Aortic dissection pathophysiology: Difference between revisions
No edit summary |
|||
| Line 127: | Line 127: | ||
[[Category:Up-To-Date]] | [[Category:Up-To-Date]] | ||
[[Category:Up-To-Date cardiology]] | [[Category:Up-To-Date cardiology]] | ||
[[Category:Best pages]] | |||
Revision as of 14:35, 2 February 2013
|
Aortic dissection Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Special Scenarios |
|
Case Studies |
|
|
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Aortic dissection begins as a tear in the aortic wall in > 95% of patients. The tear is usually transverse, extends through the intima and halfway through the media and involves ~50% of the aortic circumference. Two thirds of dissections originate in the ascending aorta, and 20% are in the proximal descending aorta.
Pathophysiology
Normal Anatomy of the Aorta
As with all other arteries, the aorta is made up of three layers. The layer that is in direct contact with the flow of blood is the tunica intima, commonly called the intima. This layer is made up of mainly endothelial cells. Just deep to this layer is the tunica media, known as the media. This middle layer is made up of smooth muscle cells and elastic tissue. The outermost layer (furthest from the flow of blood) is known as the tunica adventitia or the adventitia. This layer is composed of connective tissue.

Initial Intimal Tear
- Aortic dissection begins as a tear in the aortic wall in > 95% of patients.
- It is usually transverse, extends through the intima and halfway through the media and involves ~50% of the aortic circumference.
Location of Dissections
- The initial tear is usually within 100 mm of the aortic valve.
- 65% of dissections originate in the ascending aorta, distal to the aortic valve and coronary ostia
- 10% arise in the transverse aortic arch
- 20% in the proximal descending aorta
- 5% in the more distal descending aorta
Propagation of the Intimal Tear
In an aortic dissection, blood penetrates the intima and enters the media layer. The high pressure rips the tissue of the media apart, allowing more blood to enter. This can propagate along the length of the aorta for a variable distance, dissecting either towards or away from the heart or both.
Once a tear develops, blood then passes into the media, and a false lumen is dissected in the outer layer of aortic media involving ~50% of the aortic circumference. This false lumen can enlarge, and compress the true lumen, as well as extend proximally or distally and occlude aortic branches. For some unknown reason, the right lateral wall of the ascending aorta is the most common site for dissection. The right coronary artery can become occluded as a result of this propagation.
Separating the false lumen from the true lumen is a layer of intimal tissue. This tissue is known as the intimal flap. As blood flows down the false lumen, it may cause secondary tears in the intima. Through these secondary tears, the blood can re-enter the true lumen.
Risk Factors for an Intimal Tear
While it is not always clear why an intimal tear may occur, quite often it involves degeneration of the collagen and elastin that make up the media. This is known as cystic medial necrosis and is most commonly associated with Marfan syndrome and is also associated with Ehlers-Danlos syndrome. Aging, atherosclerosis, diabetes, hypertension and trauma are common risk factors for aortic dissection. Uncommon risk factors include bicuspid aortic valve, cocaine, coarctation of the aorta, cystic medial necrosis, Ehlers-Danlos syndrome, giant cell arteritis, heart surgery, Marfan’s syndrome, Pseudoxanthoma elasticum, Turner's syndrome, tertiary syphilis and the third trimester of pregnancy.
Aortic Dissection in the Absence of an Intimal Tear
In about 13% of aortic dissections, there is no evidence of an intimal tear. It is believed that in these cases the inciting event is an intramural hematoma (caused by hemorrhage within the media). Since there is no direct connection between the true lumen and the false lumen in these cases, it is difficult to diagnose an aortic dissection by aortography if the etiology is an intramural hematoma. An aortic dissection secondary to an intramural hematoma should be treated the same as one caused by an intimal tear.
An aortic intramural hematoma can form when the vasa vasorum ruptures into the aortic wall. This is distinguished from dissection by the lack of an intimal tear. This disorder parallels aortic dissection in terms of prognosis when the ascending aorta or aortic arch is involved, and rapid surgical intervention is indicated. Involvement of the descending aorta, however, carries a better prognosis than dissection, and outcome tends to be similar with medical or surgical therapy.
Gross Pathology Images of Aortic dissection
-

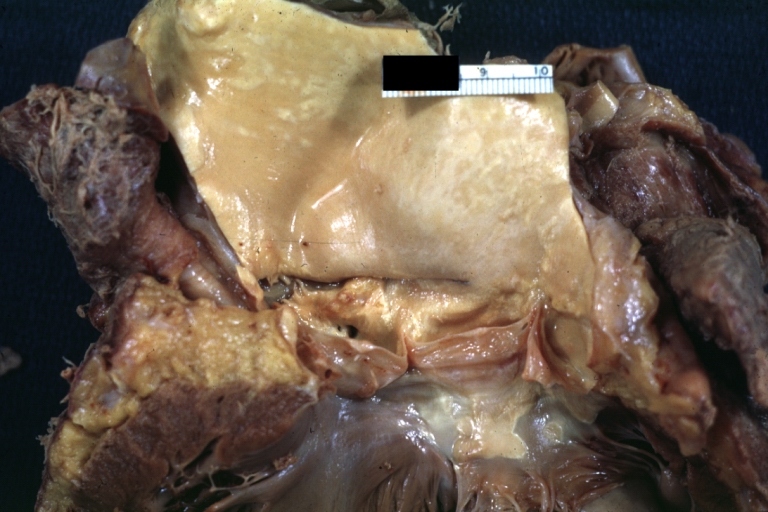
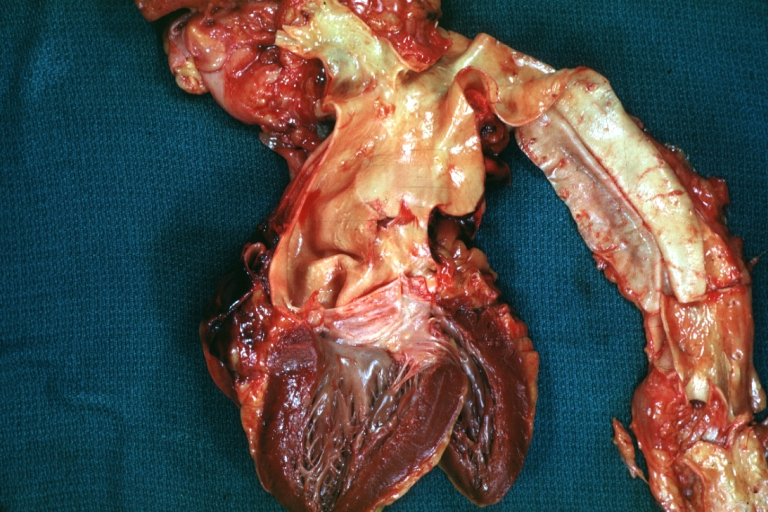
Dissecting Aneurysm: Gross fixed tissue external view of heart aortic arch and descending aorta showing dilated first and second portion of arch from anterior projection.
-
-



-
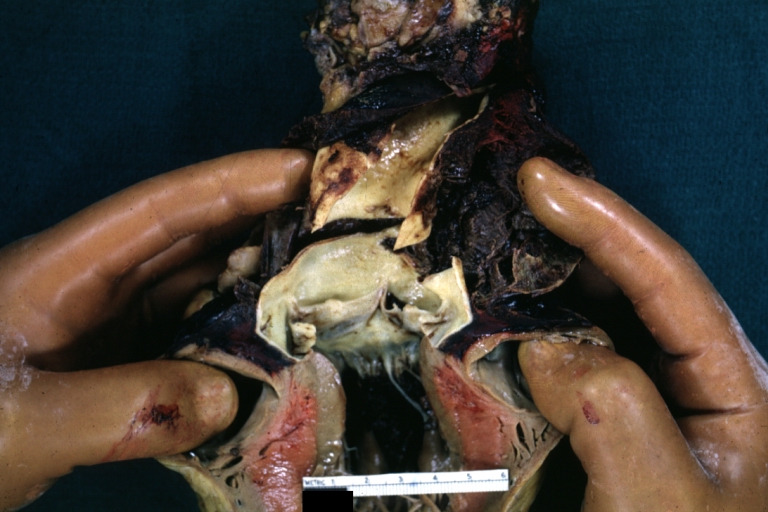
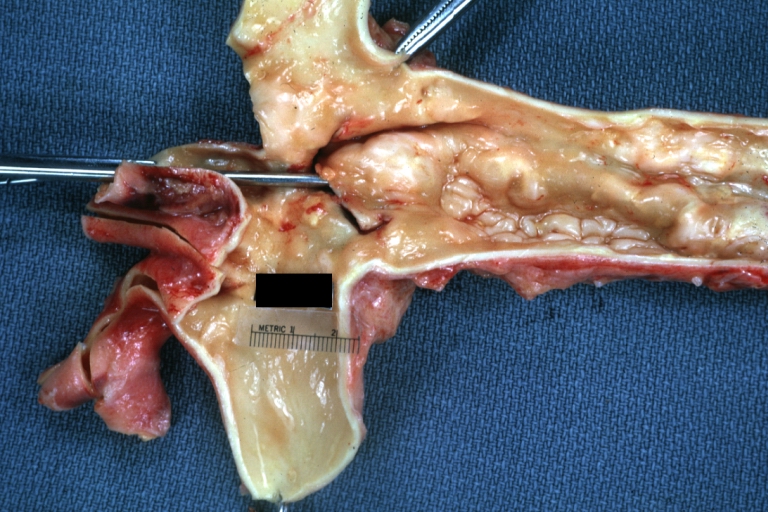
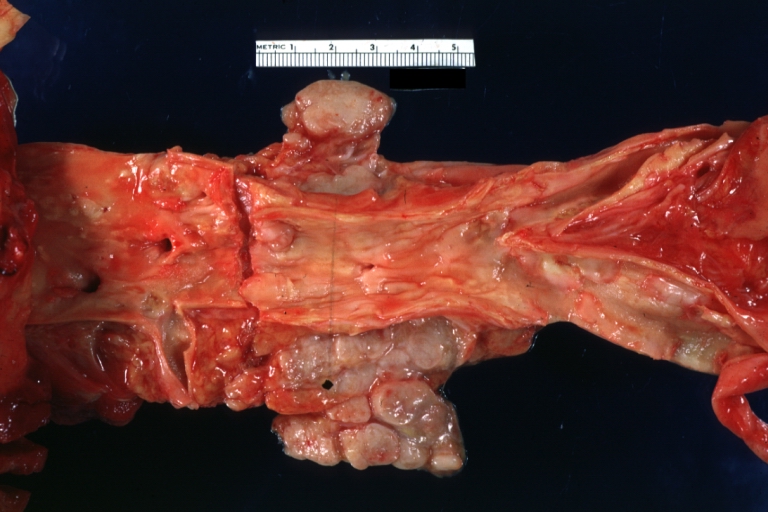
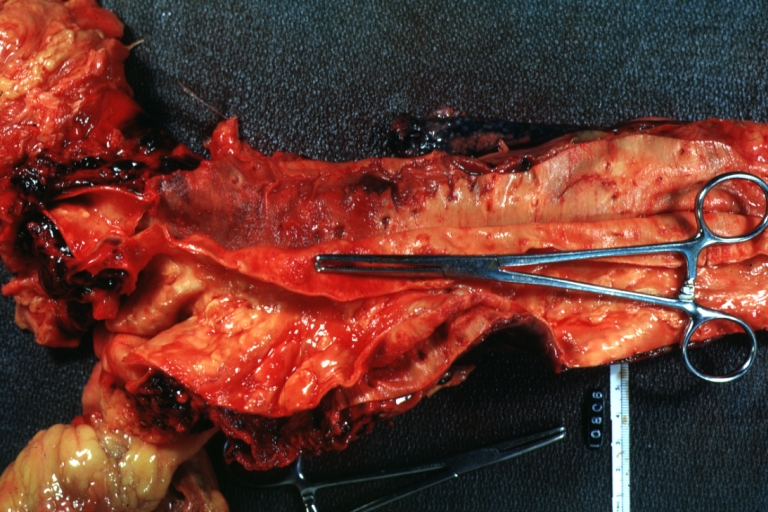
Dissecting Aneurysm: Gross very good example dissected channel has been opened.
-
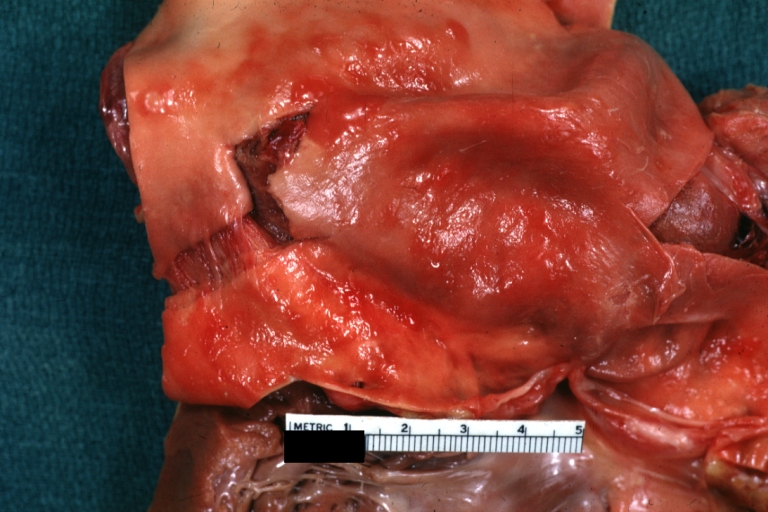
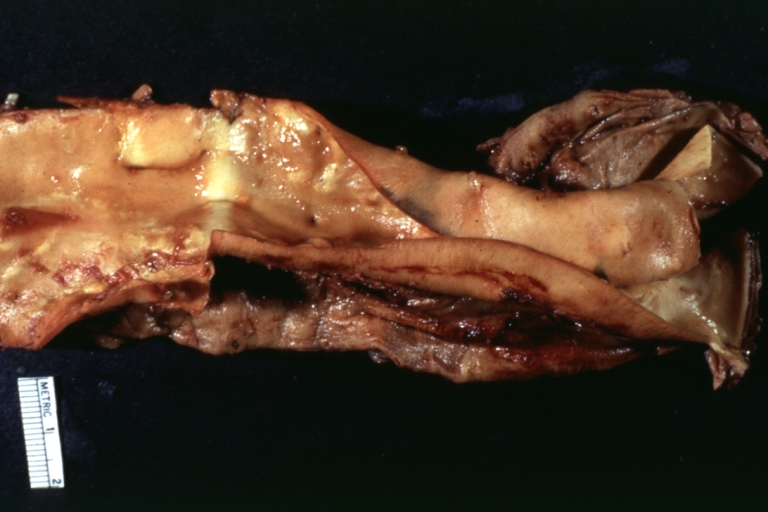
Dissecting Aneurysm: Gross external view good appearance from adventitia.
-
Dissecting Aneurysm: Gross opened false channel.



-
Dissecting Aneurysm: Gross good example dissection beginning at third portion aortic arch.
-
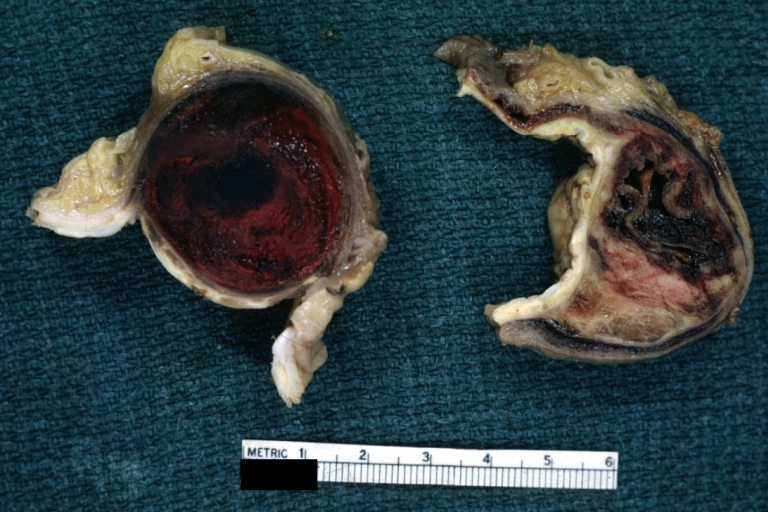
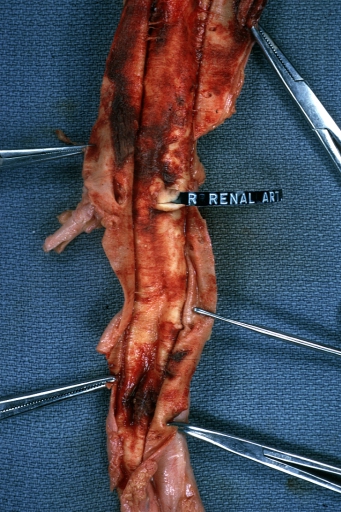
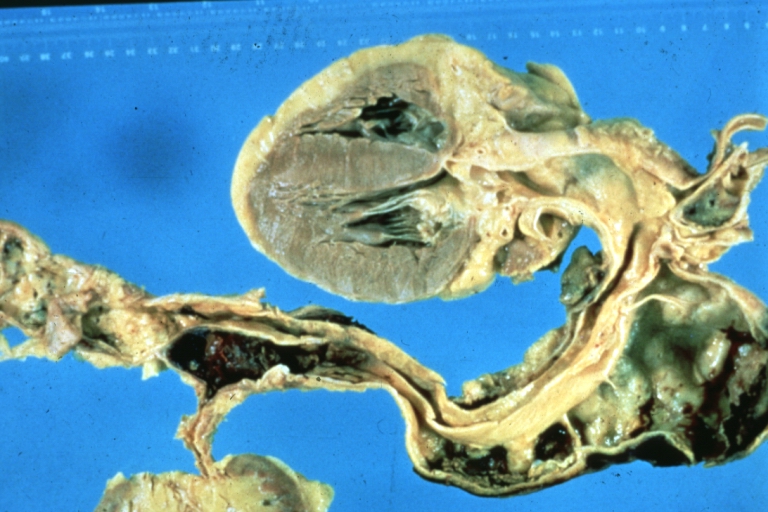
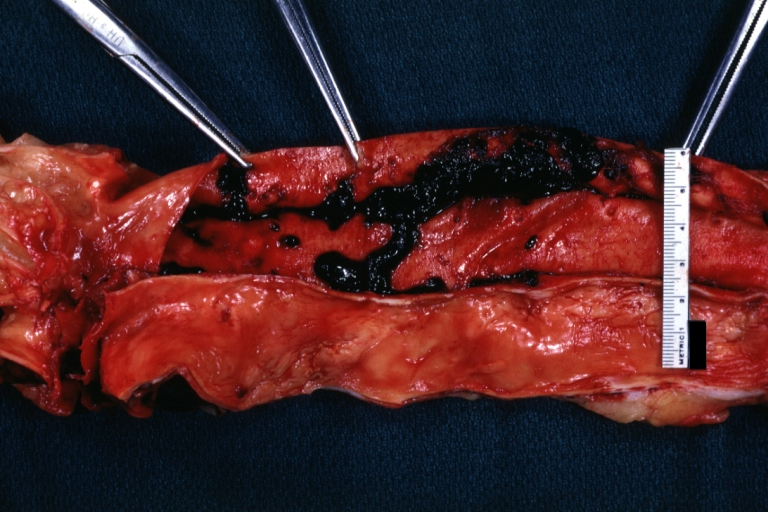
Dissecting Aneurysm: Gross cross sections showing thrombus in false lumen. True lumen has been opened longitudinally.
-
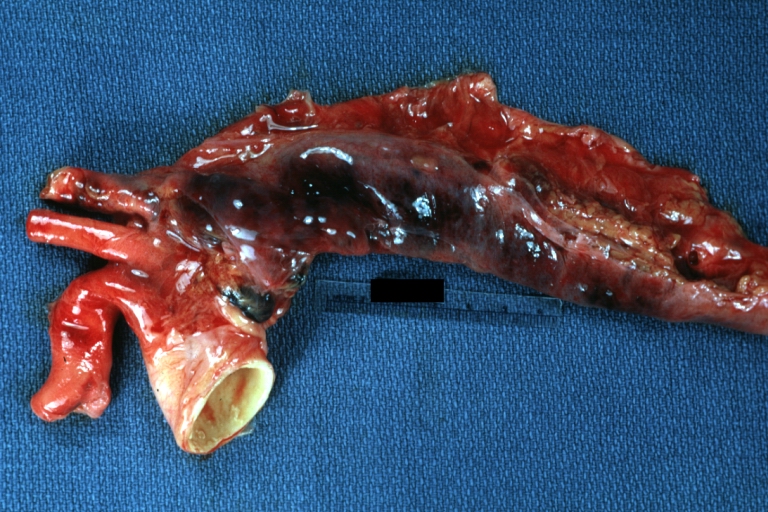
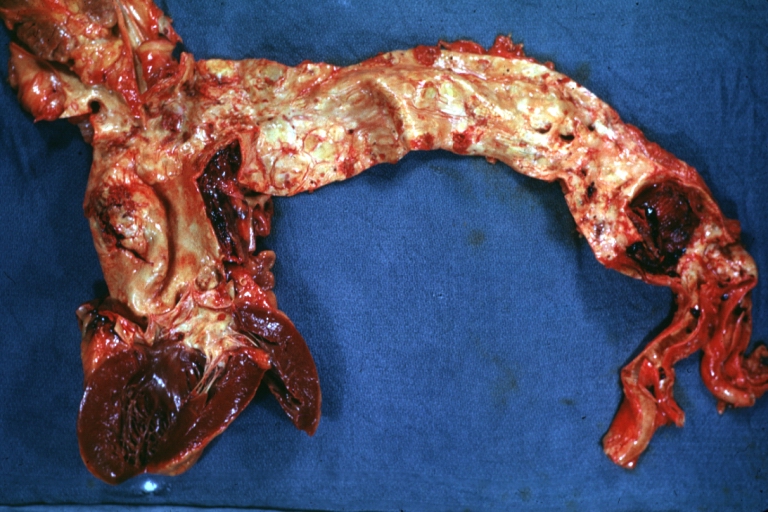
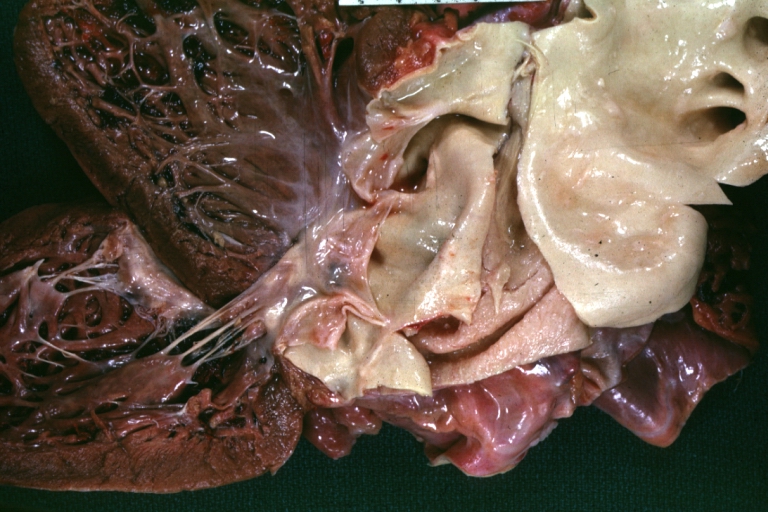
Dissecting Aneurysm: Gross shows origin just above aortic valve false channel shown in descending thoracic aorta (very good example).



-
Dissecting Aneurysm: Gross, an excellent example, starting just above the aortic valve with reflection of aorta to show the dissection tract and some thrombus
-
Dissecting Aneurysm: Gross shows dilated aorta with extensive atherosclerosis dissection is seen, a small abdominal aorta atherosclerotic aneurysm is present good for association of dilation with dissection
-
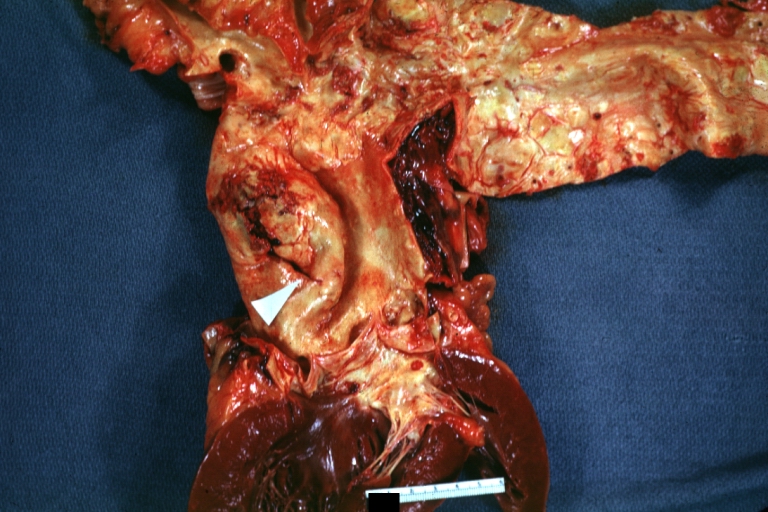
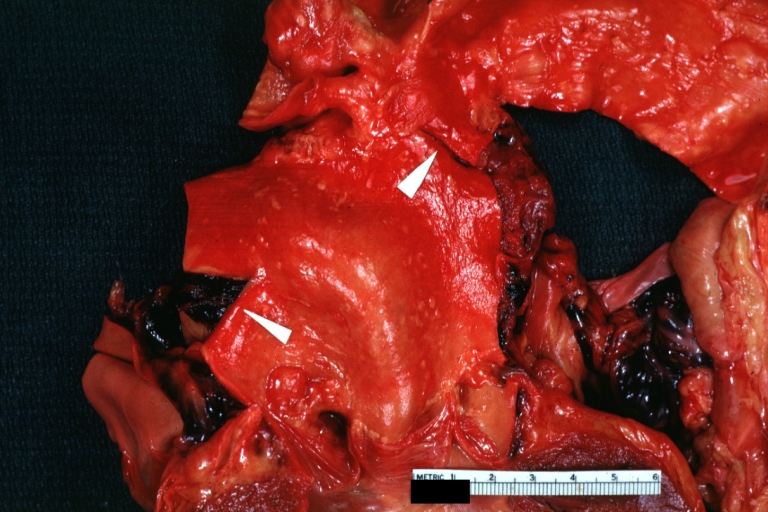
Dissecting Aneurysm: Gross arrow points to start of dissection in first portion aortic arch good but not the best example shows dilation
-

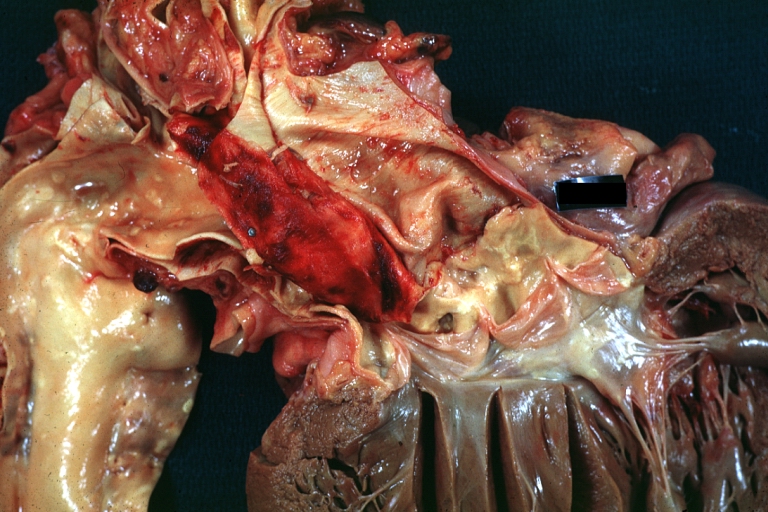
Dissecting Aneurysm: Gross, very good to show start of dissection above aortic valve and blood in false channel.




-
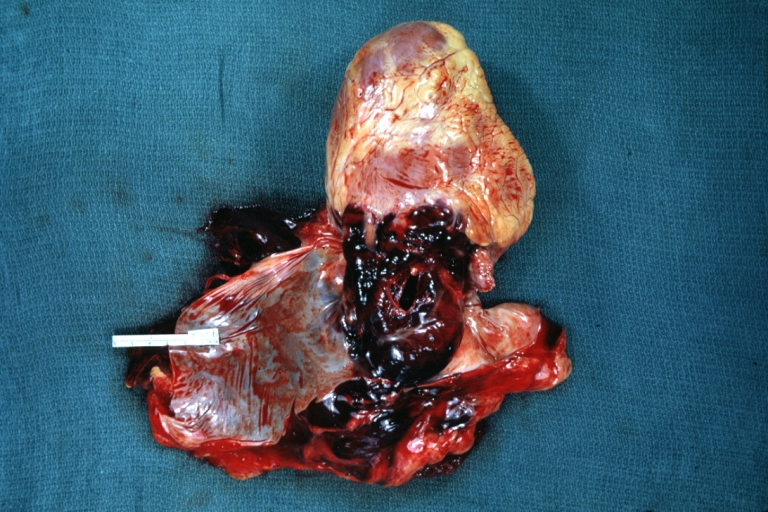
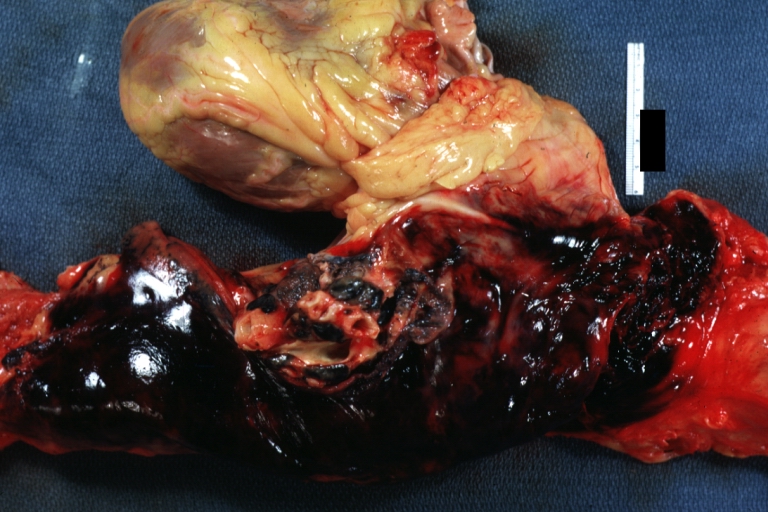
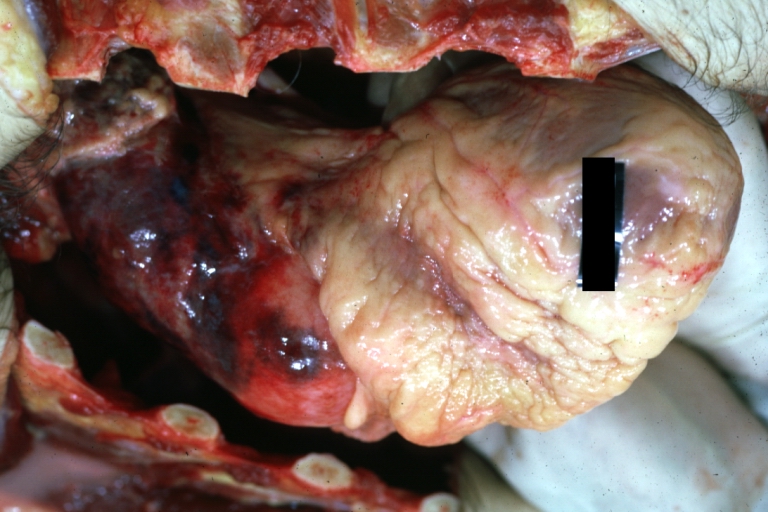
Dissecting Aneurysm: Gross, heart with root of aorta to show hemorrhage into pericardium (a very good example).
-
-

-
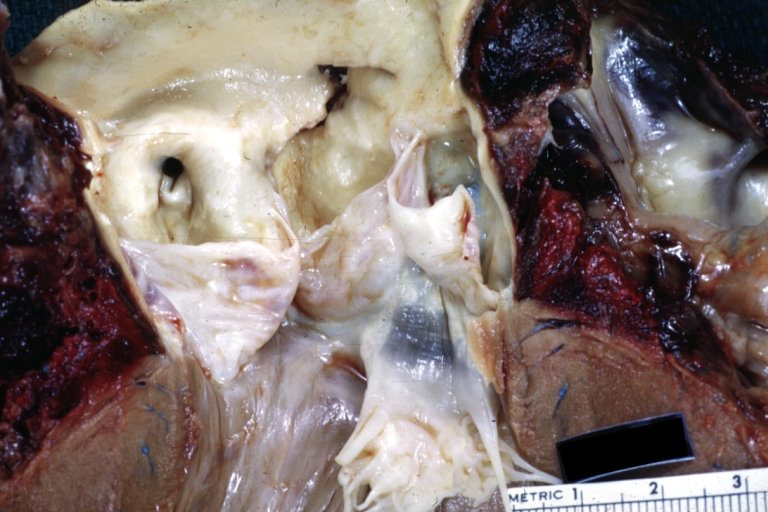
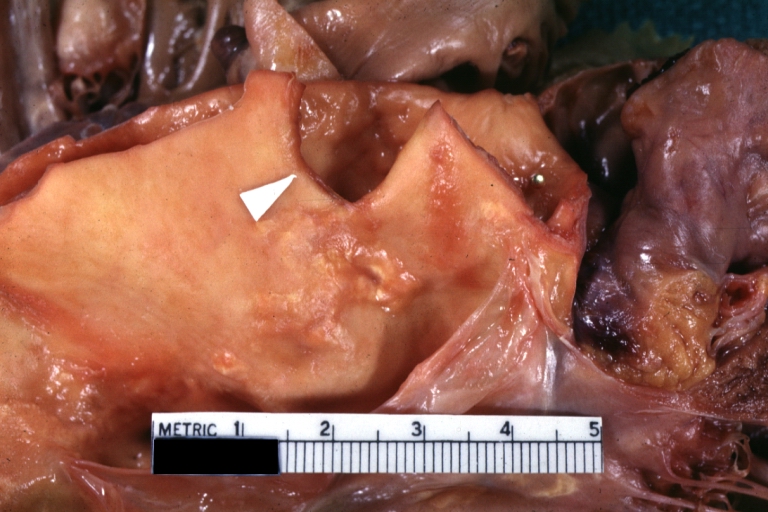
Dissecting Aneurysm: Gross good example angular tear above aortic valve.




-

Dissecting Aneurysm: Gross good example of typical angular tear above aortic valve.
-
Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch
-
Dissecting Aneurysm: Gross, rather well shown dissection in first portion of the aortic arch
-




-
Dissecting Aneurysm: Gross, external view, an excellent example
-

Dissecting Aneurysm: Gross, Type I shows false channel
-
Dissecting Aneurysm: Gross, opened to show false channel (good example)
-
Dissecting Aneurysm: Gross, large tear in first portion of aortic arch, annuloaortic ectasia




-

Dissecting Aneurysm: Gross, coagulum of blood in false channel
-
Dissecting Aneurysm: Gross, aortic valve area dissection (well shown, typical lesion)
-
Dissecting Aneurysm: Gross, external view of heart and first portion of aortic arch, annuloaortic ectasia, hemorrhage beneath adventitia is evidence of dissection
-
Dissecting Aneurysm in a patient with Marfan's syndrome




-

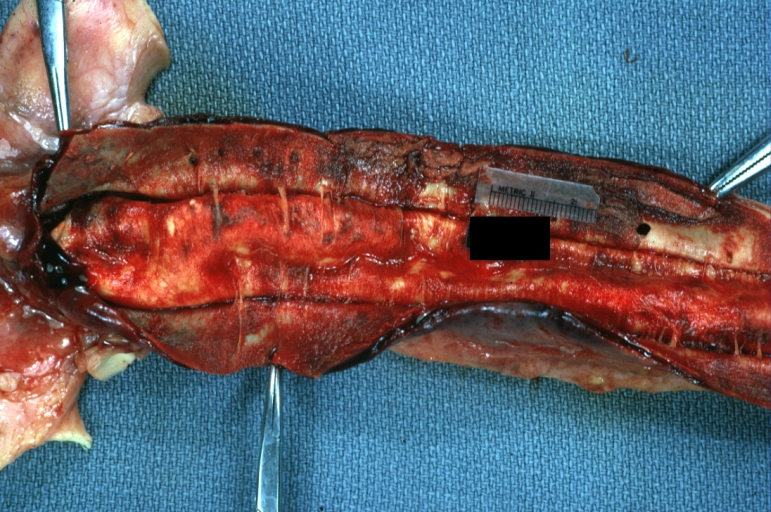
Dissecting Aneurysm: Gross, fixed tissue, descending thoracic segment dissection opened to show the false channel. The true surface is also visible
-
Dissecting Aneurysm: Gross natural color descending aorta opened into false channel
-

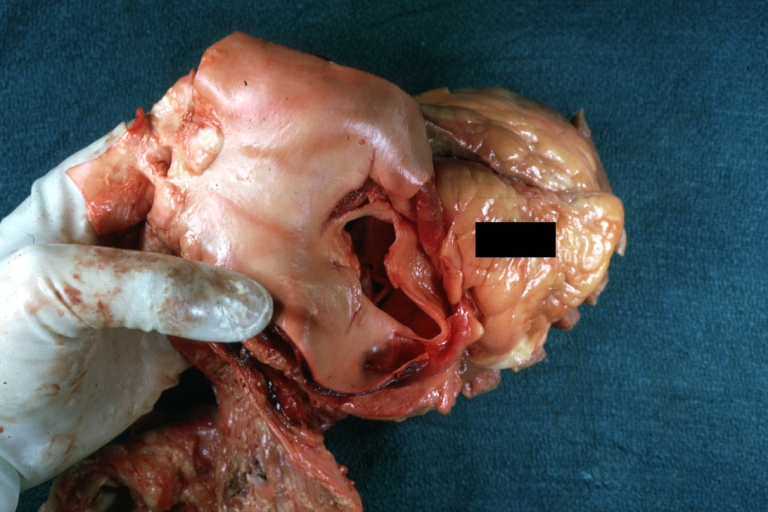
Dissecting Aneurysm: Gross natural color close-up view of aortic valve and proximal aortic arch with ruptured intima rather good illustration of this lesion
-
Dissecting Aneurysm Chronic: Gross natural color first portion of aortic arch with intimal rent well shown with healed margins and view into false channel that shows a surface looking like atherosclerosis which is known to develop in a chronic dissection
-





