Osteomyelitis: Difference between revisions
No edit summary |
|||
| Line 122: | Line 122: | ||
<youtube v=X2ShDUfeso0/> | <youtube v=X2ShDUfeso0/> | ||
<br clear="left"/> | <br clear="left"/> | ||
===Pathological Findings=== | |||
[[Image:Osteomyelitis in cancer.jpg|thumb|left|250px|Osteomyelitis in cancer. <br> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology]. ]] | |||
==Osteomyelitis and Chondritis of Vertebrae== | ==Osteomyelitis and Chondritis of Vertebrae== | ||
Revision as of 00:22, 12 April 2009
| Osteomyelitis | |
 | |
|---|---|
| Osteomyelitis of the tibia of a young child. Numerous abscesses in the bone show as radiolucency. | |
| ICD-10 | M86 |
| ICD-9 | 730 |
| DiseasesDB | 9367 |
| MedlinePlus | 000437 |
| eMedicine | ped/1677 |
| MeSH | D010019 |
Template:Search infobox Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please Join in Editing This Page and Apply to be an Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
Osteomyelitis is an infection of bone or bone marrow, usually caused by pyogenic bacteria or mycobacteria. It can be usefully subclassifed on the basis of the causative organism, the route, duration and anatomic location of the infection.
Etiology
| Age group | Most common organisms |
| Newborns (younger than 4 mo) | S. aureus, Enterobacter species, and group A and B Streptococcus species |
| Children (aged 4 mo to 4 y) | S. aureus, group A Streptococcus species, Haemophilus influenzae, and Enterobacter species |
| Children, adolescents (aged 4 y to adult) | S. aureus (80%), group A Streptococcus species, H. influenzae, and Enterobacter species |
| Adult | S. aureus and occasionally Enterobacter or Streptococcus species |
In children, the long bones are usually affected. In adults, the vertebrae and the pelvis are most commonly affected.
Acute osteomyelitis almost invariably occurs in children. When adults are affected, it may be because of compromised host resistance due to debilitation, intravenous drug abuse, infectious root-canaled teeth, or other disease or drugs (e.g. immunosuppressive therapy).
Osteomyelitis is a secondary complication in 1-3% of patients with pulmonary tuberculosis[1]. In this case, the bacteria generally spread to the bone through the circulatory system, first infecting the synovium (due to its higher oxygen concentration) before spreading to the adjacent bone[1]. In tubercular osteomyelitis, the long bones and vertebrae are the ones which tend to be affected[1].
Presentation
Generally, microorganisms may infect bone through one or more of three basic methods: via the bloodstream, contiguously from local areas of infection (as in cellulitis), or penetrating trauma, including iatrogenic causes such as joint replacements or internal fixation of fractures or root-canaled teeth.[1] Once the bone is infected, leukocytes enter the infected area, and in their attempt to engulf the infectious organisms, release enzymes that lyse the bone. Pus spreads into the bone's blood vessels, impairing their flow, and areas of devitalized infected bone, known as sequestra, form the basis of a chronic infection.[1] Often, the body will try to create new bone around the area of necrosis. The resulting new bone is often called an involucrum.[1] On histologic examination, these areas of necrotic bone are the basis for distinguishing between acute osteomyelitis and chronic osteomyelitis. Osteomyelitis is an infective process which encompasses all of the bone (osseous) components, including the bone marrow. When it is chronic it can lead to bone sclerosis and deformity.
In infants, the infection can spread to the joint and cause arthritis. In children, large subperiosteal abscesses can form because the periosteum is loosely attached to the surface of the bone.[1]
Because of the particulars of their blood supply, the tibia, femur, humerus, vertebra, the maxilla, and the mandibular bodies are especially susceptible to osteomyelitis.[2] However, abscesses of any bone may be precipitated by trauma to the affected area. Many infections are caused by Staphylococcus aureus, a member of the normal flora found on the skin and mucous membranes.
Complete Differential Diagnosis of Associated Conditions
- Bacteroides
- Decubitus
- Diabetic angiopathy
- E.Coli
- Gastrointestinal infection
- Klebsiella
- Otitis
- Pneumonia
- Pseudomonas
- Serratia
- Sinusitis
- Skin infection
- Staphylococcus aureus
- Staphylococcus epidermidis
- Streptococcus pyogenes
- Streptococcus pneumoniae
- Tonsilitis
- Urinary tract infection
- Vasculitis [3] [4]
Diagnostic Findings
- Conventional radiographic evaluation of acute osteomyelitis is insufficient because bone changes are not evident for 14–21 days after the onset of infection.
- Although MR imaging is the accepted modality of choice for the early detection and surgical localization of osteomyelitis, in the emergency department, CT is usually more readily available for establishing the diagnosis. [5]
- At CT, features of bacterial osteomyelitis include overlying soft-tissue swelling, periosteal reaction, medullary low-attenuation areas or trabecular coarsening, and focal cortical erosions.
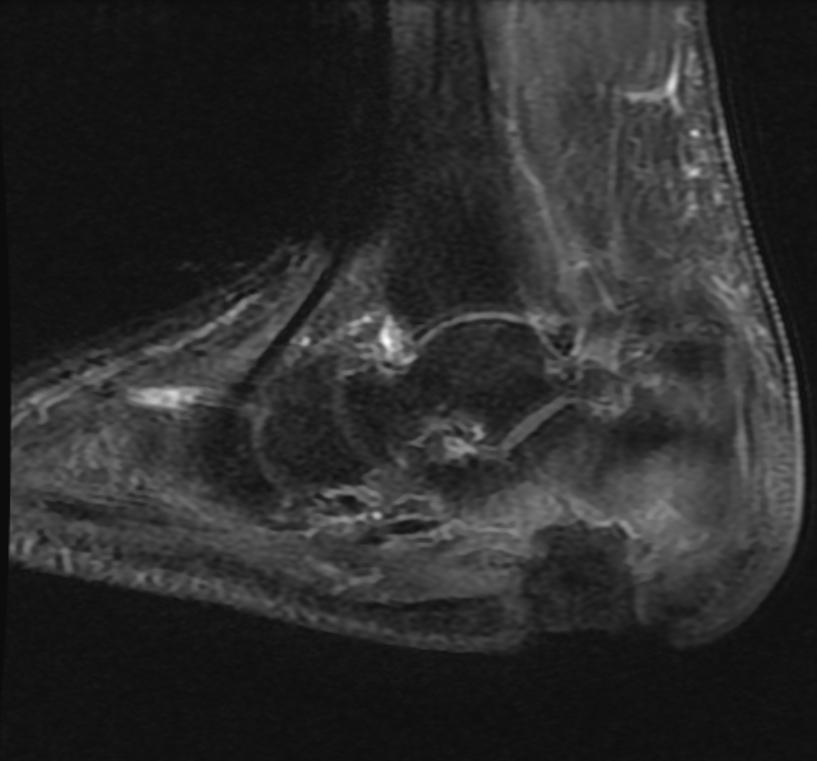
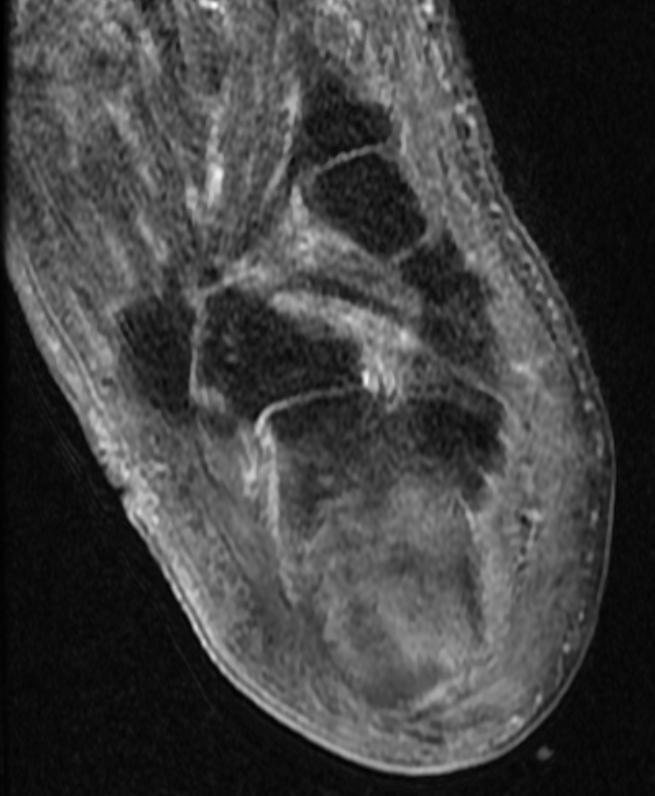
MRI
Patient #1 Extensive calcaneal osteomyelitis. Note soft tissue ulceration and cellulitis
-
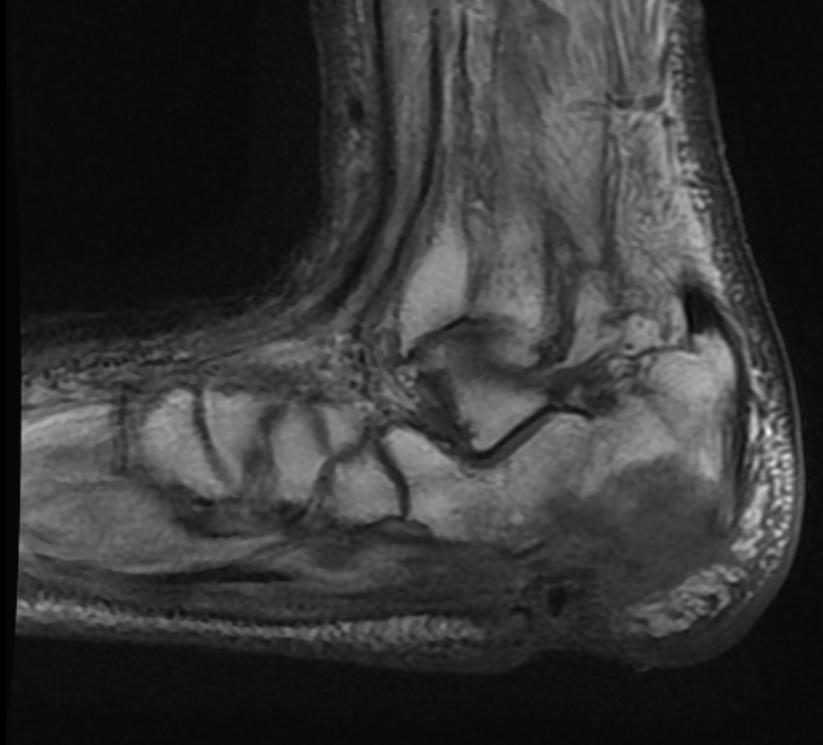
T1
-
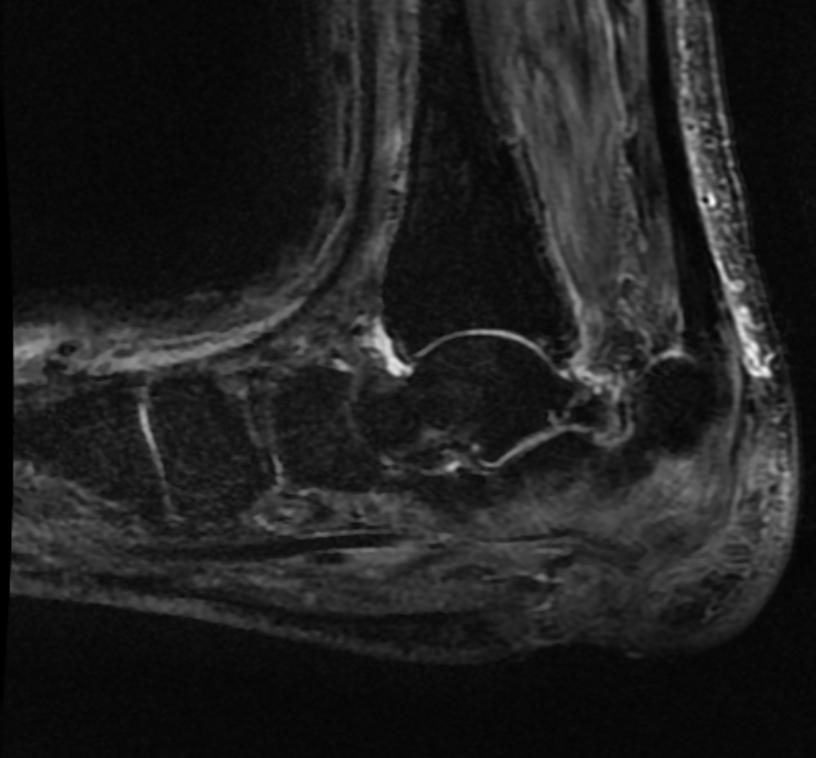
STIR
-
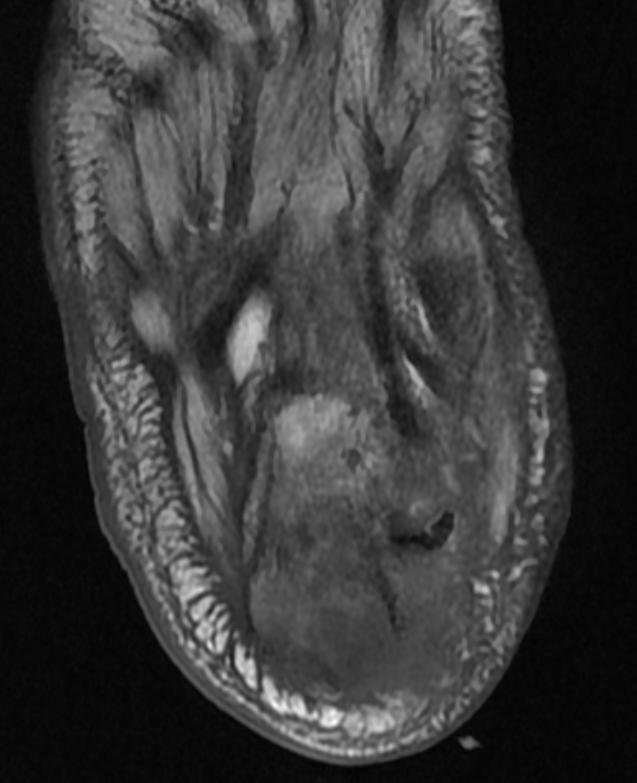
T1
-
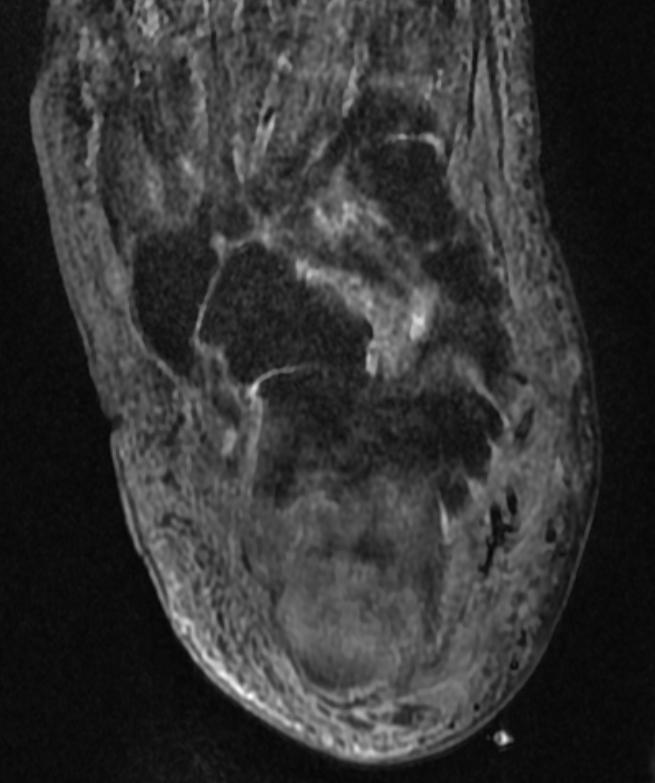
STIR
-
T1 fat sat contrast
-
T1 fat sat contrast






Bone Scan
Patient #2
-
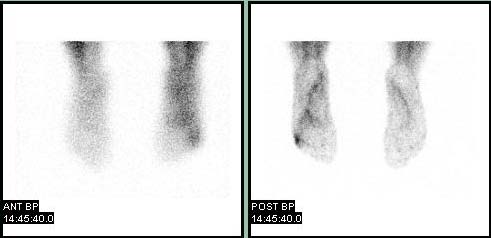
Blood pool
-

Delayed


<youtube v=X2ShDUfeso0/>
Pathological Findings

Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology.
Osteomyelitis and Chondritis of Vertebrae
<youtube v=KTfOwYS1ykY/>
Treatment
Osteomyelitis often requires prolonged antibiotic therapy. IV antibiotics are generally used to combat the infection, with a course lasting a matter of weeks or months. A PICC line or central venous catheter is often placed for this purpose. Osteomyelitis also may require surgical debridement. Severe cases may lead to the loss of a limb. Initial first line antibiotic choice is determined by the patient's history and regional differences in common infective organisms.
Prior to the widespread availability and use of antibiotics, blow fly larvae were sometimes deliberately introduced to the wounds to feed on the infected material, effectively scouring clean.[4]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6
- ↑ King MD, Randall W. (2006-07-13). "Osteomyelitis". eMedicine. WebMD. Retrieved 2007-11-11. Unknown parameter
|coauthors=ignored (help) - ↑ Sailer, Christian, Wasner, Susanne. Differential Diagnosis Pocket. Hermosa Beach, CA: Borm Bruckmeir Publishing LLC, 2002:77 ISBN 1591032016
- ↑ Kahan, Scott, Smith, Ellen G. In A Page: Signs and Symptoms. Malden, Massachusetts: Blackwell Publishing, 2004:68 ISBN 140510368X
- ↑ Laura M. Fayad, John A. Carrino, and Elliot K. Fishman. Musculoskeletal Infection: Role of CT in the Emergency Department. RadioGraphics 2007 27: 1723-1736.
See also
External Links
Additional Resources
Template:Diseases of the musculoskeletal system and connective tissue
de:Osteomyelitis it:Osteomielite nl:Osteomyelitis no:Ostomyelitt