Folliculitis
| Folliculitis | |
 | |
|---|---|
| Folliculitis, Fungal; Pustular Diseases Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology | |
| ICD-10 | L73.8 |
| ICD-9 | xxx |
| DiseasesDB | 31367 |
| eMedicine | DERM/159 |
|
WikiDoc Resources for Folliculitis |
|
Articles |
|---|
|
Most recent articles on Folliculitis Most cited articles on Folliculitis |
|
Media |
|
Powerpoint slides on Folliculitis |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Folliculitis at Clinical Trials.gov Clinical Trials on Folliculitis at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Folliculitis
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Folliculitis Discussion groups on Folliculitis Patient Handouts on Folliculitis Directions to Hospitals Treating Folliculitis Risk calculators and risk factors for Folliculitis
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Folliculitis |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Jesus Rosario Hernandez, M.D. [2].
Overview
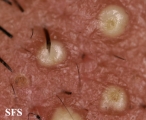
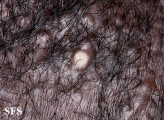
Folliculitis is the inflammation of one or more hair follicles. The condition may occur anywhere on the skin.
Classification
- Folliculitis can be classified in a variety of ways based on the:
- Depth of the involvement(superficial vs deep)
- Underlying etiological agent(infectious vs non infectious)
- chronicity of the condition( acute vs chronic/recurrent)
- Non-infectious variant of the folliculitis include Pseudofolliculitis barbae,Eosinophilic folliculitis ,drug induced acneiform folliculitis,Folliculitis decalvans or tufted folliculitis and Acne keloidalis nuchae or Folliculitis keloidalis to mention a few.
Pathophysiology
- The pathogenesis of folliculitis depends upon the etiological agent.It can be caused by an infection (bacterial, viral, fungal, or parasitic) or have a noninfectious etiology, as the result of follicular trauma, inflammation, occlusion,scratch around the hair follicle or topical application of steroids may induce the infection and subsequently inflammation of the hair follicle.
- Although the cause of Esinophilic Folliculitis is unknown. A variety of microorganisms have been implicated, including the mite Demodex, the yeast Pityrosporum, and bacteria. An autoimmune process has also been investigated.
- On microscopic pathology, superficial folliculitis characterized by neutrophic infiltration confined to the infundibulum of the hair follicle, however in deep folliculitis it extend to the deeper portion of the follicle and dermis.Infiltrate initially consists of neutrophils, later becomes mixed with lymphocytes and macrophages.Chronic cases shows granulomatous inflammation with giant cells containing keratin and fragmented hair. Suppurative folliculitiis often heals spontaneously, some longstanding cases may progress to the formation of granulomas or fibrosis with evident clinical scarring.
Clinical Features
Differentiating Folliculitis from other Diseases
- Folliculitis must be differentiated from following diseases:
- Acne vulgaris
- Acne rosasea
- Periorofacial dermatitis
- Acneform Eruptions
- Hidraadenitis suppurativa
- Rosacea
- Transient acantholytic dermatosis
- Insect bite
- Papular urticaria
- Milia
- Contact dermatitis
Epidemiology and Demographics
- Superficial Folliculitis is although commonly seen but the exact incidence is not known.It is difficult to determine the incidence of the folliculitis as majority of the people affected with it never seek medical attention.
Age
- Patients of all age groups may develop Folliculitis.
- Superficial Folliculitis and Hot tub folliculitis is more commonly observed among adults than children.
- Demodex folliculitis is more commonly seen in adults however it also has been implicated in facial pustules and papules in children.[1]
Gender
- Superficial Folliculitis affects men and women equally.
- Males are more commonly affected with Herpes folliculitis and Pityrosporum folliculitis[2] than females.
- Eosinophilic Folliculitis has been seen in HIV-infected men, women, and children. [3][4][5]
Race
- There is no racial predilection for Folliculitis however Pseudofolliculitis barbae usually affects individuals of the African descent.
Causes
Most carbuncles and furuncles and other cases of folliculitis develop from Staphylococcus aureus.
Folliculitis starts when hair follicles are damaged by friction from clothing, blockage of the follicle, or shaving. In most cases of folliculitis, the damaged follicles are then infected with the bacteria Staphylococcus (staph).[6]
Iron deficiency anemia is sometimes associated with chronic cases
- Sycosis barbae or barber's itch is a staph infection of the hair follicles in the bearded area of the face, usually the upper lip. Shaving aggravates the condition.
- Tinea barbae is similar to barber's itch, but the infection is caused by the fungus T._rubrum.
- Pseudofolliculitis barbae is a disorder occurring primarily in men of African descent. If curly beard hairs are cut too short, they may curve back into the skin and cause inflammation.
- Hot tub folliculitis is caused by the bacteria Pseudomonas aeruginosa often found in new hot tubs. The folliculitis usually occurs after sitting in a hot tub that was not properly cleaned before use. Symptoms are found around the body parts that sit in the hot tub -- typically the legs, hips and buttocks and surrounding areas. Symptoms are typically amplified around regions that were covered by wet clothing, such as bathing suits.
- Drug Side Effect: Betamethasone valerate, Betamethasone dipropionate, Clocortolone pivalate, Desoximetasone, Diflorasone, Sorafenib, Mometasone furoate
Risk Factors
- Common risk factors in the development of Folliculitis are:
- Frequent shaving against the direction of the hair growth
- Immunosuppresion
- Presence of dermatosis
- Long term oral antibiotic use
- Hot tub bath
- tight clothing
- exposure of certain solvents
- poor hygiene
- friction
- obesity
- Diabetes
- HIV,late stage esp with low CD4 cell count
- Prolonged used of topical steriods
- Exposure to the hot humid temperature
- Patients treated with EGFR inhibitors[7]
- post vaccination esp after the small pox and anthrax vaccine[8][9]
Natural History, Complications and Prognosis
- The majority of patients with folliculitis remain asymptomatic however sometimes it presents with pruritic or painful erythematous papule or pustule that is a self limiting entitiy.
- If left untreated,occasionally folliculitis may progress to develop furuncle. Multiple furuncles can coalesce to form carbuncles that become painful and fluctuant after several days.Sometimes rupture do occur with the discharge of pus and necrotic material.
- Common complications of folliculitis include cellulitis, furunculosis, scarring, sinus tract formation, permanent hair loss and recurrence in some cases.
- Sometimes,in dark skin people, folliculitis often resolve with post-inflammatory hyperpigmentation, which can take months to years to fade completely.
- Prognosis is generally excellent if the causative agent is accurately identified and treated.
Diagnosis
Folliculitis is a clinical diagnosis so diagnosis is usually based on history and physical examination.
Symptoms
- Folliculitis is usually asymptomatic, benign and self limiting condition.
- Symptoms of folliculitis may include the following:
- Clusters of small red bumps or white-headed pimples present around hair follicle
- Itchy, burning and painful skin lesions.
- Pus-filled blisters that may break open and crust over
Physical Examination
- Patients with folliculitis usually appear generally well.
- Physical examination may be remarkable for:
- multiple erythematous, folliculocentric papules and pustules in the hair-bearing regions,usually less than 5 mm in diameter.
- Superficial folliculitis presents with multiple small papules and pustules on an erythematous base, with each papule or pustule pierced by a central hair.
- Deep folliculitis presents as tender plaques and nodules overlying the erythema and induration, usually heal by scarring.
- Pyrexia and systematic manifestation in deeper or immunocompromised patients
- [finding 5]
- [finding 6]
Laboratory Findings
- Folliculitis is a clinical diagnosis so the laboratory tests are generally done in cases of treatment resistance.
- CBC suggestive of leukocytosis and eosinophilia, with elevated immunoglobulin E levels in patients with eosinophilic folliculitis.
- RBS can be done in cases of the recurrent folliculitis.
- HIV testing can be done in suspected cases of esinophilic folliculitis.
- Gram stain and culture can be done when bacterial etiology is suspected.Gram stain usually shows gram-positive cocci, and culture grows S aureus. Pseudomonas species can be cultured from the pustules of hot tub folliculitis.
- In chronic cases,nasal culture of family members can be done to look for S aureus colonization.
- KOH preparation, fungal culture, or both can be helpful for diagnosing dermatophyte infections however skin biopsy is best to visualise Pityrosporum yeast forms in cases of Pityrosporum folliculitis.
- Viral culture, polymerase chain reaction (PCR), or immunofluorescence testing helps to confirm the diagnosis if herpes folliculitis is suspected.[10]
Imaging Findings
- There are no imaging study findings associated with Folliculitis.
Other Diagnostic Studies
- Folliculitis may also be diagnosed using skin biopsy and histology.
- Findings on biopsy and histology varies depending upon the causative agent.
Treatment
Medical Therapy
Folliculitis is a self limiting condition ,if uncomplicated. Complicated and recurrent cases requires treatment targeted against the specific organism.
- Due to increased resistance seen with fusidic acid, uncomplicated bacterial folliculitis (staph aureus) folliculitis is best treated with topical mupirocin and clidamycin.[11]However complicated,recurrent and folliculitis resistant to the topical treatment can be managed with 7-10 days course of oral antibiotics.
- Psedomonas folliculitis can be treated with oral ciprofloxocin if the patient is immunocompromise and lesions are persistent.
- Gram negative folliculitis is usually seen due to complication of chronic antibiotic use so best managed by discontinuing the implicated antibiotic and administering oral trimethoprim-sulfamethoxazole.
- Esinophilic folliculitis usually reponds well to the indomethacin treatemnt.
- Fungal folliculitis can be treated with oral antifungal agents such as fluconazole and itraconazole.
- Viral folliculitis responds well to valacyclovir, famciclovir, or acyclovir.
- Antiparasitic agents, such as permethrin and oral ivermectin, can be used for Demodex folliculitis
Surgery
- Surgery is the mainstay of therapy for [disease name].
- [Surgical procedure] in conjunction with [chemotherapy/radiation] is the most common approach to the treatment of [disease name].
- [Surgical procedure] can only be performed for patients with [disease stage] [disease name].
Prevention
- Effective measures for the primary prevention of folliculitis include:
- Maintain good personal hygiene including regular bathing with antibacterial soaps and washing hands.
- Avoidance of the precipitating causes like wearing tight fitted clothing.
- Avoid sharing razors with others.
- Avoiding unsanitary hot tubs and pools.
- Daily decontamination of personal items.
- A five-day course of topical mupirocin ointment in the nares and daily chlorhexidine body washes can be used as decolonization regimen.
- Once diagnosed and successfully treated, patients with folliculitis are followed-up after 2 weeks to check the response of the treatment.
Gallery
Extremities








Folliculitis Of Barbae
-

Folliculitis Of Barbae.
With permission from Dermatology Atlas. -
Folliculitis Of Barbae.
With permission from Dermatology Atlas. -

Folliculitis Of Barbae.
With permission from Dermatology Atlas.



Folliculitis cheloidalis
-

Folliculitis Cheloidalis.
Used with permission of Dermatology Atlas -

Folliculitis Cheloidalis.
Used with permission of Dermatology Atlas -

Folliculitis Cheloidalis.
Used with permission of Dermatology Atlas -

Folliculitis Cheloidalis.
Used with permission of Dermatology Atlas -

Folliculitis Cheloidalis.
Used with permission of Dermatology Atlas -

Folliculitis Cheloidalis.
Used with permission of Dermatology Atlas -
Folliculitis Cheloidalis.
Used with permission of Dermatology Atlas







Treatment
- Topical antiseptic treatment is adequate for most cases
- Some patients may benefit from systemic flucloxacillin
References
- ↑ Brown M, Hernández-Martín A, Clement A, Colmenero I, Torrelo A (2014). "Severe demodexfolliculorum-associated oculocutaneous rosacea in a girl successfully treated with ivermectin". JAMA Dermatol. 150 (1): 61–3. doi:10.1001/jamadermatol.2013.7688. PMID 24284904.
- ↑ Poli F (2012). "Differential diagnosis of facial acne on black skin". Int J Dermatol. 51 Suppl 1: 24–6, 27–9. doi:10.1111/j.1365-4632.2012.05559.x. PMID 23210948.
- ↑ Basarab T, Russell Jones R (1996). "HIV-associated eosinophilic folliculitis: case report and review of the literature". Br J Dermatol. 134 (3): 499–503. PMID 8731676.
- ↑ Ramdial PK, Morar N, Dlova NC, Aboobaker J (1999). "HIV-associated eosinophilic folliculitis in an infant". Am J Dermatopathol. 21 (3): 241–6. PMID 10380045.
- ↑ Hayes BB, Hille RC, Goldberg LJ (2004). "Eosinophilic folliculitis in 2 HIV-positive women". Arch Dermatol. 140 (4): 463–5. doi:10.1001/archderm.140.4.463. PMID 15096375.
- ↑ Laureano AC, Schwartz RA, Cohen PJ (2014). "Facial bacterial infections: folliculitis". Clin Dermatol. 32 (6): 711–4. doi:10.1016/j.clindermatol.2014.02.009. PMID 25441463.
- ↑ Bachet JB, Peuvrel L, Bachmeyer C, Reguiai Z, Gourraud PA, Bouché O; et al. (2012). "Folliculitis induced by EGFR inhibitors, preventive and curative efficacy of tetracyclines in the management and incidence rates according to the type of EGFR inhibitor administered: a systematic literature review". Oncologist. 17 (4): 555–68. doi:10.1634/theoncologist.2011-0365. PMC 3336835. PMID 22426526.
- ↑ Oh RC (2005). "Folliculitis after smallpox vaccination: a report of two cases". Mil Med. 170 (2): 133–6. PMID 15782834.
- ↑ Greenberg RN, Schosser RH, Plummer EA, Roberts SE, Caldwell MA, Hargis DL; et al. (2004). "Urticaria, exanthems, and other benign dermatologic reactions to smallpox vaccination in adults". Clin Infect Dis. 38 (7): 958–65. doi:10.1086/382360. PMID 15034827.
- ↑ Böer A, Herder N, Winter K, Falk T (2006). "Herpes folliculitis: clinical, histopathological, and molecular pathologic observations". Br J Dermatol. 154 (4): 743–6. doi:10.1111/j.1365-2133.2005.07118.x. PMID 16536821.
- ↑ Williamson DA, Monecke S, Heffernan H, Ritchie SR, Roberts SA, Upton A; et al. (2014). "High usage of topical fusidic acid and rapid clonal expansion of fusidic acid-resistant Staphylococcus aureus: a cautionary tale". Clin Infect Dis. 59 (10): 1451–4. doi:10.1093/cid/ciu658. PMID 25139961.