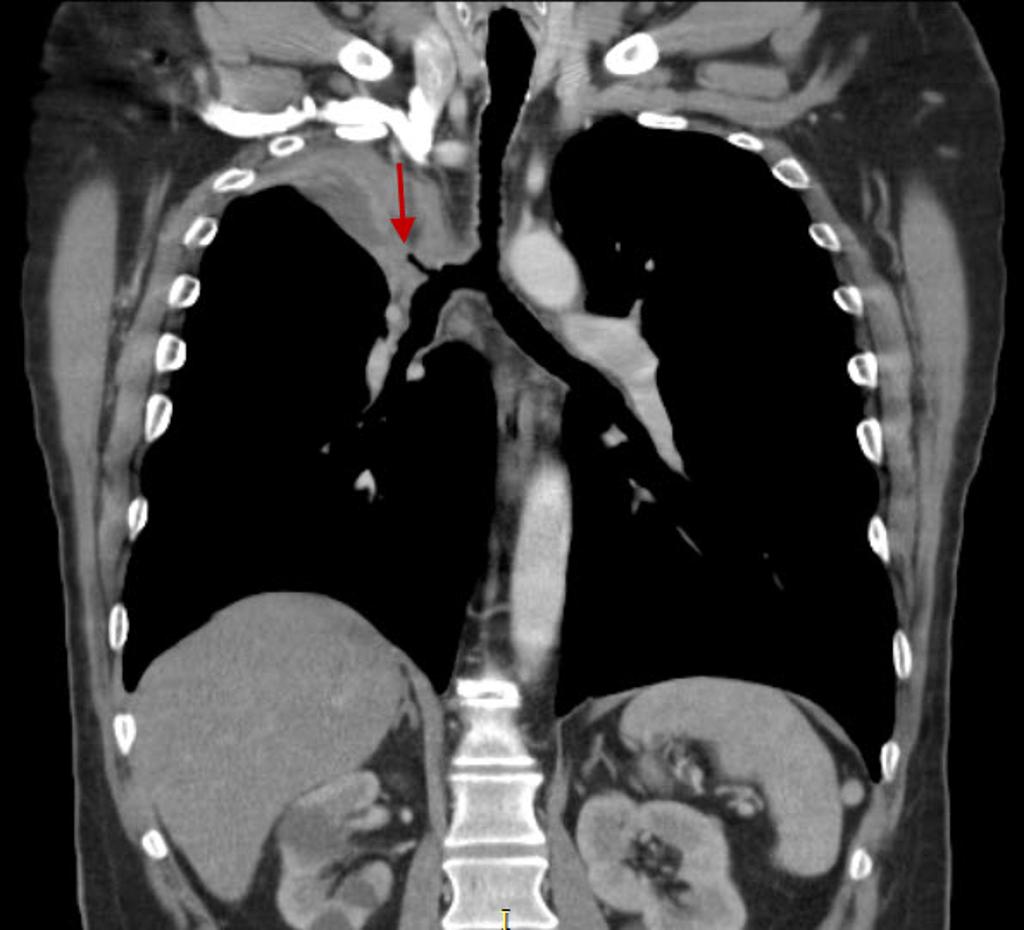
Bronchogenic lung carcincoma: upper lobe collapse
-

Bronchogenic lung carcincoma: upper lobe with lymphangitic spread
-
Ádenocarcinoma of the lung: ground-glass attenuation corresponds to a lepidic growth pattern and the solid component correspond to invasive patterns.
-

Squamous cell lung carcinoma: Peripheral squamous cell lung carcinoma may be seen as a solid nodule/mass with or without an irregular border. The irregular margin can be attributed to a desmoplastic reaction or infiltrative growth




References
- ↑ Rosado-de-Christenson ML, Templeton PA, Moran CA (1994). "Bronchogenic carcinoma: radiologic-pathologic correlation". Radiographics. 14 (2): 429–46, quiz 447–8. doi:10.1148/radiographics.14.2.8190965. PMID 8190965.
- ↑ 2.0 2.1 Parker MS, Chasen MH, Paul N (2009). "Radiologic signs in thoracic imaging: case-based review and self-assessment module". AJR Am J Roentgenol. 192 (3 Suppl): S34–48. doi:10.2214/AJR.07.7081. PMID 19234288.
- ↑ 3.0 3.1 3.2 Kundel HL (1981). "Predictive value and threshold detectability of lung tumors". Radiology. 139 (1): 25–9. doi:10.1148/radiology.139.1.7208937. PMID 7208937.