Coagulative necrosis
| Coagulative necrosis | |
 | |
|---|---|
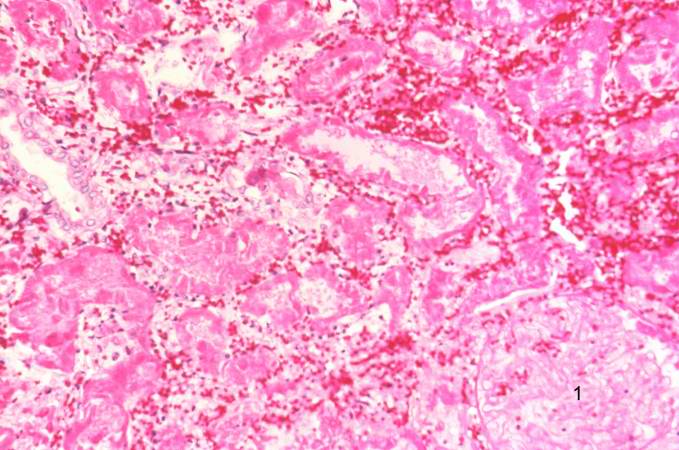
| A high-power photomicrograph shows the edge of this reddish area, illustrating coagulation necrosis (1) compared to the normal tissue (2). The necrotic tubules in this hemorrhagic, red infarct are hypereosinophilic. Compare the tubules on the right with the normal tubules seen in the left-hand portion of the slide. Note the interstitial hemorrhage which is associated with vascular leakage within this necrotic region in the tissue. Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Coagulative Necrosis is a type of accidental cell death typically caused by ischemia or infarction.
It is characterised by the 'ghostly' appearance of cells under light microscopy in the affected area of tissue. Like most types of necrosis if enough labile cells are present around the affected area regeneration can occur.
Causes
Coagulative necrosis is most commonly caused by hypoxic conditions, which don't involve severe trauma, toxins or an acute or chronic immune response. The lack of oxygen causes cell death in a localised area which is perfused by blood vessels failing to deliver primarily oxygen, but also other important nutrients. It is important to note that while ischemia in most tissues of the body will cause coagulative necrosis, in the central nervous system ischemia causes liquefactive necrosis as there is very little structural framework in the brain tissue.
Pathology
Macroscopic
The macroscopic appearance of an area of coagulative necrosis is a pale segment of tissue contrasting against surrounding well vascularised tissue. The surrounding survivng cells can aid in regeneration of the affected tissue unless they are stable or permanent cells.
Microscopic
The microscopic anatomy shows a lighter staining tissue (when stained with H&E) containing no nuclei with very little structural damage giving the appearance often quoted as 'ghost cells'. The decreased staining is due to digested nuceli which no longer show up as dark purple when stained with hematoxylin and removed cytoplasmic structures giving reduced amounts of intracellular protein reducing the usual dark pink staining cytoplasm with eosin.
Regeneration
As the majority of the structural remnants of the necrotic tissue remains, labile cells adjacent to the affected tissue will replicate and replace the cells which have been killed during the event. Labile cells are constantly undergoing mitosis and can therefore help reform the tissue, whereas nearby stable and permanent cells (eg. neurons and cardiomyocytes) do not undergo mitosis and will not replace the tissue affected. Fibroblasts will also migrate to the affected area depositing fibrous tissue producing fibrosis or scarring in areas where labile cells do not replicate and replace tissue.
Pathological Findings: Case #1: Kidney: Coagulative Necrosis
Clinical Summary
A 48-year-old black male committed suicide by ingesting an unidentified toxin, after which he went into profound shock and died.
Autopsy Findings
An incidental finding at autopsy was a small renal lesion which was reddish-tan in color, sharply delineated, and triangular in shape. The base of the lesion was located at the capsular surface and its apex at the corticomedullary junction.
-
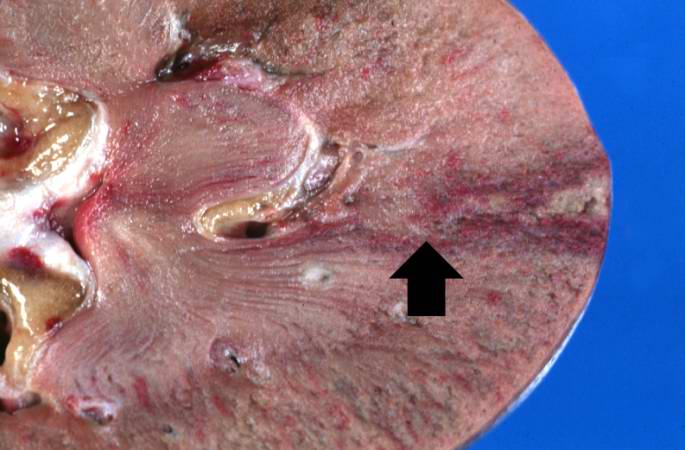
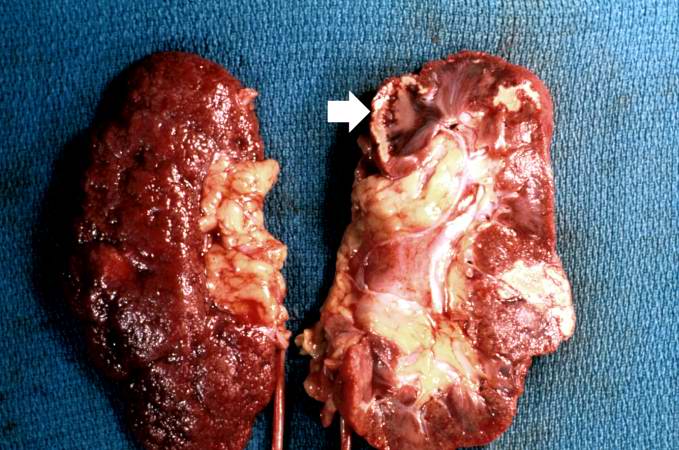 This gross photograph shows a kidney that has been transected longitudinally at autopsy. The cut surface (right) shows several areas of infarction. The most recent infarct is seen at the top left (arrow). The surface of the kidney (left) shows a marked nodularity and roughening from scarring due to chronic hypertension.
This gross photograph shows a kidney that has been transected longitudinally at autopsy. The cut surface (right) shows several areas of infarction. The most recent infarct is seen at the top left (arrow). The surface of the kidney (left) shows a marked nodularity and roughening from scarring due to chronic hypertension. -
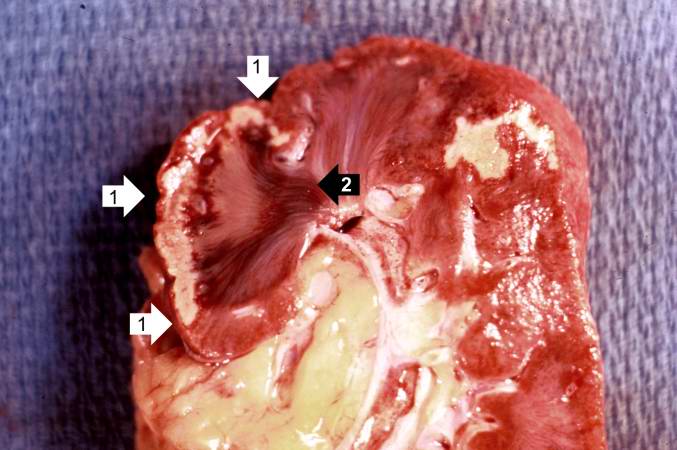 This is a closer view of the triangular-shaped infarction with the base at the cortical surface (1) and the apex at the corticomedullary junction (2).
This is a closer view of the triangular-shaped infarction with the base at the cortical surface (1) and the apex at the corticomedullary junction (2).


-
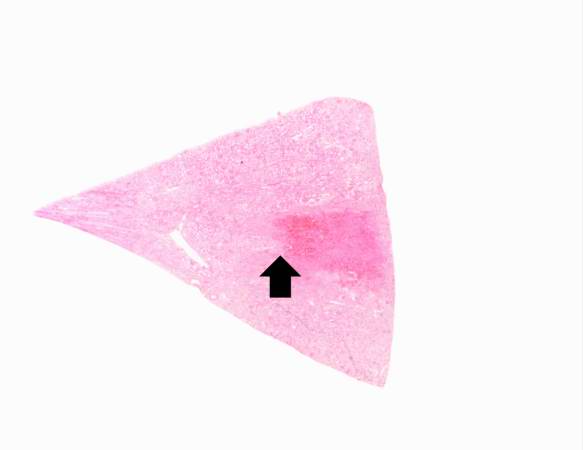 This low-power photomicrograph of the kidney illustrates a sharply demarcated area of red discoloration extending from the capsule to the cortical medullary junction (arrow).
This low-power photomicrograph of the kidney illustrates a sharply demarcated area of red discoloration extending from the capsule to the cortical medullary junction (arrow). -
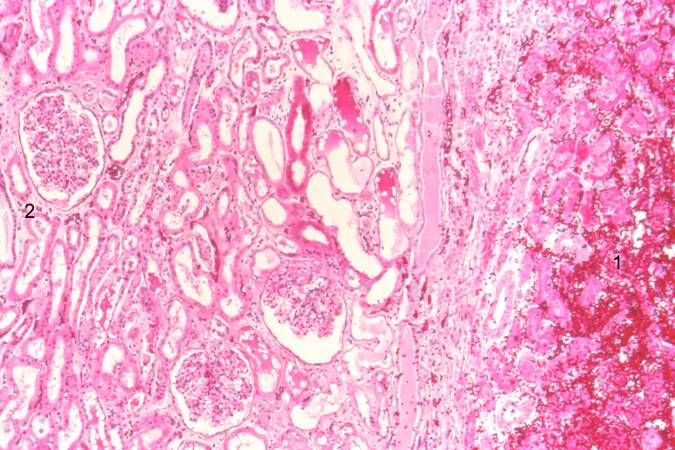 A higher-power photomicrograph shows the edge of this reddish area, illustrating coagulation necrosis (1) compared to the normal tissue (2). The necrotic tubules in this hemorrhagic, red infarct are hypereosinophilic. Compare the tubules on the right with the normal tubules seen in the left-hand portion of the slide. Note the interstitial hemorrhage which is associated with vascular leakage within this necrotic region in the tissue.
A higher-power photomicrograph shows the edge of this reddish area, illustrating coagulation necrosis (1) compared to the normal tissue (2). The necrotic tubules in this hemorrhagic, red infarct are hypereosinophilic. Compare the tubules on the right with the normal tubules seen in the left-hand portion of the slide. Note the interstitial hemorrhage which is associated with vascular leakage within this necrotic region in the tissue.

-
 This higher-power view of the infarct demonstrates retention of the tubular structure and cellular outlines. In the lower right-hand corner is a barely identifiable glomerulus (1). Note that, although the cellular architecture is retained, there are no nuclei within the renal tubular cells. The nuclei visible in this photomicrograph are the nuclei of inflammatory cells.
This higher-power view of the infarct demonstrates retention of the tubular structure and cellular outlines. In the lower right-hand corner is a barely identifiable glomerulus (1). Note that, although the cellular architecture is retained, there are no nuclei within the renal tubular cells. The nuclei visible in this photomicrograph are the nuclei of inflammatory cells. -
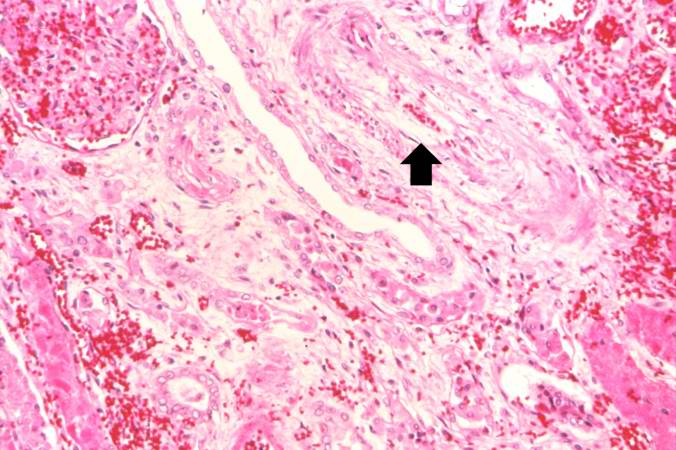 This section, taken at the cortical medullary junction, illustrates a blood vessel in the upper right portion of the slide (arrow) which is filled with thrombotic material. This vessel has occluded an end artery resulting in ischemia and infarction.
This section, taken at the cortical medullary junction, illustrates a blood vessel in the upper right portion of the slide (arrow) which is filled with thrombotic material. This vessel has occluded an end artery resulting in ischemia and infarction. -
 This gross photograph of an infarcted kidney is from another case. The triangular shape of an infarct is prominent on the right side of the image; the apex (arrow) of the triangle is evident at the corticomedullary junction.
This gross photograph of an infarcted kidney is from another case. The triangular shape of an infarct is prominent on the right side of the image; the apex (arrow) of the triangle is evident at the corticomedullary junction.



Pathological Findings: Case #2: Heart: Coagulative Necrosis
Clinical Summary
This was a 57-year-old male whose hospital course following abdominal surgery was characterized by progressive deterioration and hypotension. Four days post-operatively, the patient sustained an anterior myocardial infarction and died the next day.
Autopsy Findings
The patient's heart weighed 410 grams. Examination of the coronary arteries revealed marked atherosclerotic narrowing of all three vessels with focal occlusion by a thrombus of the left anterior descending artery.
Fresh necrosis of the anterior wall of the left ventricle and anterior portion of the septum was present, extending from the endocardium to the inner half of the ventricular wall.
-
 A gross image of the heart from this case, note the area of fresh myocardial infarction (arrows) in the anterior portion of the left ventricle and extending into the anterior portion of the interventricular septum. Note that the walls of the left and right ventricle are slightly thicker than normal.
A gross image of the heart from this case, note the area of fresh myocardial infarction (arrows) in the anterior portion of the left ventricle and extending into the anterior portion of the interventricular septum. Note that the walls of the left and right ventricle are slightly thicker than normal. -
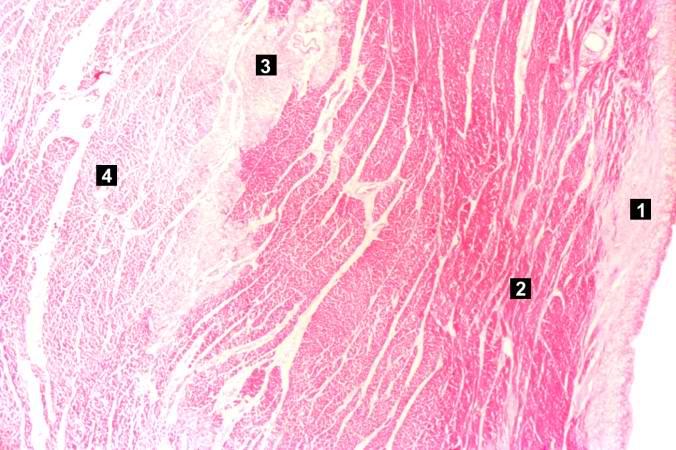
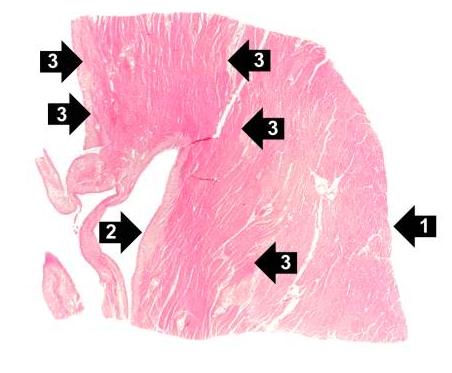 This is a low-power photomicrograph of the left ventricular free wall extending from the epicardium (1) to the endocardium (2). The area of infarction is the darker red (hypereosinophilic area) along the subendocardium (3).
This is a low-power photomicrograph of the left ventricular free wall extending from the epicardium (1) to the endocardium (2). The area of infarction is the darker red (hypereosinophilic area) along the subendocardium (3).


-
 This higher-power photomicrograph shows endocardium on the right side of this image. Directly beneath the endocardium is a pale area consisting of cardiac myocytes exhibiting vacuolar degeneration (1). The area of infarction is visible as a hypereosinophilic area (2) and there is a second zone of vacuolated myocytes (3) between the infarct and the normal myocardium (4).
This higher-power photomicrograph shows endocardium on the right side of this image. Directly beneath the endocardium is a pale area consisting of cardiac myocytes exhibiting vacuolar degeneration (1). The area of infarction is visible as a hypereosinophilic area (2) and there is a second zone of vacuolated myocytes (3) between the infarct and the normal myocardium (4). -
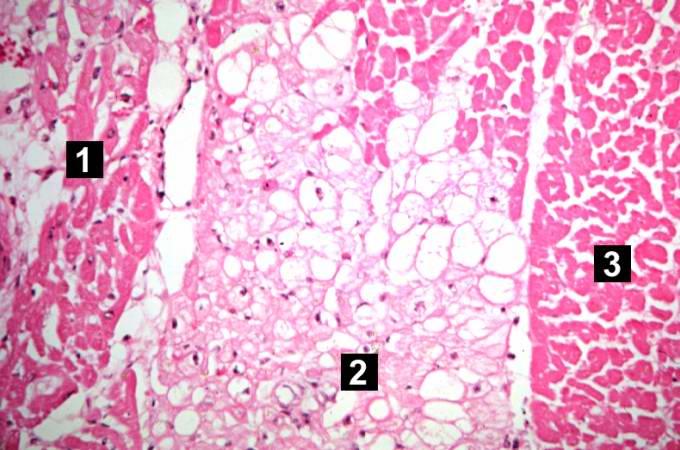
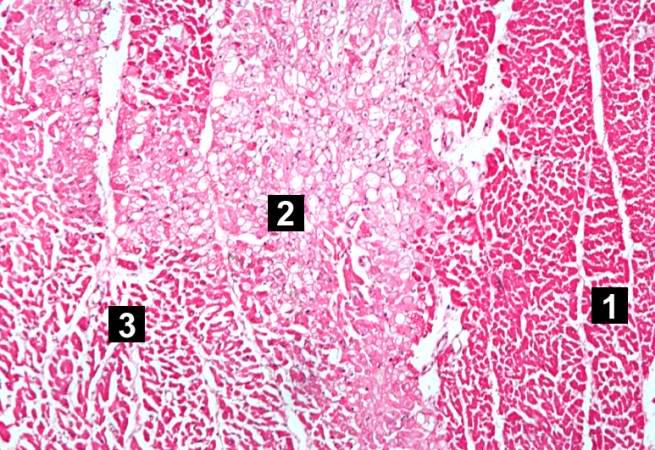 This high-power photomicrograph shows the area of infarction on the right (1). There is an area of vacuolated myocytes (2) adjacent to the infarcted myocytes and then normal cardiac muscle to the left (3).
This high-power photomicrograph shows the area of infarction on the right (1). There is an area of vacuolated myocytes (2) adjacent to the infarcted myocytes and then normal cardiac muscle to the left (3).


-
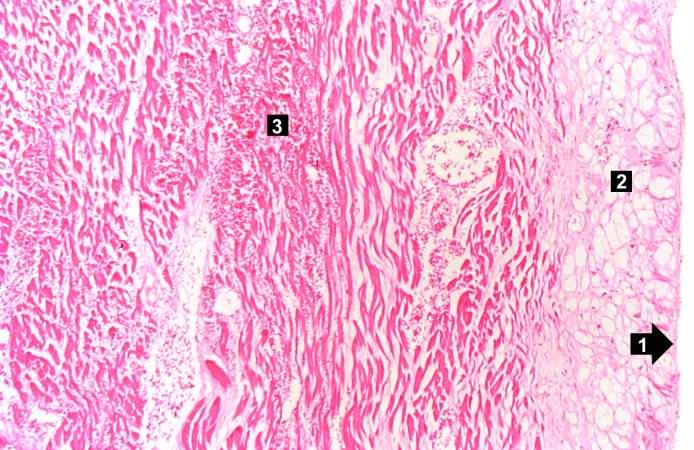 This high-power photomicrograph shows the endocardium (1) and the area of subendocardial vacuolar degeneration (2). The area of infarction (3) contains some red blood cells.
This high-power photomicrograph shows the endocardium (1) and the area of subendocardial vacuolar degeneration (2). The area of infarction (3) contains some red blood cells. -
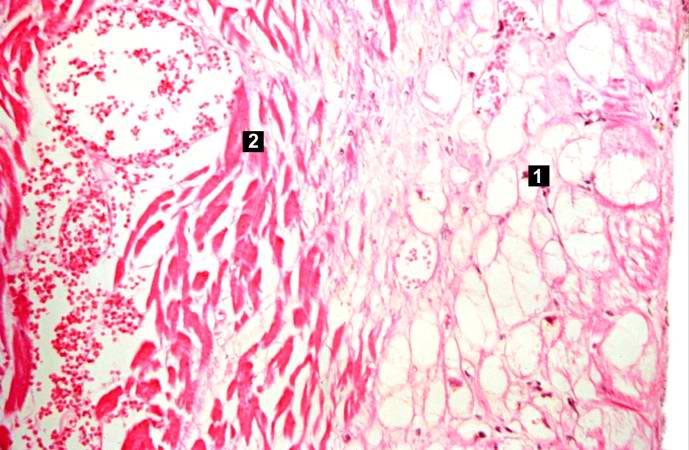 This high-power photomicrograph demonstrates the border between the vacuolated subendocardial myocytes (1) and the infarcted myocytes (2).
This high-power photomicrograph demonstrates the border between the vacuolated subendocardial myocytes (1) and the infarcted myocytes (2). -
 This high-power photomicrograph contains normal myocytes (1), vacuolated myocytes (2), and infarcted myocytes (3).
This high-power photomicrograph contains normal myocytes (1), vacuolated myocytes (2), and infarcted myocytes (3).


