Mononucleosis
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]; Associate Editor(s)-In-Chief: Lakshmi Gopalakrishnan, M.B.B.S. [3]{{#meta: itemprop="medicalWebPageAudiences" content="patient"}}{{#meta: itemprop="medicalWebPageSpecialities" content="cardiology"}}{{#meta: itemprop="medicalWebPageInfoTypes" content="symptoms,diagnosis,treatment,causes,prognosis,complications"}} [[Natural Progression::{{{naturalProgression}}}| ]] Classification Classic::Classification Atypical::
Overview
|
Mononucleosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Mononucleosis On the Web |
|
American Roentgen Ray Society Images of Mononucleosis |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [4]
Overview
Epstein-Barr virus, frequently referred to as EBV, is a member of the herpesvirus family and one of the most common human viruses.
Pathophysiology
Epstein-Barr virus, frequently referred to as EBV, is a member of the herpesvirus family that targets oro-pharyngeal epithelium and B cells. Transmission of the EBV through the air or blood does not normally occur. The incubation period, or the time from infection to appearance of symptoms, ranges from 4 to 6 weeks. Persons with infectious mononucleosis may be able to spread the infection to others for a period of weeks. However, no special precautions or isolation procedures are recommended, since the virus is also found frequently in the saliva of healthy people. In fact, many healthy people can carry and spread the virus intermittently for life. These people are usually the primary reservoir for person-to-person transmission. For this reason, transmission of the virus is almost impossible to prevent.
Epidemiology and Demographics
Majority of mononucleosis syndromes are caused by Epstein-Barr virus, and most people become infected with EBV sometime during their lives with an estimated 90%-95% of persons greater than 21 years of age demonstrating antibody to EBV.[1][2] In the United States, the disease occurs most often among older children and young adults; however, in certain socioeconomically depressed areas the infection affects young children who remain asymptomatic. Additionally, the dormant feature combined with long (4 to 6 week) incubation period of the disease, makes epidemiological control of the disease impractical.
Risk Factors
Majority of the population become infected with EBV at sometime during their lives with an estimated 90%-95% of adults demonstrating seropositivity by 21 years of age. Therefore, even individuals exposed to infected contacts have shown to be previously infected with EBV and hence are not at risk for the manifestation of mononucleosis. However, once infected, the patient carries the virus for the rest of their life with the virus typically residing dormantly in the B lymphocytes. Independent infections of mononucleosis may be contracted multiple times, regardless of whether the patient is already carrying the virus dormantly. Periodic reactivation of the virus may occur, during which time the patient is again infectious, but usually without any symptoms of illness. Therefore, in susceptible hosts under the appropriate environmental stressors, reactivation of the virus occurs to cause vague subclinical symptoms or remain mostly asymptomatic and diagnosed only by a positive serologic response. However, its imperative to note that during this phase the virus can spread to others.
Causes
Epstein-Barr virus is ubiquitous across the globe and the strongest causative agent for the manifestation of infectious mononucleosis. Commonly, a person is first exposed to the virus during or after adolescence. Though once deemed "The Kissing Disease", recent research has shown that transmission of mononucleosis not only occurs from intimate contact with infected saliva, but also from contact with the airborne virus.
For more information on the virus, click here
Differentiating Mononucleosis from other Diseases
Acute mononucleosis, acute cytomegalovirus infection and toxoplasma gondii infection have similar clinical presentations. In addition, since their management is much the same, it is not always helpful, or possible, to distinguish between infectious mononucleosis and cytomegalovirus infection. However, in pregnant women, it is imperative to differentiate mononucleosis from toxoplasmosis as toxo is associated with significant consequences in the fetus. Acute HIV infection can also mimic signs similar to those of infectious mononucleosis, and tests should be performed in pregnant women for the same reason as toxoplasmosis.[3]
Natural History, Complications and Prognosis
Fatalities from mononucleosis are extremely rare in developed nations. However, chronic sub-clinical infection may persist secondary to the dormant virus within the B cells. Reactivation of the virus may occur in susceptible hosts under the appropriate environmental stressors. Similar such reactivation or chronic sub-clinical viral activity in susceptible hosts may trigger multiple host autoimmune diseases and cancers secondary to virus predilection to B lymphocytes and its ability to alter both lymphocyte proliferation and lymphocyte antibody production.
Diagnosis
History and Symptoms
Symptoms of infectious mononucleosis are fever, sore throat, and swollen lymph glands. Sometimes, a splenomegaly or hepatomegaly may develop. Heart problems or involvement of the central nervous system occurs only rarely, and infectious mononucleosis is almost never fatal. There are no known associations between active EBV infection and problems during pregnancy, such as miscarriages or birth defects. Although the symptoms of infectious mononucleosis usually resolve in 1 or 2 months, EBV remains dormant or latent in a few cells in the throat and blood for the rest of the person's life. Periodically, the virus can reactivate and is commonly found in the saliva of infected persons. This reactivation usually occurs without symptoms of illness.
Physical Examination
The classic initial presentation of mononucleosis include: fever, lymphadenopathy, pharyngitis, rash and/or periorbital oedema. Occasionally, patients infected with EBV may also display splenomegaly, with subsequent life-threatening complication of splenic rupture and/or hepatomegaly.
Laboratory Findings
In most cases of infectious mononucleosis, the clinical diagnosis can be made from the characteristic triad of fever, pharyngitis, and lymphadenopathy lasting for 1 to 4 weeks.
Other Imaging Findings
Direct and indirect evidence of persistent viral infection long after recovery from acute illness has been found in patients with chronic fatigue syndrome. This is possibly due to the activation of microglia during the acute infection phase in such individuals. Lumbar puncture, EEG, CT scan and/or MRI may help to evaluate such patients with presumable CNS involvement.
Other Diagnostic Studies
Bilateral tender lymphadenopathy, particularly, the posterior posterior cervical lymph nodes are characteristic of mononucleosis. Therefore, lymph node biopsy if done may reveal atypical lymphocytosis.
Treatment
Medical Therapy
Infectious mononucleosis is generally self-limiting and only symptomatic and/or supportive treatments are used. However, severe tonsillar enlargement may cause life-threatening airway obstruction and therefore, close monitoring of such high-risk patients is essential. Glucocorticoids may be indicated in such cases of severe airway obstruction. Acyclovir has been tried as they decrease oropharyngeal viral shedding. Recently, valacyclovir has shown to lower or eliminate the presence of the Epstein-Barr virus in subjects afflicted with acute mononucleosis, leading to a significant decrease in the severity of symptoms.
Surgery
Infectious mononucleosis is generally self-limiting and only symptomatic and/or supportive therapy may be required. However, in cases of life-threatening splenic rupture which may occur even without trauma, immediate surgery may be life-saving.
Primary Prevention
Majority of mononucleosis syndromes are caused by Epstein-Barr virus, and most people become infected with EBV sometime during their lives with an estimated 90-95% population aged more than 21 years demonstrate antibody to EBV.[1][2] The transmission of the virus requires intimate contact with the saliva of an infected person and rarely occurs via air or blood. Therefore, the most reasonable way to prevent mono is to avoid close contact with infected saliva.
References
- ↑ 1.0 1.1 Henle G, Henle W, Clifford P, Diehl V, Kafuko GW, Kirya BG, Klein G, Morrow RH, Munube GM, Pike P, Tukei PM, Ziegler JL (1969). "Antibodies to Epstein-Barr virus in Burkitt's lymphoma and control groups". Journal of the National Cancer Institute. 43 (5): 1147–57. PMID 5353242. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ 2.0 2.1 Pereira MS, Blake JM, Macrae AD (1969). "EB virus antibody at different ages". British Medical Journal. 4 (5682): 526–7. PMC 1630375. PMID 4902364. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Ebell MH (2004). "Epstein-Barr virus infectious mononucleosis". American Family Physician. 70 (7): 1279–87. PMID 15508538. Retrieved 2012-02-23. Unknown parameter
|month=ignored (help)
Pathophysiology
|
Mononucleosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Mononucleosis On the Web |
|
American Roentgen Ray Society Images of Mononucleosis |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [5]
Overview
Epstein-Barr virus, frequently referred to as EBV, is a member of the herpesvirus family that targets oro-pharyngeal epithelium and B cells. Transmission of the EBV through the air or blood does not normally occur. The incubation period, or the time from infection to appearance of symptoms, ranges from 4 to 6 weeks. Persons with infectious mononucleosis may be able to spread the infection to others for a period of weeks. However, no special precautions or isolation procedures are recommended, since the virus is also found frequently in the saliva of healthy people. In fact, many healthy people can carry and spread the virus intermittently for life. These people are usually the primary reservoir for person-to-person transmission. For this reason, transmission of the virus is almost impossible to prevent.
Pathophysiology
- Following intimate contact with infected saliva, the virus infects B cells located in the oropharyngeal epithelium and subsequently spreads to involve the lymph nodes, liver and spleen.
- Mononucleosis was so-named because the count of mononuclear leucocytes (white blood cells with a one-lobed nucleus) rises significantly.
- There are two main types of mononuclear leucocytes: monocytes and lymphocytes.
- Mononuclear leucocytes normally account for about 35% of all white blood cells and in patients infected with mononucleosis, this count can rise to 50-70%.
- In addition, the total white blood count may increase to 10,000-20,000 per cubic millimeter.
- Humoral response: As with many viral infections, such as chicken pox, antibodies to the viral antigens are developed with resultant recovery from acute illness.
- In addition, these antibodies remain in the system for most individuals, creating a lifelong immunity to further infections.
- Also, assessment of these specific antibodies forms the basis to diagnose mononucleosis in patients with atypical presentation or in heterophile negative cases.
- Cellular response:
- Is required to control the proliferation of infected B cells.
- This in turn, helps to terminate active EBV infection and also suppress future infections with EBV.
- Ineffective cellular response results in excessive proliferation of B cells with resultant EBV-associated malignancies such as Burkitt's lymphoma and nasopharyngeal carcinoma.
Transmission
- Transmission of EBV requires intimate contact with the saliva of an infected person.
- Typically, the disease is transmitted from asymptomatic individuals through blood or saliva (hence the kissing disease), or by sharing a drink, or sharing eating utensils. The disease is far less contagious than is commonly thought. In rare cases, a person may have a high resistance to infection.
- Modes of transmission include:
- Saliva
- Epstein-Barr virus (EBV) shed for up to 18 months after primary infection
- Intermittent viral shedding thereafter in asymptomatic sero-positive patients
- Increased viral shedding in immunocompromised patients
- Blood transfusion is rare.
- Individuals in close living arrangements nearly always pass the infection onto each other, although symptoms may not present for months or even years.
Electron Microscopy

Microscopic Pathology
Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-
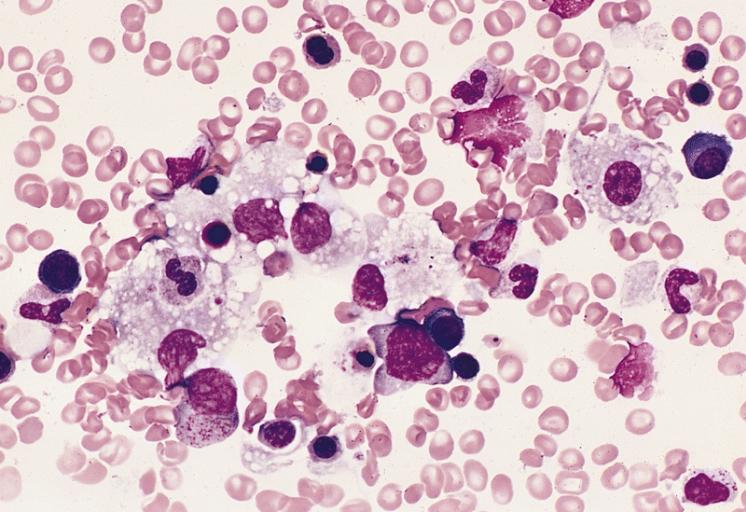
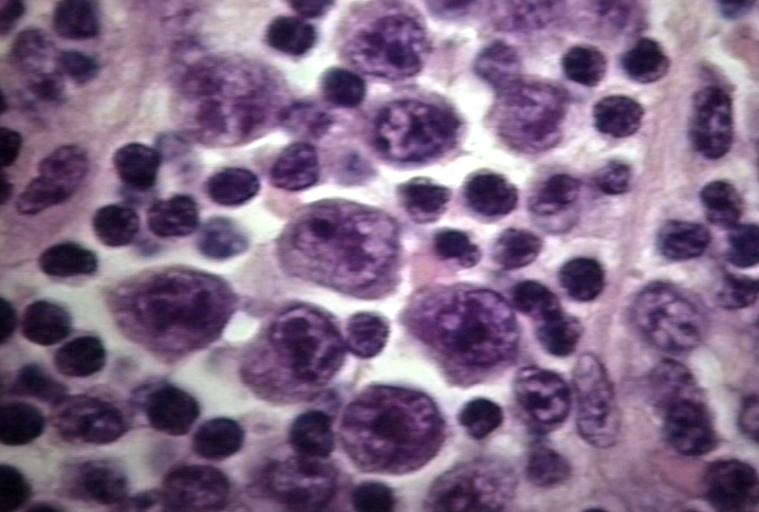
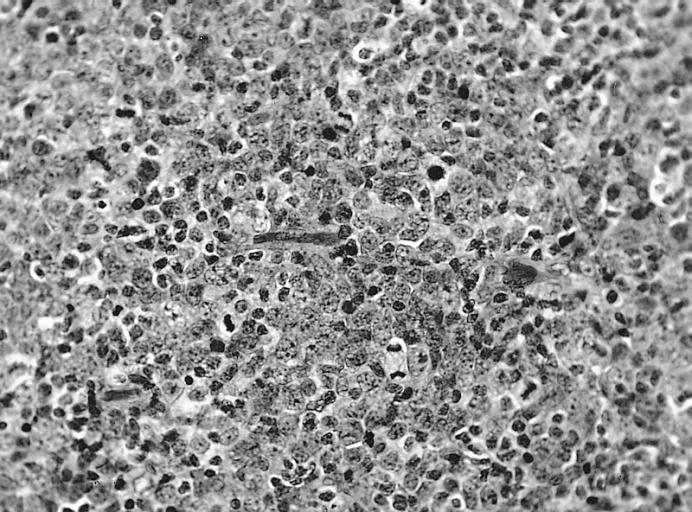
BONE MARROW: INFECTION-ASSOCIATED HEMOPHAGOCYTIC SYNDROME A bone marrow aspirate smear from a child with infection-associated hemophagocytic syndrome secondary to an Epstein-Barr virus infection. On this field there are several large histiocytes. Phagocytosis of nucleated red blood cells, neutrophils, and platelets is evident. The histiocytes have the appearance of reactive cells and should be readily distinguishable from neoplastic histiocytes. (Wright-Giemsa stain)
-
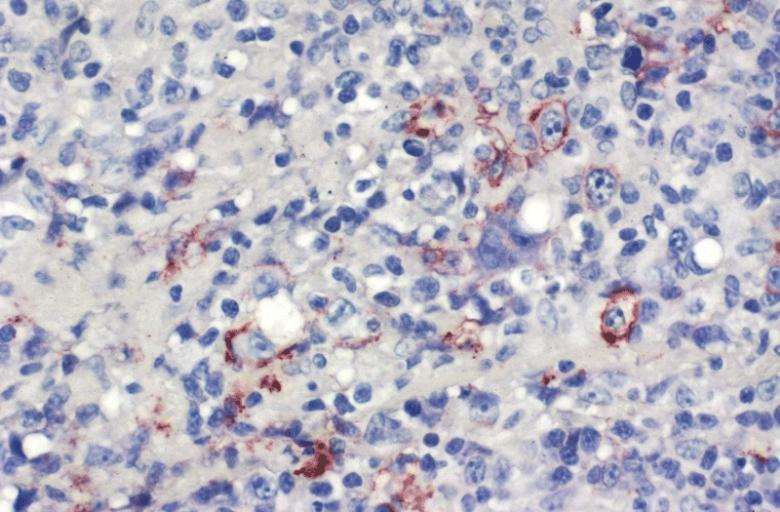
LOWER RESPIRATORY TRACT: (Supplement) AIL/LYG CD20 staining (for B cells) in the viable tissue shows positive staining of scattered large lymphoid cells (C) which were also the cells that were positive for Epstein-Barr virus by in situ hybridization
-
LOWER RESPIRATORY TRACT: (Supplement) AIL/LYG CD20 staining (for B cells) in the viable tissue shows positive staining of scattered large lymphoid cells (C) which were also the cells that were positive for Epstein-Barr virus by in situ hybridization



-
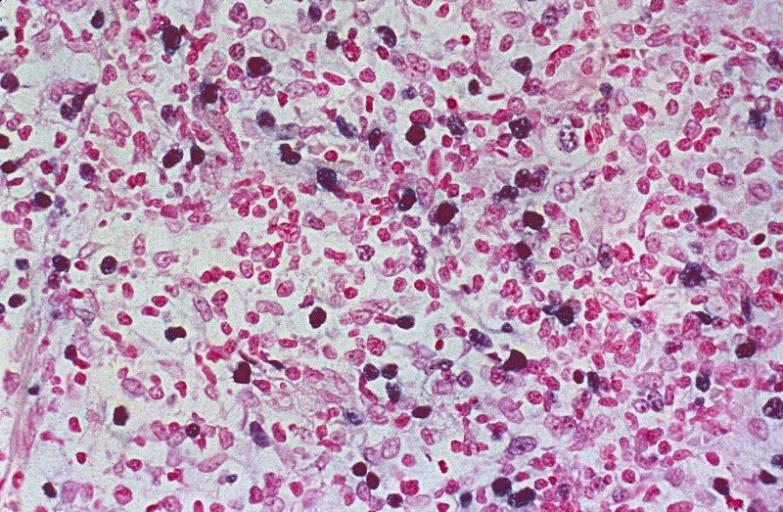
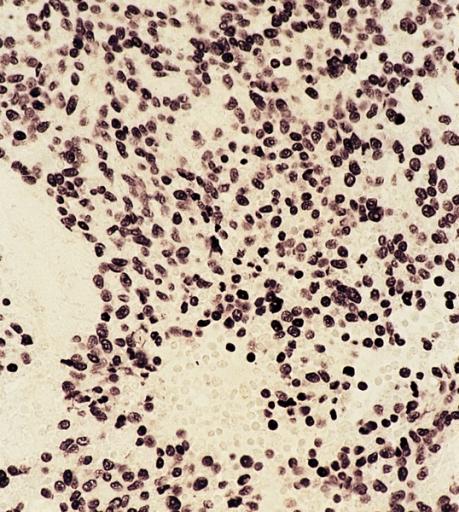
LYMPH NODES-SPLEEN: EPSTEIN-BARR VIRUS-ASSOCIATED INFECTIOUS MONONUCLEOSIS A heterogeneous population is present, including cells mimicking Hodgkin cells. However, the spectrum of cell types and the extensive apoptosis present would not be found in Hodgkin's disease.
-
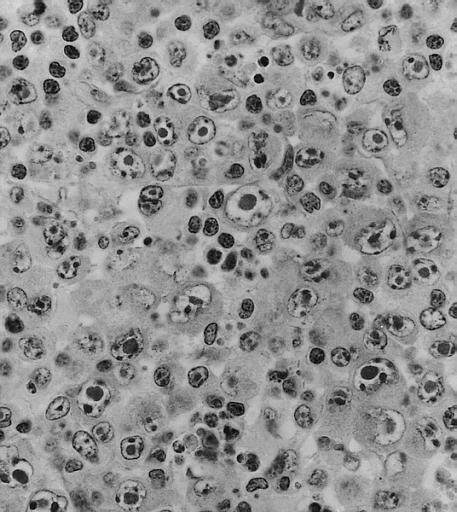
LYMPH NODES-SPLEEN: METASTATIC NASOPHARYNGEAL CARCINOMA IN LYMPH NODE PRESENTING AS METASTATIC CARCINOMA OF UNKNOWN PRIMARY Nuclear labeling of the carcinoma cells for Epstein-Barr virus-encoded RNA strongly suggests that the primary is nasopharyngeal.
-
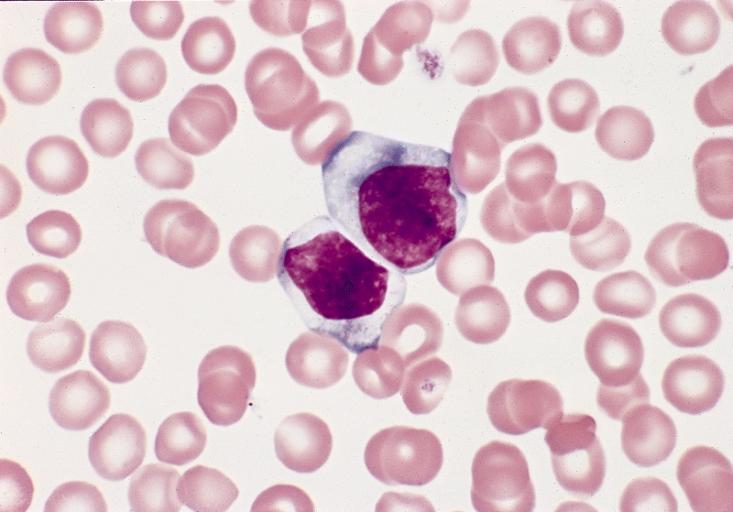
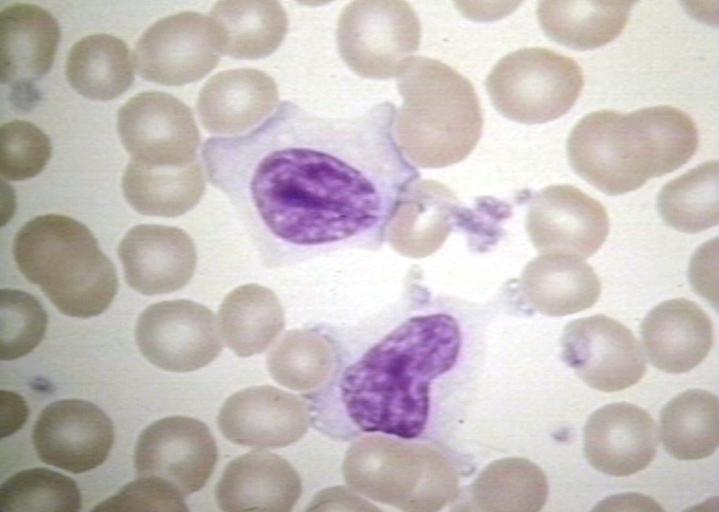
BONE MARROW: REACTIVE (ATYPICAL) LYMPHOCYTES This blood smear is from a 19-year-old male college student with infectious mononucleosis. The two reactive (atypical) lymphocytes are large, with abundant cytoplasm and coarse nuclear chromatin, and lack a nucleolus. Cytoplasmic basophilia is radial in distribution and accentuated at the cell margin. In contrast, lymphoblasts are generally smaller, have less cytoplasm with uniform basophilia and more dispersed nuclear chromatin, and may contain a nucleolus. (Wright-Giemsa stain)



-
LYMPH NODE: INFECTIOUS MONONUCLEOSIS, LYMPH NODE
-
BLOOD: INFECTIOUS MONONUCLEOSIS; PERIPHERAL BLOOD
-

EYE AND OCULAR ADNEXA: BURKITT LYMPHOMA Bilateral involvement.
-
EYE AND OCULAR ADNEXA: BURKITT LYMPHOMA Lymphoblastic tumor with numerous mitotic figures.




References
Epidemiology and Demographics
|
Mononucleosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Mononucleosis On the Web |
|
American Roentgen Ray Society Images of Mononucleosis |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [6]
Overview
Majority of mononucleosis syndromes are caused by Epstein-Barr virus, and most people become infected with EBV sometime during their lives with an estimated 90%-95% of persons greater than 21 years of age demonstrating antibody to EBV.[1][2] In the United States, the disease occurs most often among older children and young adults; however, in certain socioeconomically depressed areas the infection affects young children who remain asymptomatic. Additionally, the dormant feature combined with long (4 to 6 week) incubation period of the disease, makes epidemiological control of the disease impractical.
Epidemiology and Demographics
Age
- In the United States, as many as 95% of adults between 35 and 40 years of age have been infected with approximately 50% of the population seroconverts during early childhood.
- Infants become susceptible to EBV as soon as maternal antibody protection which is present at birth starts to disappears.
- Children if infected with EBV usually remain asymptomatic and hence are indistinguishable from the other mild, brief illnesses of childhood. However, when the infection occurs during adolescence or young adulthood, it causes acute infectious mononucleosis 35% to 50% of the time.
Outbreaks
- True outbreaks of infectious mononucleosis are extremely rare.
- A substantial number of pseudo-outbreaks have been reported and linked to laboratory error.[3][4][5]
References
- ↑ Henle G, Henle W, Clifford P, Diehl V, Kafuko GW, Kirya BG, Klein G, Morrow RH, Munube GM, Pike P, Tukei PM, Ziegler JL (1969). "Antibodies to Epstein-Barr virus in Burkitt's lymphoma and control groups". Journal of the National Cancer Institute. 43 (5): 1147–57. PMID 5353242. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Pereira MS, Blake JM, Macrae AD (1969). "EB virus antibody at different ages". British Medical Journal. 4 (5682): 526–7. PMC 1630375. PMID 4902364. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Armstrong CW, Hackler RL, Miller GB (1986). "Two pseudo-outbreaks of infectious mononucleosis". Pediatric Infectious Disease. 5 (3): 325–7. PMID 3014455.
|access-date=requires|url=(help) - ↑ Herbert JT, Feorino P, Caldwell GG (1977). "False-positive epidemic infectious mononucleosis". American Family Physician. 15 (2): 119–21. PMID 835452. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ "Pseudo-Outbreak of Infectious Mononucleosis -- Puerto Rico, 1990". Retrieved 2012-12-19.
Risk Factors
|
Mononucleosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Mononucleosis On the Web |
|
American Roentgen Ray Society Images of Mononucleosis |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [7]
Overview
A majority of the population is infected with EBV at sometime during their lives with an estimated 90%-95% of adults demonstrating seropositivity by 21 years of age. Therefore, even individuals exposed to infected contacts have shown to be previously infected with EBV and hence are not at risk for the manifestation of mononucleosis. However, once infected, the patient carries the virus for the rest of their life with the virus typically residing dormantly in the B lymphocytes. Independent infections of mononucleosis may be contracted multiple times, regardless of whether the patient is already carrying the virus dormantly. Periodic reactivation of the virus may occur, during which time the patient is again infectious, but usually without any symptoms of illness. Therefore, in susceptible hosts under the appropriate environmental stressors, reactivation of the virus occurs to cause vague subclinical symptoms or remain mostly asymptomatic and diagnosed only by a positive serologic response. However, its imperative to note that during this phase the virus can spread to others.
Risk Factors
By Epidemiology
- It is predominantly found in under-developed countries, and almost everyone is exposed to the ebstein barr virus by 18 months of age. Therefore, even individuals exposed to infected contacts are not at risk for the manifestation of the disease. Additionally, antibody to the virus is almost universally positive.
- In the United States, roughly half of five-year-olds have been infected and up to 95% of adults between 35 and 40 years of age.[1]
By Age
- Infants become susceptible to EBV as soon as maternal antibody protection which is present at birth starts to disappears.
- Children if infected with EBV usually remain asymptomatic and hence are indistinguishable from the other mild, brief illnesses of childhood. However, when the infection occurs during adolescence or young adulthood, it causes acute infectious mononucleosis 35% to 50% of the time.
- Among adults, increased risk of acquiring mononucleosis is observed among:
- Adolescents and young adults
- Patients who have intimate contact with the saliva of an infected person
- Contact with the airborne virus
By Immune System Status
- Any condition that weakens the immune system is a predisposing factor for the development of mononucleosis secondary to EBV infection. Such states include:
- Diabetes
- Following solid organ transplant
- Chemotherapy
- HIV
By Genetic Susceptibility
- A recent twin study done to assess the genetic susceptibility to infectious mononucleosis demonstrated results compatible with a heritable contribution to the risk of acquiring mononucleosis.[2]
References
- ↑ Epstein-Barr Virus and Infectious Mononucleosis - National Center for Infectious Diseases
- ↑ Hwang AE, Hamilton AS, Cockburn MG, Ambinder R, Zadnick J, Brown EE, Mack TM, Cozen W (2011). "Evidence of genetic susceptibility to infectious mononucleosis: a twin study". Epidemiology and Infection: 1–7. doi:10.1017/S0950268811002457. PMID 22152594. Retrieved 2012-02-29. Unknown parameter
|month=ignored (help)
Causes
|
Mononucleosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Mononucleosis On the Web |
|
American Roentgen Ray Society Images of Mononucleosis |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [8]
Overview
Epstein-Barr virus is ubiquitous across the globe and the strongest causative agent for the manifestation of infectious mononucleosis. Commonly, a person is first exposed to the virus during or after adolescence. Though once deemed "The Kissing Disease", recent research has shown that transmission of mononucleosis not only occurs from intimate contact with infected saliva, but also from contact with the airborne virus.
For more information on the virus, click here
Causes
Epstein-Barr Virus
- Epstein-Barr virus is ubiquitous across the globe and the strongest causative agent for the manifestation of infectious mononucleosis. Commonly, a person is first exposed to the virus during or after adolescence.
- Once the acute symptoms of an initial infection disappear, they often do not return. But once infected, the patient carries the virus for the rest of their life. The virus typically lives dormantly in B lymphocytes. Independent infections of mononucleosis may be contracted multiple times, regardless of whether the patient is already carrying the virus dormantly.
- Periodically, the virus can reactivate, during which time the patient is again infectious, but usually without any symptoms of illness. Usually, a patient has few, if any, further symptoms or problems from the latent B lymphocyte infection. However, in susceptible hosts under the appropriate environmental stressors, reactivation of the virus is observed and known to cause vague subclinical symptoms or remain mostly asymptomatic and is diagnosed by positive serologic response. Additionally, its imperative to note that during this phase the virus can spread to others.
- Similar such reactivation or chronic sub-clinical viral activity in susceptible hosts may trigger multiple host autoimmune diseases and cancers secondary to EBV's predilection to B lymphocytes (the primary antibody-producing cell of the immune system) and its ability to alter both lymphocyte proliferation and lymphocyte antibody production.[1][2]
Burkitt's Lymphoma
- Burkitt's lymphoma is a type of Non-Hodgkin's lymphoma and is most common in the equatorial Africa.
- It is co-existent with the presence of malaria. Malarial infection is shown to reduce the immune surveillance of EBV immortalized B cells; thereby, allowing their proliferation which in turn increases the chance of a mutation to occur. Repeated such mutations lead to the escape of B cells from cell-cycle control and furthermore allow the cells to proliferate unchecked, resulting in the formation of Burkitt's lymphoma.
- Commonly affects the jaw bone, forming a huge tumor mass.
- Responds quickly to chemotherapy treatment, namely cyclophosphamide, but recurrence is common.
Nasopharyngeal Carcinoma
- Nasopharyngeal carcinoma is a cancer found in the upper respiratory tract, most commonly in the nasopharynx, and is linked to the EBV virus.
- Occurs secondary to both genetic and environmental factors
- Predominantly prevalent in Southern China and Africa. It is much more common in people of Chinese ancestry (genetic), but is also linked to the Chinese diet of a high amount of smoked fish, which contain nitrosamines, well known carcinogens (environmental).[3]
Chronic Fatigue Syndrome
- In the late 1980s and early 1990s, EBV became the favored explanation for chronic fatigue syndrome. It was noted that people with chronic exhaustion had EBV, although it was also noted EBV was present in almost everyone.
- In a four year study, the Centers for Disease Control and Prevention found that the virus did not adhere to Koch's Postulates and therefore had no definitive association between CFS and EBV but it is still being studied by researchers.
- Majority of the chronic post-infectious fatigue state appear not to be caused by a chronic viral infection, but be triggered by the acute infection.
- Direct and indirect evidence of persistent viral infection has been found in CFS, for example in muscle and via detection of an unusually low molecular weight RNase L enzyme, although the commonality and significance of such findings is disputed.
- Hickie et al, contend that mononucleosis appears to cause a hit and run injury to the brain in the early stages of the acute phase, thereby causing the chronic fatigue state. This would explain why in mononucleosis, fatigue very often lingers for months after the Epstein Barr Virus has been controlled by the immune system.
- However, it has also been noted in several (although altogether rare) cases that the only symptom displayed by a mononucleosis sufferer is elevated moods and higher energy levels, virtually the opposite of CFS and comparable to hypomania.
- Just how infectious mononucleosis changes the brain and causes fatigue (or lack thereof) in certain individuals remains to be seen. Such a mechanism may include activation of microglia in the brain of some individuals during the acute infection, thereby causing a slowly dissipating fatigue.
References
- ↑ Sitki-Green D, Covington M, Raab-Traub N (2003). "Compartmentalization and transmission of multiple epstein-barr virus strains in asymptomatic carriers". Journal of Virology. 77 (3): 1840–7. PMC 140987. PMID 12525618. Retrieved 2012-02-23. Unknown parameter
|month=ignored (help) - ↑ Hadinoto V, Shapiro M, Greenough TC, Sullivan JL, Luzuriaga K, Thorley-Lawson DA (2008). "On the dynamics of acute EBV infection and the pathogenesis of infectious mononucleosis". Blood. 111 (3): 1420–7. doi:10.1182/blood-2007-06-093278. PMC 2214734. PMID 17991806. Retrieved 2012-02-23. Unknown parameter
|month=ignored (help) - ↑ [1] Nasopharyngeal carcinoma information at OncologyChannel.com
Differential Diagnosis
|
Mononucleosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Mononucleosis On the Web |
|
American Roentgen Ray Society Images of Mononucleosis |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [9]; Associate Editor(s)-in-Chief: João André Alves Silva, M.D. [10]
Overview
Acute mononucleosis, acute cytomegalovirus infection and toxoplasma gondii infection have similar clinical presentations. In addition, since their management is much the same, it is not always helpful, or possible, to distinguish between infectious mononucleosis and cytomegalovirus infection. However, in pregnant women, it is imperative to differentiate mononucleosis from toxoplasmosis as toxo is associated with significant consequences in the fetus. Acute HIV infection can also mimic signs similar to those of infectious mononucleosis, and tests should be performed in pregnant women for the same reason as toxoplasmosis.[1]
Differentiating Mononucleosis from Other Diseases
The table below summarizes the findings that differentiate Mononucleosis from other conditions that cause fever, fatigue, abdominal pain and diarrhea:[2]
| Disease | Findings |
|---|---|
| Ebola | Presents with fever, chills vomiting, diarrhea, generalized pain or malaise, and sometimes internal and external bleeding, that follow an incubation period of 2-21 days. |
| Typhoid fever | Presents with fever, headache, rash, gastrointestinal symptoms, with lymphadenopathy, relative bradycardia, cough and leucopenia and sometimes sore throat. Blood and stool culture can confirm the presence of the causative bacteria. |
| Malaria | Presents with acute fever, headache and sometimes diarrhea (children). A blood smears must be examined for malaria parasites. The presence of parasites does not exclude a concurrent viral infection. An antimalarial should be prescribed as an empiric therapy. |
| Lassa fever | Disease onset is usually gradual, with fever, sore throat, cough, pharyngitis, and facial edema in the later stages. Inflammation and exudation of the pharynx and conjunctiva are common. |
| Yellow fever and other Flaviviridae | Present with hemorrhagic complications. Epidemiological investigation may reveal a pattern of disease transmission by an insect vector. Virus isolation and serological investigation serves to distinguish these viruses. Confirmed history of previous yellow fever vaccination will rule out yellow fever. |
| Shigellosis & other bacterial enteric infections | Presents with diarrhea, possibly bloody, accompanied by fever, nausea, and sometimes toxemia, vomiting, cramps, and tenesmus. Stools contain blood and mucous in a typical case. A search for possible sites of bacterial infection, together with cultures and blood smears, should be made. Presence of leucocytosis distinguishes bacterial infections from viral infections. |
| Leukemia | Cancer of the blood or bone marrow and is characterized by an abnormal proliferation (production by multiplication) of blood cells, usually white blood cells (leukocytes). It is part of the broad group of diseases called hematological neoplasms. |
| Tonsillitis | Tonsillitis is characterized by signs of red, swollen tonsils which may have a purulent exudative coating of white patches (i.e. pus). In addition, there may be enlarged and tender neck cervical lymph nodes. |
| Pharyngitis | Typically characterized by sore throat, but commonly accompanied by fever, headache, joint pain and muscle aches, skin rashes, swollen lymph nodes in the neck, diphtheria and common cold. |
| Adenovirus infections | Commonly presents by a cold syndrome, pneumonia, croup and bronchitis. |
| Influenza | Symptoms of influenza can start quite suddenly one to two days after infection. Usually the first symptoms are chills or a chilly sensation but fever is also common early in the infection, with body temperatures as high as 39 °C (approximately 103 °F). Many people are so ill that they are confined to bed for several days, with aches and pains throughout their bodies, which are worst in their backs and legs. Common symptoms of the flu such as fever, headaches, and fatigue come from the huge amounts of proinflammatory cytokines and chemokines (such as interferon or tumor necrosis factor) produced from influenza-infected cells.[3] In contrast to the rhinovirus that causes the common cold, influenza does cause tissue damage, so symptoms are not entirely due to the inflammatory response.[4] |
| Others | Leptospirosis, rheumatic fever, typhus, and mononucleosis can produce signs and symptoms that may be confused with Ebola in the early stages of infection. |
The table below summarizes the findings that differentiate the rash in Mononucleosis from other conditions, such as:[5]
| Disease | Findings |
|---|---|
| [[Insect bite]] | In an insect bite, the insect injects formic acid, which can cause an immediate skin reaction often resulting in a rash and swelling in the injured area, often with formation of vesicles. |
| Kawasaki disease | Commonly presents with high and persistent fever, red mucous membranes in mouth, "strawberry tongue", swollen lymph nodes and skin rash in early disease, with peeling off of the skin of the hands, feet and genital area. |
| Measles | Commonly presents with high fever, coryza and conjunctivitis, with observation of oral mucosal lesions (Koplik's spots), followed by widespread skin rash. |
| Monkeypox | Presentation is similar to smallpox, although it is often a milder form, with fever, headache, myalgia, back pain, swollen lymph nodes, a general feeling of discomfort, and exhaustion. Within 1 to 3 days (sometimes longer) after the appearance of fever, the patient develops a papular rash, often first on the face. The lesions usually develop through several stages before crusting and falling off. |
| Rubella | Commonly presents with a facial rash which then spreads to the trunk and limbs, fading after 3 days, low grade fever, swollen glands, joint pains, headache and conjunctivitis. The rash disappears after a few days with no staining or peeling of the skin. Forchheimer's sign occurs in 20% of cases, and is characterized by small, red papules on the area of the soft palate. |
| Atypical measles | Symptoms commonly begin about 7-14 days after infection and present as fever, cough, coryza and conjunctivitis. Observation of Koplik's spots is also a characteristic finding in measles. |
| Coxsackievirus | The most commonly caused disease is the Coxsackie A disease, presenting as hand, foot and mouth disease. It may be asymptomatic or cause mild symptoms, or it may produce fever and painful blisters in the mouth (herpangina), on the palms and fingers of the hand, or on the soles of the feet. There can also be blisters in the throat or above the tonsils. Adults can also be affected. The rash, which can appear several days after high temperature and painful sore throat, can be itchy and painful, especially on the hands/fingers and bottom of feet. |
| Acne | Typical of teenagers, usually appears on the face and upper neck, but the chest, back and shoulders may have acne as well. The upper arms can also have acne, but lesions found there are often keratosis pilaris, not acne. The typical acne lesions are comedones and inflammatory papules, pustules, and nodules. Some of the large nodules were previously called "cysts" |
| Syphilis | Commonly presents with generalized systemic symptoms such as malaise, fatigue, headache and fever. Skin eruptions may be subtle and asymptomatic. It is classically described as 1) non-pruritic bilateral symmetrical mucocutaneous rash; 2) non-tender regional lymphadenopathy; 3) condylomata lata; and 4) patchy alopecia. |
| Molluscum contagiosum | Lesions are commonly flesh-colored, dome-shaped, and pearly in appearance. They are often 1-5 millimeters in diameter, with a dimpled center. Generally not painful, but they may itch or become irritated. Picking or scratching the lesions may lead to further infection or scarring. In about 10% of the cases, eczema develops around the lesions. They may occasionally be complicated by secondary bacterial infections. |
| Mononucleosis | Common symptoms include low-grade fever without chills, sore throat, white patches on tonsils and back of the throat, muscle weakness and sometime extreme fatigue, tender lymphadenopathy, petechial hemorrhage and skin rash. |
| Toxic erythema | Common rash in infants, with clustered and vesicular appearance. |
| Rat-bite fever | Commonly presents with fever, chills, open sore at the site of the bite and rash, which may show red or purple plaques. |
| Parvovirus B19 | The rash of fifth disease is typically described as "slapped cheeks," with erythema across the cheeks and sparing the nasolabial folds, forehead, and mouth. |
| Cytomegalovirus | Common symptoms include sore throat, swollen lymph nodes, fever, headache, fatigue, weakness, muscle pain and loss of appetite. |
| Scarlet fever | Commonly includes fever, punctate red macules on the hard and soft palate and uvula (Forchheimer's spots), bright red tongue with a "strawberry" appearance, sore throat and headache and lymphadenopathy. |
| Rocky Mountain spotted fever | Symptoms may include maculopapular rash, petechial rash, abdominal pain and joint pain. |
| Stevens-Johnson syndrome | Symptoms may include fever, sore throat and fatigue. Commonly presents ulcers and other lesions in the mucous membranes, almost always in the mouth and lips but also in the genital and anal regions. Those in the mouth are usually extremely painful and reduce the patient's ability to eat or drink. Conjunctivitis of the eyes occurs in about 30% of children. A rash of round lesions about an inch across, may arise on the face, trunk, arms and legs, and soles of the feet, but usually not on the scalp. |
| Varicella-zoster virus | Commonly starts as a painful rash on one side of the face or body. The rash forms blisters that typically scab over in 7-10 days and clears up within 2-4 weeks. |
| Chickenpox | Commonly starts with conjunctival and catarrhal symptoms and then characteristic spots appearing in two or three waves, mainly on the body and head, rather than the hands, becoming itchy raw pox (small open sores which heal mostly without scarring). Touching the fluid from a chickenpox blister can also spread the disease. |
| Meningococcemia | Commonly presents with rash, petechiae, headache, confusion, and stiff neck, high fever, mental status changes, nausea and vomiting. |
| Rickettsialpox | First symptom is commonly a bump formed by a mite-bite, eventually resulting in a black, crusty scab. Many of the symptoms are flu-like including fever, chills, weakness and muscle pain but the most distinctive symptom is the rash that breaks out, spanning the person's entire body. |
| Meningitis | Commonly presents with headache, nuchal rigidity, fever, petechiae and altered mental status. |
| Impetigo | Commonly presents with pimple-like lesions surrounded by erythematous skin. Lesions are pustules, filled with pus, which then break down over 4-6 days and form a thick crust. It's often associated with insect bites, cuts, and other forms of trauma to the skin. |
Pharyngitis vs EBV
- EBV infection may cause either exudative or non-exudative pharyngitis and both of which is colonized by streptococcus pyogens present in the oropharynx
- Petechial hemorrhages present in the posterior oropharynx are characteristic of infectious mononucleosis
- Edema of the uvula is rare but if present differentiates mononucleosis from all other types of pharyngitis
Infectious mononucleosis should be differentiated from other diseases that cause runny nose, cough, and constitutional symptoms.
| Disease | History | Physical examination | Laboratory or radiological findings |
|---|---|---|---|
| Acute viral nasopharyngitis[6] |
|
|
|
| Allergic rhinitis[7] |
|
|
|
| Acute sinusitis[9] |
|
|
|
| Infectious mononucleosis[11] |
|
|
|
Cytomegalovirus vs EBV
- Almost all cases of mononucleosis are caused by the EBV; however, cytomegalovirus can produce a similar symptoms but milder and with less throat pain and no rash.
- Extreme fatigue, bilateral supra-orbital edema, tender bilateral lymphadenopathy, splenomegaly, elevated liver function tests are characteristic of mononucleosis and may or may not be present in cytomegalovirus infections.
- Although, due to the presence of the atypical lymphocytes on the blood smear in both conditions, some physicians confusingly used to include both infections under the diagnosis of "mononucleosis," though EBV is by definition the infection that must be present for this illness.
- An elevated antibody (IgM) titer specific for CMV helps to differentiate it from EBV infection
Toxoplasmosis vs EBV
- In pregnant women, it is imperative to differentiate mononucleosis from toxoplasmosis as toxo is associated with significant consequences in the fetus.
- In contrast to tender bilateral lymphadenopathy observed in patients with mononucleosis, toxo causes unilateral lymphadenopathy.
- In addition, normal to moderately elevated white blood cell count, particularly the number of lymphocytes is observed with mononucleosis; while, in patients infected with toxo, the white blood cell count is typically normal.
Viral Hepatitis vs EBV
- Liver function tests may show a moderate elevation of liver enzyme levels in nearly 90% of patients infected with mononucleosis. On the contrary, there is a significant increase in enzyme levels observed in patients with viral hepatitis.
References
- ↑ Ebell MH (2004). "Epstein-Barr virus infectious mononucleosis". American Family Physician. 70 (7): 1279–87. PMID 15508538. Retrieved 2012-02-23. Unknown parameter
|month=ignored (help) - ↑ "WHO Infection Control for Viral Haemorrhagic Fevers in the African Health Care Setting" (PDF).
- ↑ Schmitz N, Kurrer M, Bachmann MF, Kopf M (2005). "Interleukin-1 is responsible for acute lung immunopathology but increases survival of respiratory influenza virus infection". J Virol. 79 (10): 6441–8. doi:10.1128/JVI.79.10.6441-6448.2005. PMC 1091664. PMID 15858027.
- ↑ Winther B, Gwaltney J, Mygind N, Hendley J. "Viral-induced rhinitis". Am J Rhinol. 12 (1): 17–20. PMID 9513654.
- ↑ Moore, Zack S; Seward, Jane F; Lane, J Michael (2006). "Smallpox". The Lancet. 367 (9508): 425–435. doi:10.1016/S0140-6736(06)68143-9. ISSN 0140-6736.
- ↑ Heikkinen T, Järvinen A (2003). "The common cold". Lancet. 361 (9351): 51–9. doi:10.1016/S0140-6736(03)12162-9. PMID 12517470.
- ↑ Pawankar R, Bunnag C, Chen Y, Fukuda T, Kim YY, Le LT, Huong le TT, O'Hehir RE, Ohta K, Vichyanond P, Wang DY, Zhong N, Khaltaev N, Bousquet J (2009). "Allergic rhinitis and its impact on asthma update (ARIA 2008)--western and Asian-Pacific perspective". Asian Pac. J. Allergy Immunol. 27 (4): 237–43. PMID 20232579.
- ↑ Skoner DP (2001). "Allergic rhinitis: definition, epidemiology, pathophysiology, detection, and diagnosis". J. Allergy Clin. Immunol. 108 (1 Suppl): S2–8. PMID 11449200.
- ↑ Low DE, Desrosiers M, McSherry J, Garber G, Williams JW, Remy H, Fenton RS, Forte V, Balter M, Rotstein C, Craft C, Dubois J, Harding G, Schloss M, Miller M, McIvor RA, Davidson RJ (1997). "A practical guide for the diagnosis and treatment of acute sinusitis". CMAJ. 156 Suppl 6: S1–14. PMID 9347786.
- ↑ "Acute maxillary sinusitis". N. Engl. J. Med. 305 (4): 226–7. 1981. doi:10.1056/NEJM198107233050419. PMID 7242607.
- ↑ Niederman JC, McCollum RW, Henle G, Henle W (1968). "Infectious mononucleosis. Clinical manifestations in relation to EB virus antibodies". JAMA. 203 (3): 205–9. PMID 4864269.
Natural History, Complications & Prognosis
Diagnosis
{{#ask:Used To Diagnose::Mononucleosis |?Sort Order |format=list |headers=hide |link=none |sep= | |template=MedicalTestQuery |sort=Sort Order }}
Treatment
{{#ask:Used To Treat::Mononucleosis |?Sort Order |format=list |headers=hide |link=none |sep= | |template=MedicalTreatmentQuery |sort=Sort Order }} {{#ask:Prevents::Mononucleosis |?Sort Order |intro= | |format=list |headers=hide |link=none |sep= | |template=MedicalTreatmentQuery2 |sort=Sort Order }}