Laryngeal cancer pathophysiology: Difference between revisions
No edit summary |
|||
| Line 3: | Line 3: | ||
{{CMG}} {{AE}}{{Faizan}} | {{CMG}} {{AE}}{{Faizan}} | ||
==Overview== | ==Overview== | ||
Laryngeal cancer arises from [[squamous cell]]s, which are cells that are normally involved in protection of airway. Genes involved in the pathogenesis of laryngeal cancer include ''[[P16 (gene)|p16]]'', ''[[NOTCH1]]'', ''[[cyclin D1]]'', and ''[[TP53]]''. On gross pathology, flattened plaques, mucosal ulceration, and raised margins of the lesion are characteristic findings of laryngeal cancer. On microscopic histopathological analysis, [[spindle cell]]s, basaloid cells, and nuclear atypia are characteristic findings of laryngeal cancer. | |||
==Pathophysiology== | ==Pathophysiology== | ||
| Line 9: | Line 9: | ||
==Genetics== | ==Genetics== | ||
Genes involved in the pathogenesis of | Genes involved in the pathogenesis of laryngeal cancer include: | ||
*''[[P16 (gene)|p16]]'' | *''[[P16 (gene)|p16]]'' | ||
*''[[NOTCH1]]'' | *''[[NOTCH1]]'' | ||
| Line 33: | Line 33: | ||
===Subclassification by site=== | ===Subclassification by site=== | ||
It is generally divided the following way:<ref>URL: [http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Larynx_11protocol.pdf http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Larynx_11protocol.pdf]. Accessed on: | It is generally divided the following way:<ref>URL: [http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Larynx_11protocol.pdf http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Larynx_11protocol.pdf]. Accessed on: October 28, 2015.</ref> | ||
{{familytree/start}} | {{familytree/start}} | ||
| Line 40: | Line 40: | ||
{{familytree | | | | B01 | | | B02 | | | B03|B01=Supraglottis|B02=Glottis|B03=Subglottis }} | {{familytree | | | | B01 | | | B02 | | | B03|B01=Supraglottis|B02=Glottis|B03=Subglottis }} | ||
{{familytree/end}} | {{familytree/end}} | ||
SCC is subdivided by the WHO into:<ref name=Ref_Sternberg4_975>{{Ref Sternberg4|975}}</ref> | SCC is subdivided by the WHO into:<ref name=Ref_Sternberg4_975>{{Ref Sternberg4|975}}</ref> | ||
*Keratinizing type (KT). | *Keratinizing type (KT). | ||
*Undifferentiated type (UT). | *Undifferentiated type (UT). | ||
**EBV association. | **EBV association. | ||
*Nonkeratinizing type (NT). | *Nonkeratinizing type (NT). | ||
**EBV association. | **EBV association. | ||
==Microscopic== | ==Microscopic== | ||
Features based on classification: | Features based on classification: | ||
*Keratinizing subtype: | *Keratinizing subtype: | ||
**Keratinization & intercellular bridges through-out most of the malignant lesion | **Keratinization & intercellular bridges through-out most of the malignant lesion | ||
| Line 69: | Line 62: | ||
**Long rete ridges | **Long rete ridges | ||
**Numerous beeds/blobs of epithelial cells that seem unlikely to be rete ridges | **Numerous beeds/blobs of epithelial cells that seem unlikely to be rete ridges | ||
===Squamous cell carcinoma subtypes=== | |||
There are several subtypes:<ref>Squamous cell carcinoma subtypes. URL: [http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970297-2 http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970297-2]. Accessed on: October 28, 2015.</ref> | |||
*Basaloid | |||
*Warty (Condylomatous) | |||
*Verrucous | |||
*Papillary | |||
*Lymphoepithelial | |||
*Spindle cell | |||
===Images=== | ===Images=== | ||
| Line 77: | Line 79: | ||
</gallery> | </gallery> | ||
====Verrucous squamous cell carcinoma==== | ====Verrucous squamous cell carcinoma==== | ||
| Line 92: | Line 87: | ||
*"Glassy" appearance | *"Glassy" appearance | ||
*Pushing border | *Pushing border | ||
====Spindle cell squamous carcinoma==== | ====Spindle cell squamous carcinoma==== | ||
| Line 101: | Line 94: | ||
*Typically keratin -ve. | *Typically keratin -ve. | ||
*p63 +ve. | *p63 +ve. | ||
====Basaloid squamous cell carcinoma==== | ====Basaloid squamous cell carcinoma==== | ||
*May mimic ''[[adenoid cystic carcinoma]]'' | *May mimic ''[[adenoid cystic carcinoma]]'' | ||
====Lymphoepithelial (squamous cell) carcinoma==== | ====Lymphoepithelial (squamous cell) carcinoma==== | ||
*Lymphoid component | |||
==IHC== | ==IHC== | ||
Immunohistochemistry markers include:<ref name=pmid20233885>{{cite journal |author=Nichols AC, Finkelstein DM, Faquin WC, ''et al.'' |title=Bcl2 and human papilloma virus 16 as predictors of outcome following concurrent chemoradiation for advanced oropharyngeal cancer |journal=Clin. Cancer Res. |volume=16 |issue=7 |pages=2138–46 |year=2010 |month=April |pmid=20233885 |doi=10.1158/1078-0432.CCR-09-3185 |url=}}</ref> | |||
*p63 positive | |||
*EBER negative | |||
*p16 negative | |||
*BCL2 positive/negative | |||
==References== | ==References== | ||
{{reflist|2}} | {{reflist|2}} | ||
| Line 134: | Line 114: | ||
{{WikiDoc Sources}} | {{WikiDoc Sources}} | ||
[[Category:Disease]] | [[Category:Disease]] | ||
[[Category:Types of cancer]] | [[Category:Types of cancer]] | ||
Revision as of 14:52, 28 October 2015
|
Laryngeal cancer Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Laryngeal cancer pathophysiology On the Web |
|
American Roentgen Ray Society Images of Laryngeal cancer pathophysiology |
|
Risk calculators and risk factors for Laryngeal cancer pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Faizan Sheraz, M.D. [2]
Overview
Laryngeal cancer arises from squamous cells, which are cells that are normally involved in protection of airway. Genes involved in the pathogenesis of laryngeal cancer include p16, NOTCH1, cyclin D1, and TP53. On gross pathology, flattened plaques, mucosal ulceration, and raised margins of the lesion are characteristic findings of laryngeal cancer. On microscopic histopathological analysis, spindle cells, basaloid cells, and nuclear atypia are characteristic findings of laryngeal cancer.
Pathophysiology
Laryngeal cancer arises from squamous cells, which are cells that are normally involved in protection of airway. Development of laryngeal cancer is the result of multiple genetic mutations. These mutations lead to activation of oncogenes and inactivation of tumor suppression genes which ultimately results in deregulated cellular proliferation.
Genetics
Genes involved in the pathogenesis of laryngeal cancer include:
Gross Pathology
On gross pathology, laryngeal cancer is characterized by:
- Flattened plaques
- Raised margins of the lesion
- Mucosal ulceration
-
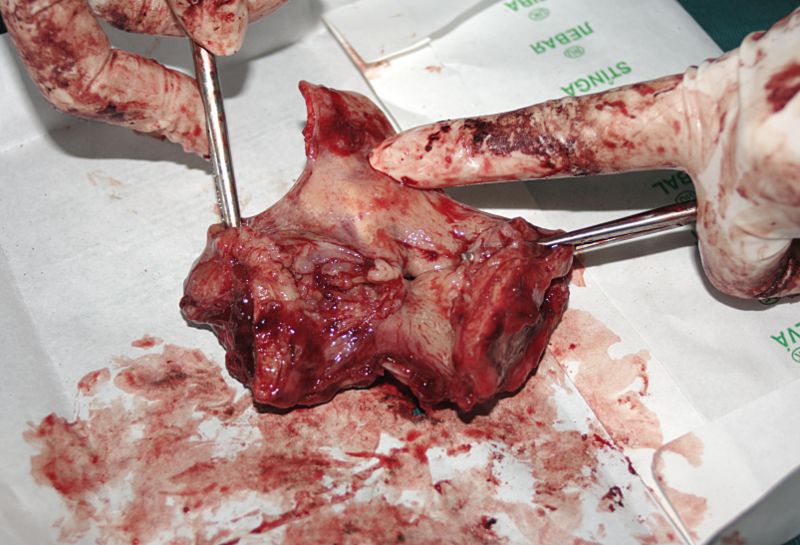
Gross pathology specimen of laryngeal cancer

Microscopic Pathology
On microscopic histopathological analysis, laryngeal carcinoma is characterized by:
- Spindle cells
- Basaloid cells
- Nuclear atypia
- Abundant chromatin
Subclassification by site
It is generally divided the following way:[1]
| Laryngeal cancer | |||||||||||||||||||||||||||||||||
| Supraglottis | Glottis | Subglottis | |||||||||||||||||||||||||||||||
SCC is subdivided by the WHO into:[2]
- Keratinizing type (KT).
- Undifferentiated type (UT).
- EBV association.
- Nonkeratinizing type (NT).
- EBV association.
Microscopic
Features based on classification:
- Keratinizing subtype:
- Keratinization & intercellular bridges through-out most of the malignant lesion
- Undifferentiated type:
- Non-distinct borders/syncytial pattern
- Nucleoli
- Non Keratinizing type:
- Well-defined cell borders
- Eosinophilia
- Extra large nuclei/bizarre nuclei
- Inflammation (lymphocytes, plasma cells)
- Long rete ridges
- Numerous beeds/blobs of epithelial cells that seem unlikely to be rete ridges
Squamous cell carcinoma subtypes
There are several subtypes:[3]
- Basaloid
- Warty (Condylomatous)
- Verrucous
- Papillary
- Lymphoepithelial
- Spindle cell
Images
-
![Laryngeal squamous carcinoma (Intermediate Magnification)[4]](/images/c/ca/800px-Laryngeal_squamous_carcinoma_--_intermed_mag.jpg)
Laryngeal squamous carcinoma (Intermediate Magnification)[4]
-
![Laryngeal squamous carcinoma (High Magnification)[4]](/images/e/e3/800px-Laryngeal_squamous_carcinoma_--_high_mag.jpg)
Laryngeal squamous carcinoma (High Magnification)[4]
-
![Laryngeal squamous carcinoma (Very High Magnification)[4]](/images/f/f5/800px-Laryngeal_squamous_carcinoma_--_very_high_mag.jpg)
Laryngeal squamous carcinoma (Very High Magnification)[4]
![Laryngeal squamous carcinoma (Intermediate Magnification)[4]](/index.php/File:800px-Laryngeal_squamous_carcinoma_--_intermed_mag.jpg)
![Laryngeal squamous carcinoma (High Magnification)[4]](/index.php/File:800px-Laryngeal_squamous_carcinoma_--_high_mag.jpg)
![Laryngeal squamous carcinoma (Very High Magnification)[4]](/index.php/File:800px-Laryngeal_squamous_carcinoma_--_very_high_mag.jpg)
Verrucous squamous cell carcinoma
Features:
- Exophytic growth
- Well-differentiated
- "Glassy" appearance
- Pushing border
Spindle cell squamous carcinoma
- Key to diagnosis is finding a component of conventional squamous cell carcinoma
IHC:
- Typically keratin -ve.
- p63 +ve.
Basaloid squamous cell carcinoma
- May mimic adenoid cystic carcinoma
Lymphoepithelial (squamous cell) carcinoma
- Lymphoid component
IHC
Immunohistochemistry markers include:[5]
- p63 positive
- EBER negative
- p16 negative
- BCL2 positive/negative
References
- ↑ URL: http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Larynx_11protocol.pdf. Accessed on: October 28, 2015.
- ↑ Template:Ref Sternberg4
- ↑ Squamous cell carcinoma subtypes. URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970297-2. Accessed on: October 28, 2015.
- ↑ 4.0 4.1 4.2 Head and neck SCC Librepathology. http://librepathology.org/wiki/index.php/Squamous_cell_carcinoma_of_the_head_and_neck Accessed on October 26, 2015
- ↑ Nichols AC, Finkelstein DM, Faquin WC; et al. (2010). "Bcl2 and human papilloma virus 16 as predictors of outcome following concurrent chemoradiation for advanced oropharyngeal cancer". Clin. Cancer Res. 16 (7): 2138–46. doi:10.1158/1078-0432.CCR-09-3185. PMID 20233885. Unknown parameter
|month=ignored (help)