Bile duct cyst classification
|
Bile duct cyst Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Bile duct cyst classification On the Web |
|
American Roentgen Ray Society Images of Bile duct cyst classification |
|
Risk calculators and risk factors for Bile duct cyst classification |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Classification
According to the Todani system, there are five types of bile duct cysts.[1]. This classification was based on site of the cyst or dilatation. Type I to IV has been subtyped.

Type 1: Choledochal Cyst
Choledochal cysts are cystic dilatation of the common bile duct (CBD). Most common variety involving saccular or fusiform dilatation of a portion or entire common bile duct (CBD) with normal intrahepatic duct.
- Account for 80% to 90% of all bile duct cysts
- Often presents during infancy with significant liver disease.
- Characterized by fusiform dilation of the extrahepatic bile duct
- Theorized that choledochal cysts form as the result of reflux of pancreatic secretions into the bile duct via anomalous pancreaticobiliary junction.
- Cyst should be resected completely to prevent associated complications (i.e. ascending cholangitis and malignant transformation).
Type 2: Diverticulum
Isolated diverticulum protruding from the CBD.
- Accounts for 3% of all bile duct cysts
- Represents a true diverticulum.
- Saccular outpouchings arising from the supraduodenal extrahepatic bile duct or the intrahepatic bile ducts.
Type 3: Choledochocele[2]
Arise from dilatation of duodenal portion of CBD or where pancreatic duct meets.
- Accounts for 5% of all bile duct cysts
- Represents protrusion of a focally dilated, intramural segment of the distal common bile duct into the duodenum.
- Choledochoceles may be successfully managed with endoscopic sphincterotomy, surgical excision, or both, in symptomatic patients.
- Often present with pain and obstructive jaundice; many have pancreatitis.
Type 4: Multiple Communicating Intra and Extrahepatic Duct Cysts
Dilatation of both intrahepatic and extrahepatic biliary duct.
- Second most common type of bile duct cysts (10%)
- Subdivided into subtypes A and B.
- Type 4A: Fusiform dilation of the entire extrahepatic bile duct with extension of dilation of the intrahepatic bile ducts
- Type 4B: Multiple cystic dilations involving only the extrahepatic bile duct.
-
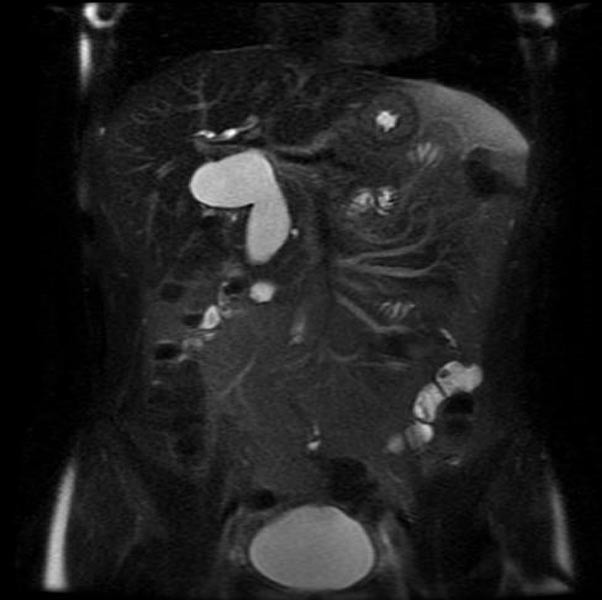
MRI - T2: Type 4 bile duct cyst
-
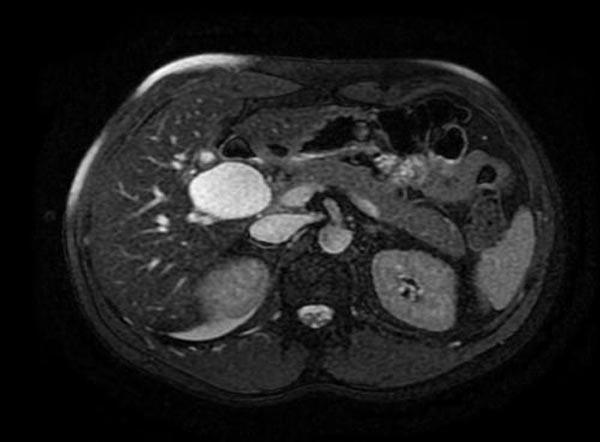
MRI - T2: Type 4 bile duct cyst
-

MRI - T2: Type 4 bile duct cyst
-
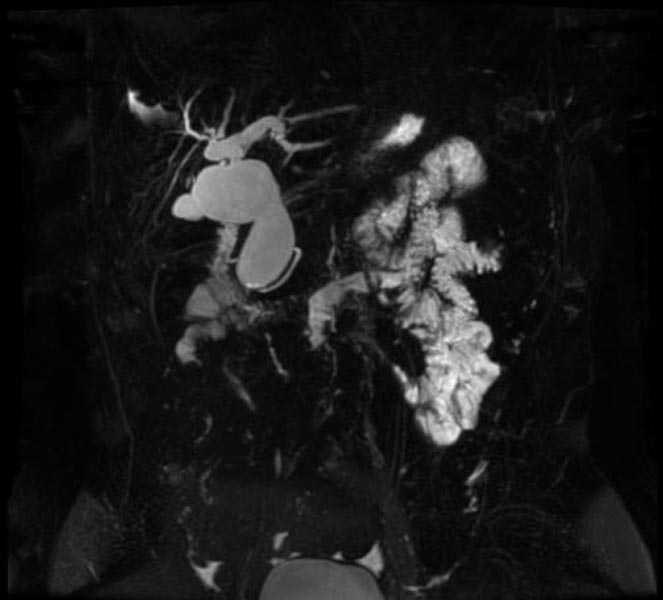
MRCP: Type 4 bile duct cyst




Type 5: Caroli's Disease
Cystic dilatation of intra hepatic biliary ducts. [2] [3] [4] [5] [6] [7] [8]
- Caroli's disease is a rare form of congenital biliary cystic disease manifested by cystic dilations of intrahepatic bile ducts
- Association with benign renal tubular ectasia and other forms of renal cystic disease.
References
- ↑ Todani T, Watanabe Y, Narusue M, Tabuchi K, Okajima K (1977). "Congenital bile duct cysts: Classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst". Am. J. Surg. 134 (2): 263–9. PMID 889044.
- ↑ Caroli, J, et al. La dilatation polykystique congenitale des voies biliaires intrahepatiques. Essai del classification. Sem Hop Paris 1958;34:488
- ↑ Lu, S.C. et al. Diseases of the biliary tree. Textbook of Gastroenterology 1995:2212.
- ↑ Tandon, RK, et al. Caroli’s disease: A heterogeneous entity. Amer J Gastroent 1990;85:170. PMID 2301339
- ↑ Chalasani, N, et al. Spontaneous rupture of a bile duct. Amer J Gastroent 1997;92:1062. PMID 9177539
- ↑ Miller, WJ, et al. Imaging findings in Caroli’s disease. Am J Roenth 1995;165:333. PMID 7618550
- ↑ Torra, R, et al. Autosomal dominant polycystic kidney disease and Caroli’s disease. Kidney Int 1997;52:33. PMID 9211343
- ↑ Ros, E, et al. Ursodeoxycholic acid treatment of primary hepatolithiasis in Caroli’s syndrome. Lancet 1993;342:404. PMID 8101905