Torsades de pointes electrocardiogram: Difference between revisions
| Line 4: | Line 4: | ||
==Overview== | ==Overview== | ||
The [[EKG]] is the main diagnostic tool for torsades de pointes. | |||
==Electrocardiography== | ==Electrocardiography== | ||
Revision as of 17:22, 15 October 2012
|
Torsades de pointes Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Torsades de pointes electrocardiogram On the Web |
|
American Roentgen Ray Society Images of Torsades de pointes electrocardiogram |
|
Risk calculators and risk factors for Torsades de pointes electrocardiogram |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The EKG is the main diagnostic tool for torsades de pointes.
Electrocardiography
EKG is the main diagnostic tool in patients with Torsade de pointes. EKG findings that can be seen are:
- Progressive change in polarity of QRS about the isoelectric line occurs
- Prolonged QT interval (QT ≥ 0.60 s or QTc ≥ 0.45 s)
- Pathological U
- Rotation of the heart's electrical axis by at least 180º
- Preceded by short long and short RR-intervals
- Triggered by an early premature ventricular contraction(R-on-T PVC)
- Paroxysms of 5-20 beats at a rate ≥ 200 bpm
- Patients may revert spontaneously to a nonpolymorphic ventricular tachycardia or ventricular fibrillation
Background
- The peaks of the QRS complexes appear to twist around the isoelectric axis.
- Polymorphic VT is distinguished from Torsades by the absence of QT prolongation in polymorphic VT.
EKG Findings
- Paroxysms of VT with irregular RR intervals.
- A ventricular rate between 200 and 250 beats per minute.
- Two or more cycles of QRS complexes with alternating polarity.
- Changing amplitude of the QRS complexes in each cycle in a sinusoidal fashion.
- Prolongation of the QT interval.
- Is often initiated by a PVC with a long coupling interval, R on T phenomenon.
- There are usually 5 to 20 complexes in each cycle.
Examples
EKG's shown below are courtesy of C. Michael Gibson MS MD, and copylefted
-
12 lead EKG at admission
-
-
-
-
-
-
-
-
-
-
-


Examples from different resources
-
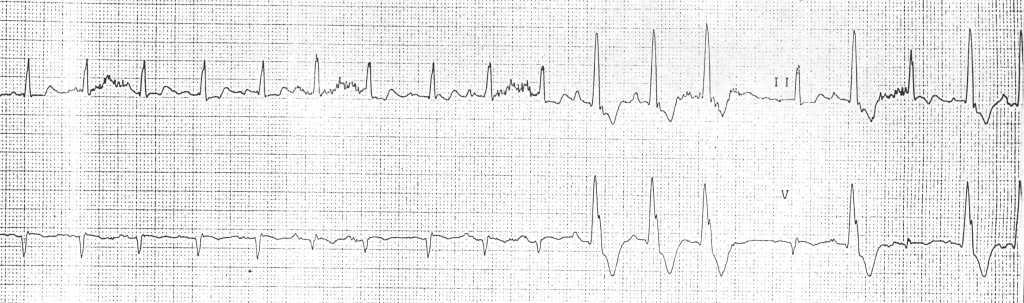
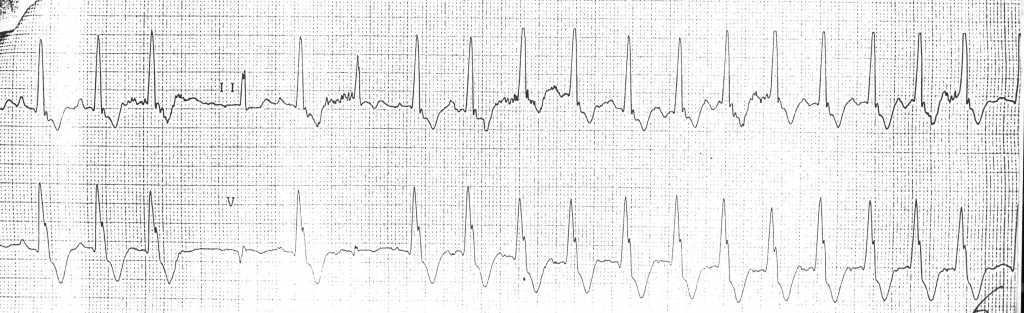
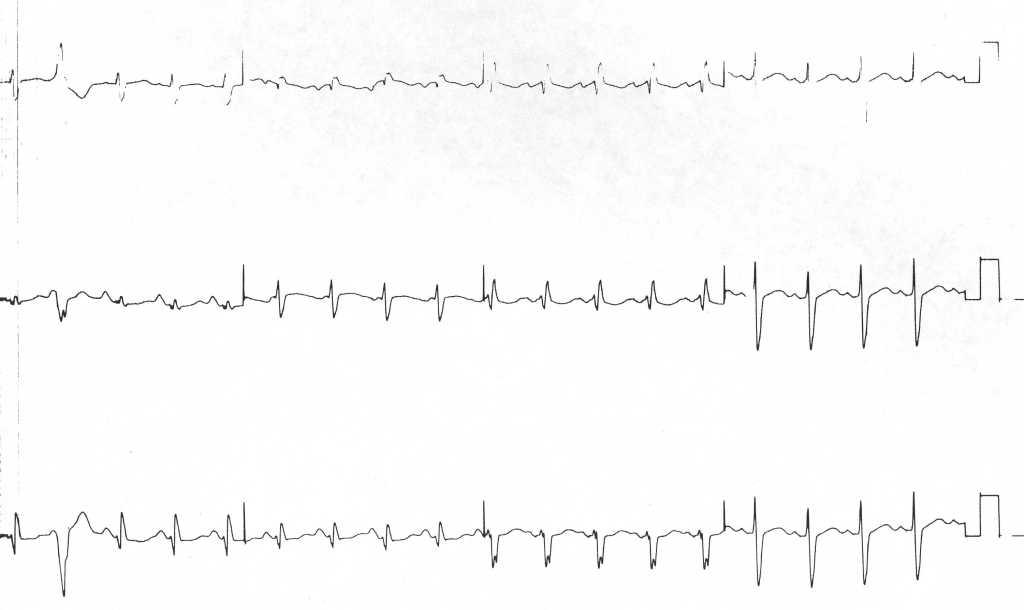
![Arrhythmias in a patient with short coupled torsade de pointes[1]](/images/f/f1/Shortcoupled_tdp1.jpg)
Arrhythmias in a patient with short coupled torsade de pointes[1]
-
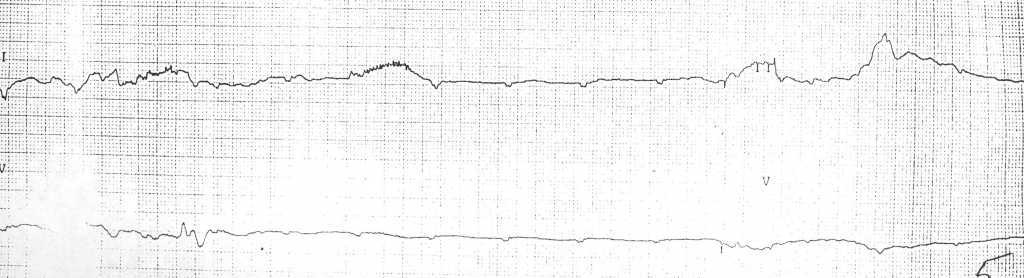
![Arrhythmias in a patient with short coupled torsades de pointes degenerating in ventricular fibrillation[1]](/images/2/2c/Shortcoupled_tdp2.jpg)
Arrhythmias in a patient with short coupled torsades de pointes degenerating in ventricular fibrillation[1]
![Arrhythmias in a patient with short coupled torsade de pointes[1]](/index.php/File:Shortcoupled_tdp1.jpg)
![Arrhythmias in a patient with short coupled torsades de pointes degenerating in ventricular fibrillation[1]](/index.php/File:Shortcoupled_tdp2.jpg)
![Arrhythmias in a patient with short coupled torsade de pointes: frequent short coupled extrasystoles[1]](/index.php/File:Shortcoupled_tdp3.jpg)
![Arrhythmias in a patient with short coupled torsade de pointes: frequent short coupled extrasystoles [1]](/index.php/File:Shortcoupled_tdp4.jpg)
-
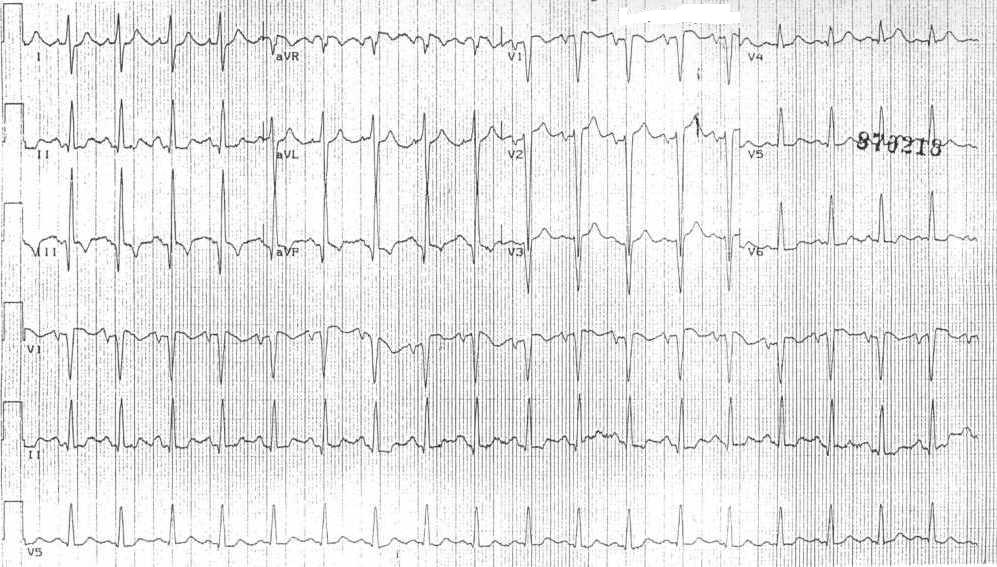
![A 12 lead ECG recording example of TdP[2]](/images/f/fc/12leadTorsade.jpg)
A 12 lead ECG recording example of TdP[2]
![A 12 lead ECG recording example of TdP[2]](/index.php/File:12leadTorsade.jpg)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

References
- ↑ 1.0 1.1 1.2 1.3 Leenhardt A, Glaser E, Burguera M, Nuernberg M, Maison-Blanche P, and Coumel P. Short-coupled variant of torsade de pointes. A new electrocardiographic entity in the spectrum of idiopathic ventricular tachyarrhythmias. Circulation 1994 Jan; 89(1) 206-15. PMID 8281648
- ↑ Khan IA. Twelve-lead electrocardiogram of torsade de pointes Tex Heart Inst J. 2001; 28 (1): 69. PMID 11330748