Pulmonary embolism electrocardiogram
|
Pulmonary Embolism Microchapters |
|
Diagnosis |
|---|
|
Pulmonary Embolism Assessment of Probability of Subsequent VTE and Risk Scores |
|
Treatment |
|
Follow-Up |
|
Special Scenario |
|
Trials |
|
Case Studies |
|
Pulmonary embolism electrocardiogram On the Web |
|
Directions to Hospitals Treating Pulmonary embolism electrocardiogram |
|
Risk calculators and risk factors for Pulmonary embolism electrocardiogram |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editors-in-Chief: Ujjwal Rastogi, MBBS [2]
Synonyms and keywords: PE
Electrocardiogram
- The most common ECG finding is anterior T-wave inversion.
- This likely represents reciprocal changes reflecting infero-posterior ischemia due to compression of the right coronary artery (RCA) as a result of pressure overload in the right ventricle (RV).
- Sinus tachycardia, right bundle branch block (RBBB), SIQIIITIII, and a normal ECG are also frequently seen, but again are not sensitive or specific
- There may be an S wave in lead 1, a Q wave in lead 3, and a flipped T wave in lead 3 (S1Q3T3 pattern).
An ECG may show signs of right heart strain or acute cor pulmonale in cases of large PEs - the classic signs are a large S wave in lead I, a large Q wave in lead III and an inverted T wave in lead III ("S1Q3T3").[1] This is occasionally (up to 20%) present, but may also occur in other acute lung conditions and has therefore limited diagnostic value; the most commonly seen sign in the ECG is sinus tachycardia.
-
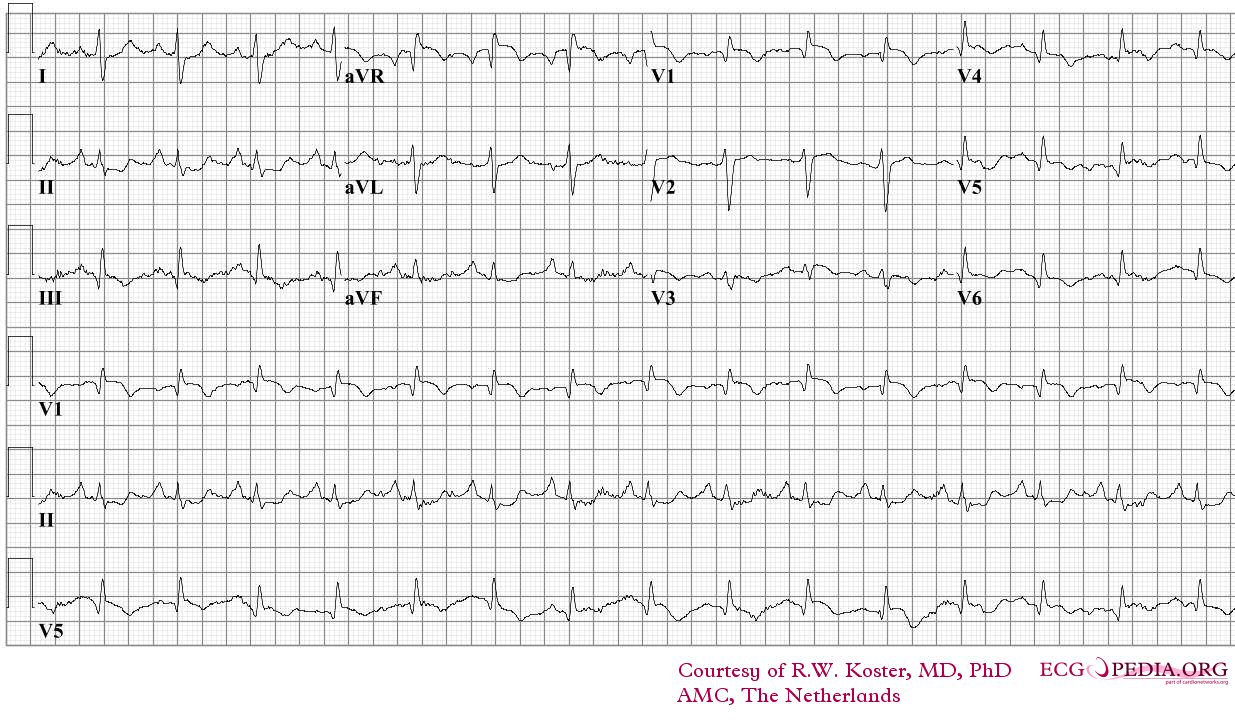
ECG of a patient with pulmonary embolism Image courtesy of ecgpedia
-
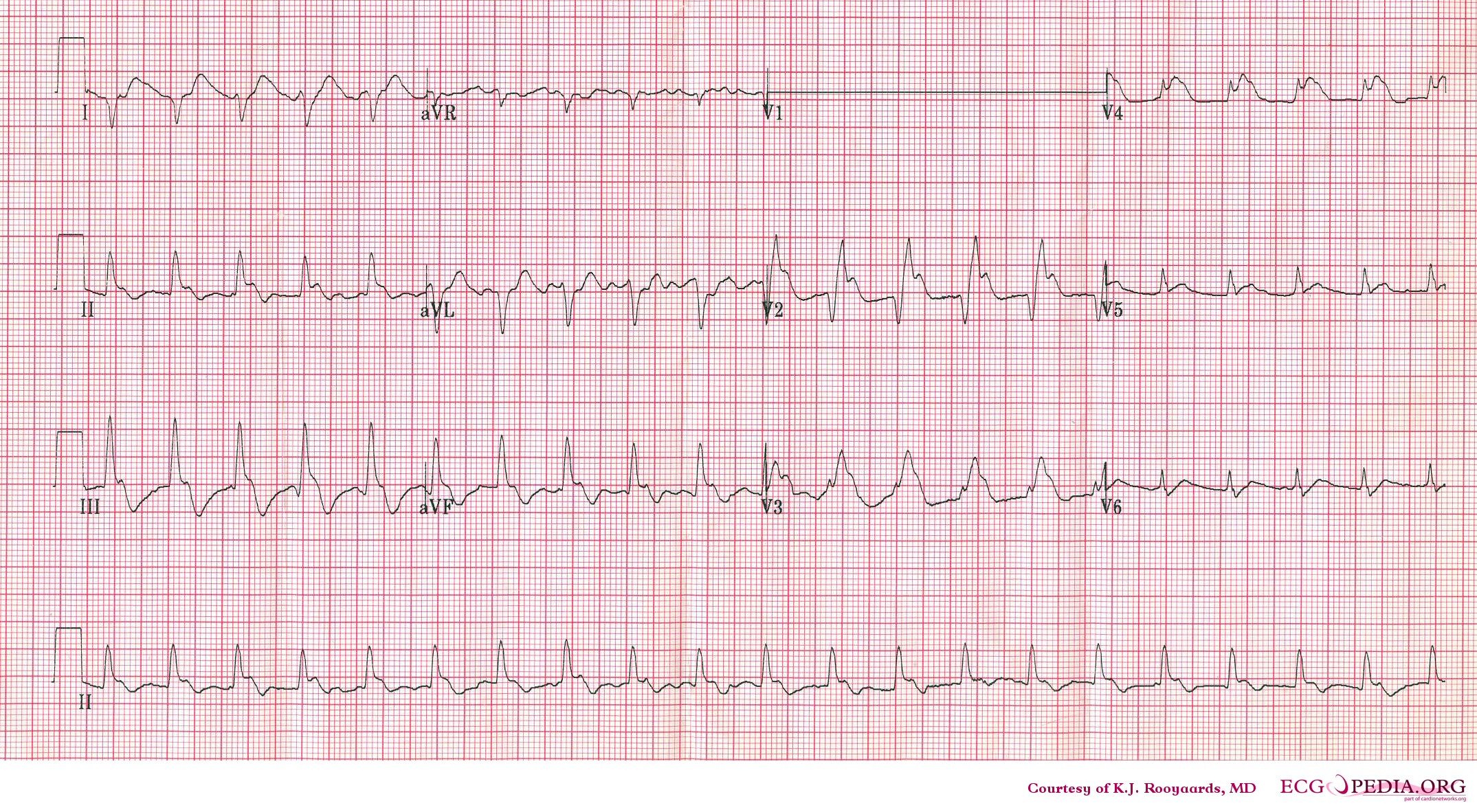
Another example; a patient with pulmonary embolism. Note the tachycardia and right axis.Image courtesy of ecgpedia
-
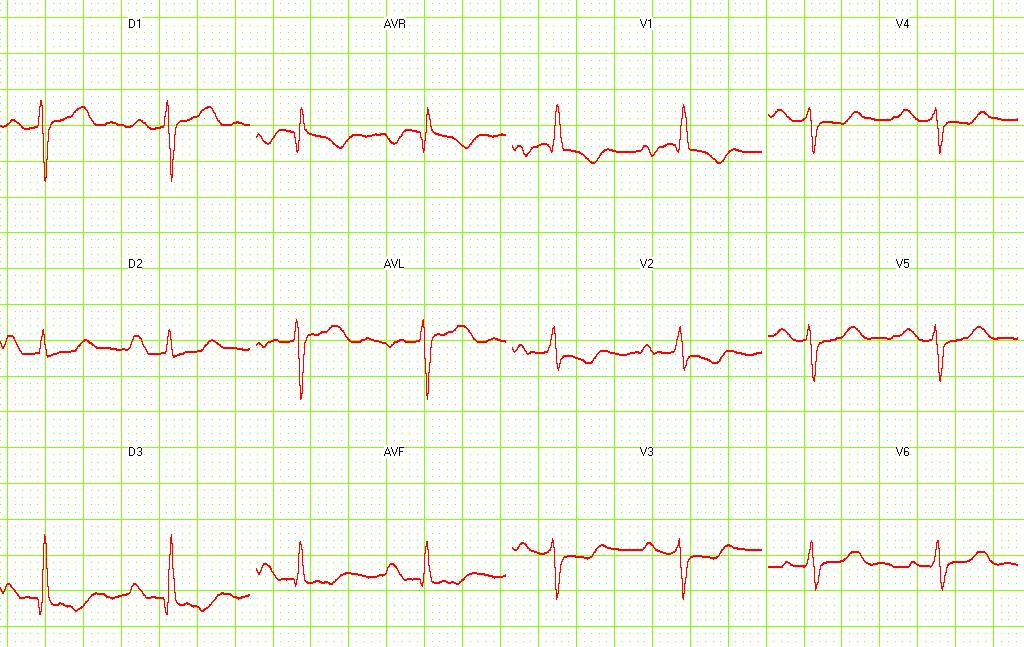
Pulmonary embolism. S1-Q3 and signs of right frontal axis are shown. Image courtesy of Dr Jose Ganseman Dr Ganseman's webpage: An ultimate source of EKG



Echocardiography findings
Approximately 40% of patients with PE have evidence of right heart strain on echocardiography.
In massive and submassive PE, dysfunction of the right side of the heart can be seen on echocardiography, an indication that the pulmonary artery is severely obstructed and the heart is unable to match the pressure. Some studies (see below) suggest that this finding may be an indication for thrombolysis. Not every patient with a (suspected) pulmonary embolism requires an echocardiogram, but elevations in cardiac troponins or brain natriuretic peptide may indicate heart strain and warrant an echocardiogram.[2]
The specific appearance of the right ventricle on echocardiography is referred to as the McConnell sign. This is the finding of akinesia of the mid-free wall but normal motion of the apex. This phenomenon has a 77% sensitivity and a 94% specificity for the diagnosis of acute pulmonary embolism.[3] Some authors suggest that the findings of right ventricular hypokinesis on echo, in association with a positive LENI is virtually pathognomonic for PE.
References
- ↑ McGinn S, White PD. Acute cor pulmonale resulting from pulmonary embolism. J Am Med Assoc 1935;104:1473–1480.
- ↑ Kucher N, Goldhaber SZ (2003). "Cardiac biomarkers for risk stratification of patients with acute pulmonary embolism". Circulation. 108 (18): 2191–4. doi:10.1161/01.CIR.0000100687.99687.CE. PMID 14597581.
- ↑ McConnell MV, Solomon SD, Rayan ME, Come PC, Goldhaber SZ, Lee RT (1996). "Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism". Am. J. Cardiol. 78 (4): 469–73. PMID 8752195.