Wide complex tachycardia electrocardiogram: Difference between revisions
Jump to navigation
Jump to search
| Line 19: | Line 19: | ||
|- | |- | ||
! | ! | ||
! | !Example | ||
! | !Regularity | ||
! | !Atrial frequency | ||
! | !Ventricular frequency | ||
! | !Origin (SVT/VT) | ||
!p-wave | !p-wave | ||
! | !Effect of adenosine | ||
|- | |- | ||
| colspan="8" style="text-align:left;background-color:#cfefcf;" | '''Wide complex (QRS > 0.12)''' | | colspan="8" style="text-align:left;background-color:#cfefcf;" | '''Wide complex (QRS > 0.12)''' | ||
Revision as of 18:19, 8 February 2013
|
Wide complex tachycardia Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Wide complex tachycardia electrocardiogram On the Web |
|
American Roentgen Ray Society Images of Wide complex tachycardia electrocardiogram |
|
Risk calculators and risk factors for Wide complex tachycardia electrocardiogram |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Electrocardiogram
EKG examples and diagnosis here:
- Extreme axis deviation favors VT. Especially -90 to -180 or “northwest” or “superior” axis (23% of SVT will have SAD).
- QRS duration >140 msec favors VT (21% of VT will have QRS <140 msec).
- AV dissociation is demonstrated in only 21% of VT.
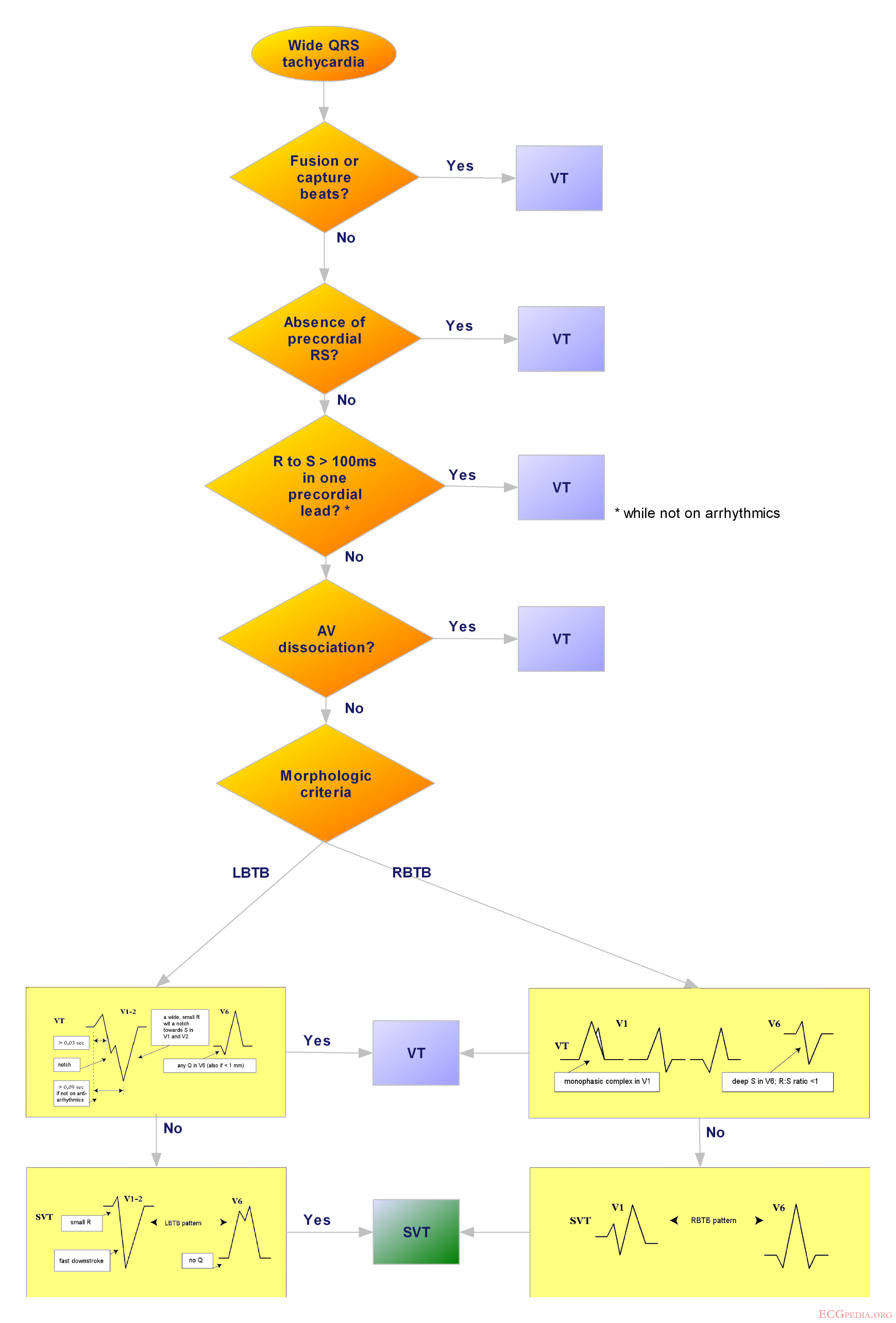
- Morphologic criteria:
- 4% of SVT and 6% of VT did not fulfill criteria in any lead.
- 40% will have discordance between V1/V2 and V5/V6. One lead may suggest VT while another suggests SVT.
- An algorithmic approach was proposed by Brugada in 1991. It has a reported sensitivity of 99% and specificity of 97%.
| Example | Regularity | Atrial frequency | Ventricular frequency | Origin (SVT/VT) | p-wave | Effect of adenosine | |
|---|---|---|---|---|---|---|---|
| Wide complex (QRS > 0.12) | |||||||
| Ventricular Tachycardia | regular (mostly) | 60-100 bpm | 110-250 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | |
| Ventricular Fibrillation | irregular | 60-100 bpm | 400-600 bpm | ventricle (VT) | AV-dissociation | none | |
| Ventricular Flutter | regular | 60-100 bpm | 150-300 bpm | ventricle (VT) | AV-dissociation | none | |
| Accelerated Idioventricular Rhythm | regular (mostly) | 60-100 bpm | 50-110 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | |
| Torsade de Pointes | regular | 150-300 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | ||
| Bundle-branch re-entrant tachycardia* | regular | 60-100 bpm | 150-300 bpm | ventricles (VT) | AV-dissociation | no rate reduction | |
| * Bundle-branch re-entrant tachycardia is extremely rare | |||||||
{kind=link}