Ovarian torsion
|
Ovarian torsion Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Ovarian torsion On the Web |
|
American Roentgen Ray Society Images of Ovarian torsion |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: Adnexal torsion
Overview
Ovarian torsion refers to a twisting of the ovary. If the torsion involves the ovary and the oviduct it is called adnexal torsion. Ovarian torsion is in the differential diagnosis of unilateral abdominal pain in a woman. Approximately 60% of the time it occurs on the right side of the abdomen.
Epidemiology and Demographics
Obviously ovarian torsion only occurs in women. Ovarian torsion is the fifth most common gynecologic emergency. 83% of cases occur in women of reproductive age, with a median age at presentation of 28 years.
Pathophysiology
In general, ovarian torsion occurs in association with an enlarged ovary. Because ovarian enlargement plays a critical role, 50% to 60% of cases of ovarian torsion are due to either benign or malignant ovarian tumors, usually over 4 cm in size. An enlarged ovary that occurs in early pregnancy due to enlargement of the corpus lutiem can also predispose a woman to ovarian torsion. Likewise women undergoing fertility treatment who develop theca lutein cysts are at risk of ovarian torsion. Ovarian torsion can occur in children if a long fallopian tube is present.
Differential Diagnosis of Underlying Causes of Ovarian Torsion
Gynecologic Disorders
Infertility drugs
Long fallopian tube in children
Benign and malignant ovarian tumors
Differential Diagnosis of Disorders That Ovarian Torsion Should Be Distinguished from
Diagnosis
Abdominal ultrasound is helpful in establishing the diagnosis in patients with suspected torsion.
-

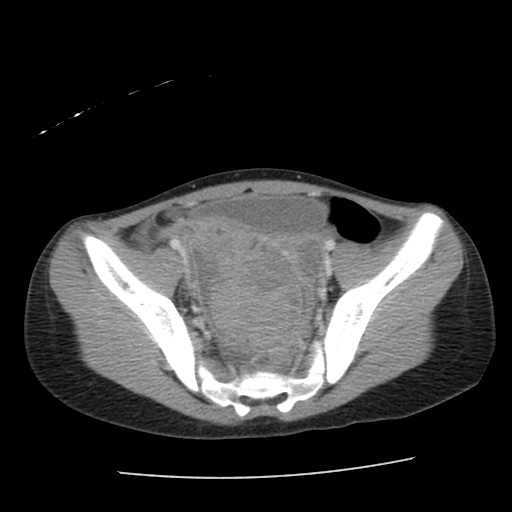
CT patient#1 Image courtesy of RadsWiki and copylefted
-

CT patient#1 Image courtesy of RadsWiki and copylefted
-

CT patient#1 Image courtesy of RadsWiki and copylefted
-

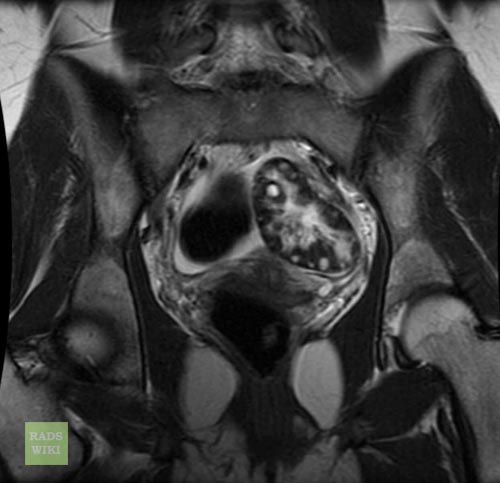
Coronal T2 patient#1 Image courtesy of RadsWiki and copylefted
-
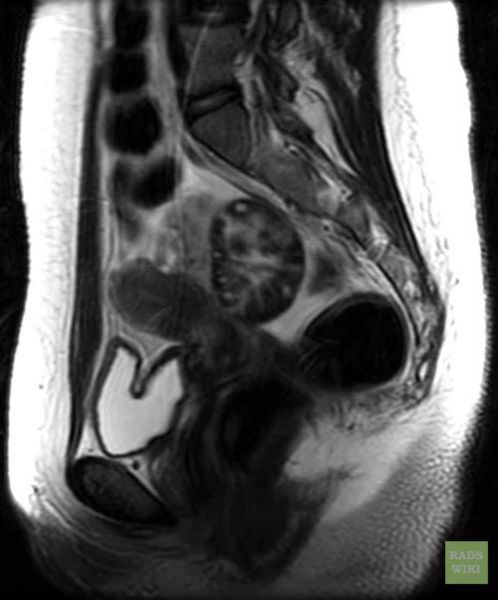
Sag T2 patient#1 Image courtesy of RadsWiki and copylefted
-
Axial T2 patient#1 Image courtesy of RadsWiki and copylefted






-

8 y/o female with right lower quadrant pain patient#2 Image courtesy of RadsWiki and copylefted
-
8 y/o female with right lower quadrant pain patient#2 Image courtesy of RadsWiki and copylefted
-

8 y/o female with right lower quadrant pain patient#2 Image courtesy of RadsWiki and copylefted
-

8 y/o female with right lower quadrant pain patient#2 Image courtesy of RadsWiki and copylefted
-

8 y/o female with right lower quadrant pain patient#2 Image courtesy of RadsWiki and copylefted





Treatment
Associated symptoms of nausea and vomiting can be treated with antiemetics. Dehydration secondary to vomiting can be treated with intravenous fluids.
Early Conservative Management
If there is no evidence of vascular compromise, or peritonitis then laparoscopy can be used to uncoil the torsed ovary.
Salpingo-oophorectomy
If there is evidence of vascular compromise, or peritonitis, the salpingo-oophorectomy may be required. Unfortunately, the visual characteristics of the ovaries such as size, color, and edema may not accurately reflect the extent of injury. Therefore, most studies support a strategy of early conservative management, which is successful in 88% of cases.
Treatment to Reduce the Risk of Recurrent Torsion
Among young women in whom there is a long ligament, laparoscopic triplication of the utero-ovarian ligament has been utilized to reduce the risk of recurrent torsion. Patients with polycystic ovarian disease are also at risk of recurrence.