Endocarditis pathophysiology: Difference between revisions
No edit summary |
|||
| Line 31: | Line 31: | ||
===Intravenous Drug Use=== | ===Intravenous Drug Use=== | ||
Infections of the [[tricuspid valve]] and less frequently the [[pulmonic valve]] tend to occur in intravenous drug users given the high pathogen burden from their introduction in the [[vein]]. The diseased valve is most commonly affected when there is a pre-existing disease. In rheumatic heart disease this is the [[aortic valve]] and the [[mitral valve]]s, on the left side of the heart. | Infections of the [[tricuspid valve]] and less frequently the [[pulmonic valve]] tend to occur in intravenous drug users given the high pathogen burden from their introduction in the [[vein]]. The diseased valve is most commonly affected when there is a pre-existing disease. In rheumatic heart disease this is the [[aortic valve]] and the [[mitral valve]]s, on the left side of the heart. | ||
==Pathology== | ==Pathology== | ||
Revision as of 16:29, 13 August 2015
|
Endocarditis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease |
|
Case Studies |
|
Endocarditis pathophysiology On the Web |
|
Risk calculators and risk factors for Endocarditis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The turbulent blood flow around the heart valves is a risk factor for the development of endocarditis. The valves may be damaged congenitally, from surgery, by auto-immune mechanisms, or simply as a consequence of old age. The damaged endothelium of these areas becomes a site for attachment of infectious agents in infectious endocarditis. Dental procedures, colorectal cancer, urinary tract infections and intravenous drug use are the most common routes of introducing the infectious agent into the bloodstream. The three most common pathogens are strepotococcus viridans, staphylococcus and enterococcus. In non-bacterial thrombotic endocarditis (NBTE), the damaged part of a heart valve becomes covered with a blood clot which organizes.
Bacteremia
In a healthy individual, a bacteremia (where bacteria get into the blood stream through a minor cut or wound) would normally be cleared quickly with no adverse consequences. If a heart valve is damaged and covered with thrombus, these structures can provide a nidus for bacteria to attach themselves and an infection can be established.
Pathogens
The predominant pathogens that account for 70% of cases of infective endocarditis include the following three gram-positive cocci:
- Viridans group streptococci, although the incidence is decreasing
- Staphylococcus species incidence is increasing
- Enterococcus species
Among the streptococcal viridans group the following are the most common:
- Species: sanguis, oralis (mitis), salivarius, mutans
- Anginosus (milleri) group: intermedius, anginosus, constellatus
- Gemella species: morbillorum, bergeriae,sanguinis, hemolysans, Abiotrophia defectiva
- Granulicatella species: elegans, adiacens, paraadiacens, balaenopterae
The surface structure of these species allows them to stick to damaged endothelium.
Causes of Bacteremia
Dental Procedures
The bacteremia is often caused by dental procedures, such as a cleaning or extraction of a tooth. It is important that a dentist or a dental hygienist therefore be told of any heart problems before beginning the procedure. Prophylactic antibiotics are administered to patients with certain heart conditions as a precaution.
Entrance of Bacteria Into the Bloodstream
Another cause of infective endocarditis is a scenario in which an excess number of bacteria enter the bloodstream. Colorectal cancer, serious urinary tract infections, and IV drug use can all introduce large numbers of such bacteria. When a large burden of bacteria are introduced, a normal heart valve may be infected. A more virulent organism (such as Staphylococcus aureus, but see below for others) is often responsible for infecting a normal valve.
Intravenous Drug Use
Infections of the tricuspid valve and less frequently the pulmonic valve tend to occur in intravenous drug users given the high pathogen burden from their introduction in the vein. The diseased valve is most commonly affected when there is a pre-existing disease. In rheumatic heart disease this is the aortic valve and the mitral valves, on the left side of the heart.
Pathology
-
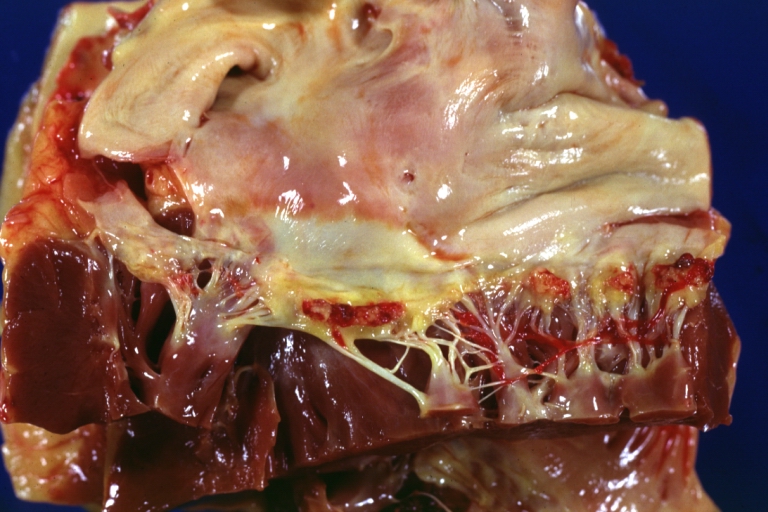
Heart; Breast intraductal papilloma metastasis. Thrombotic Nonbacterial Endocarditis (Infected): Gross mitral valve natural color vegetations well illustrated these were secondarily infected with staphylococcus case of 8 year survival breast intraductal papillary adenocarcinoma with extensive metastases. Aortic valve also involved
-
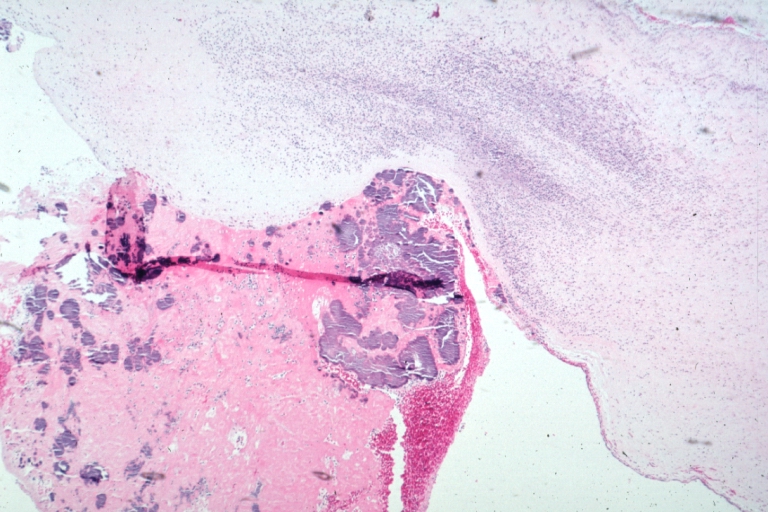
Thrombotic Nonbacterial Endocarditis Infected: Micro low mag H&E fibrin vegetation with masses of staphylococci and inflammatory cells in valve secondarily infected case 8 year survival breast papillary intraductal adenocarcinoma with extensive metastases gross is aortic valve lesions.


-
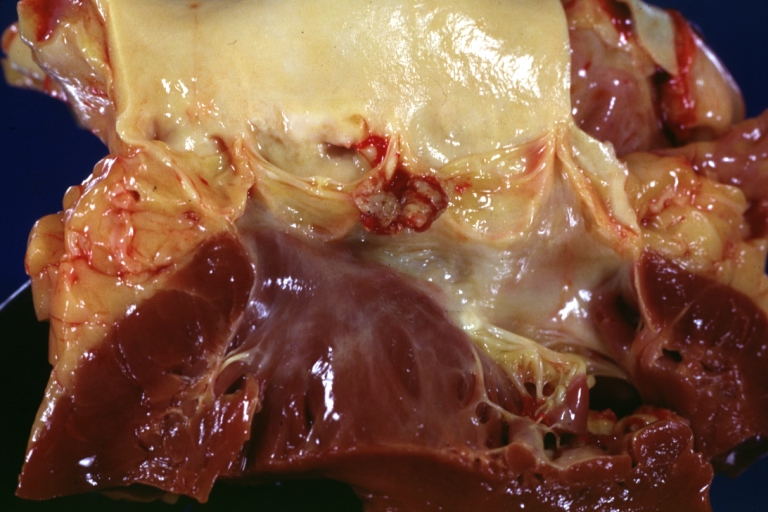
Thrombotic Nonbacterial Endocarditis Infected: Gross close-up natural color vegetations or aortic cusps well shown secondarily infected with staphylococci micro is mitral valve also involved see and case of 8 year survival breast intraductal papillary adenocarcinoma with extensive metastases
-
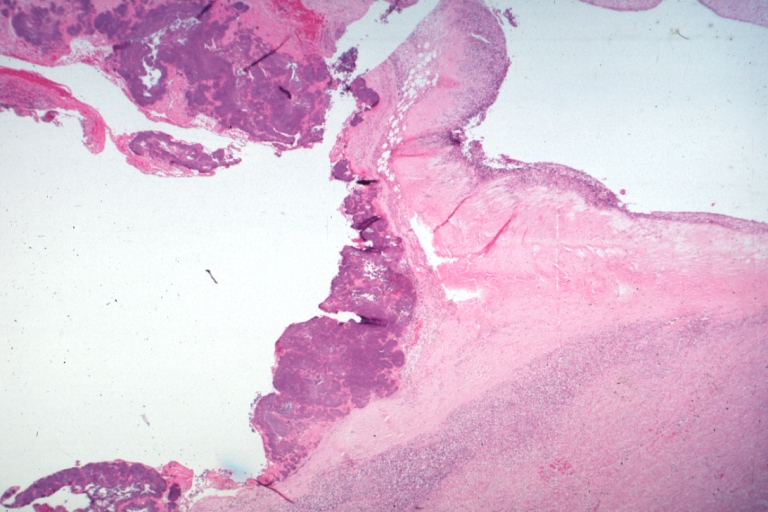
Thrombotic Nonbacterial Endocarditis Infected: Micro low mag H&E large masses staphylococci in vegetation valvulitis is seen gross is mitral valve also involved and case of 8 year survival breast intraductal papillary adenocarcinoma with extensive metastases

