Laryngeal cancer pathophysiology: Difference between revisions
Jump to navigation
Jump to search
No edit summary |
No edit summary |
||
| Line 23: | Line 23: | ||
*Prevalence - glottis > supraglottis > subglottis. | *Prevalence - glottis > supraglottis > subglottis. | ||
*Glottic carcinoma tends to present earlier (as it affects phonation) and, therefore, has a better prognosis. | *Glottic carcinoma tends to present earlier (as it affects phonation) and, therefore, has a better prognosis. | ||
SCC is subdivided by the WHO into:<ref name=Ref_Sternberg4_975>{{Ref Sternberg4|975}}</ref> | |||
*Keratinizing type (KT). | |||
**Worst prognosis. | |||
*Undifferentiated type (UT). | |||
**Intermediate prognosis. | |||
**EBV association. | |||
*Nonkeratinizing type (NT). | |||
**Good prognosis. | |||
**EBV association. | |||
==Microscopic== | |||
Features based on classification:<ref name=Ref_Sternberg4_975>{{Ref Sternberg4|975}}</ref> | |||
*KT subtype: | |||
**Keratinization & intercellular bridges through-out most of the malignant lesion. | |||
*UT: | |||
**Non-distinct borders/syncytial pattern. | |||
**Nucleoli. | |||
*NT: | |||
**Well-defined cell borders. | |||
====Invasion==== | |||
Features: | |||
*Eosinophilia. | |||
*Extra large nuclei/bizarre nuclei. | |||
*Inflammation (lymphocytes, plasma cells). | |||
*Long rete ridges. | |||
*Numerous beeds/blobs of epithelial cells that seem unlikely to be rete ridges. | |||
Pitfalls: | |||
*Tangential cuts. | |||
**If you can trace the squamous cells from a gland to the surface it is less likely to be invasive cancer. | |||
Notes on invasion: | |||
*Nice review paper by ''Wenig''.<ref name=pmid11904340>{{cite journal |author=Wenig BM |title=Squamous cell carcinoma of the upper aerodigestive tract: precursors and problematic variants |journal=Mod. Pathol. |volume=15 |issue=3 |pages=229–54 |year=2002 |month=March |pmid=11904340 |doi=10.1038/modpathol.3880520 |url=http://www.nature.com/modpathol/journal/v15/n3/pdf/3880520a.pdf}}</ref> | |||
*See ''[[SCC of the cervix versus CIN III]]''. | |||
===Images=== | |||
<gallery> | |||
Image:Oral_cancer_(1)_squamous_cell_carcinoma_histopathology.jpg | Invasive oral SCC. (WC) | |||
</gallery> | |||
<gallery> | |||
Image: Laryngeal squamous carcinoma -- intermed mag.jpg | Laryngeal SCC - intermed. mag. | |||
Image: Laryngeal squamous carcinoma -- high mag.jpg | Laryngeal SCC - high mag. | |||
Image: Laryngeal squamous carcinoma -- very high mag.jpg | Laryngeal SCC - very high mag. | |||
</gallery> | |||
===Overview of subtypes=== | |||
There are several subtypes:<ref>URL: [http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970297-2 http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970297-2]. Accessed on: March 9, 2010.</ref> | |||
*Basaloid - poor prognosis, usu. diagnosed by recognition of typical SCC. | |||
*Warty (Condylomatous). | |||
*Verrucous - good prognosis, rare. | |||
*Papillary. | |||
*Lymphoepithelial, rare. | |||
*Spindle cell, a common spindle cell lesion of the H&N. | |||
====Verrucous squamous cell carcinoma==== | |||
Features: | |||
*Exophytic growth. | |||
*Well-differentiated. | |||
*"Glassy" appearance. | |||
*Pushing border. | |||
DDx: papilloma. | |||
====Spindle cell squamous carcinoma==== | |||
*Key to diagnosis is finding a component of conventional squamous cell carcinoma. | |||
IHC: | |||
*Typically keratin -ve. | |||
*p63 +ve. | |||
DDx: | |||
*Spindle cell [[melanoma]]. | |||
*Mesenchymal neoplasm. | |||
====Basaloid squamous cell carcinoma==== | |||
*May mimic ''[[adenoid cystic carcinoma]]''. | |||
*Classically base of tongue.<ref>URL: [http://www.biomedcentral.com/1471-2407/6/146 http://www.biomedcentral.com/1471-2407/6/146]. Accessed on: March 9, 2010.</ref> | |||
*Typically poor prognosis. | |||
Features: | |||
*Need keratinization. (???) | |||
DDx: | |||
*Neuroendocrine tumour. | |||
====Lymphoepithelial (squamous cell) carcinoma==== | |||
See ''[[nasopharyngeal carcinoma]]''. | |||
==IHC== | |||
*p63 +ve. | |||
*EBER -ve. | |||
**Positive suggests [[nasopharyngeal carcinoma]]. | |||
*p16 -ve. | |||
**Positive suggests [[HPV-associated head and neck squamous cell carcinoma]]. | |||
*Bcl2 +ve/-ve. | |||
**Positive = poor prognosis.<ref name=pmid20233885>{{cite journal |author=Nichols AC, Finkelstein DM, Faquin WC, ''et al.'' |title=Bcl2 and human papilloma virus 16 as predictors of outcome following concurrent chemoradiation for advanced oropharyngeal cancer |journal=Clin. Cancer Res. |volume=16 |issue=7 |pages=2138–46 |year=2010 |month=April |pmid=20233885 |doi=10.1158/1078-0432.CCR-09-3185 |url=}}</ref> | |||
==References== | ==References== | ||
{{reflist|2}} | {{reflist|2}} | ||
Revision as of 17:49, 26 October 2015
|
Laryngeal cancer Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Laryngeal cancer pathophysiology On the Web |
|
American Roentgen Ray Society Images of Laryngeal cancer pathophysiology |
|
Risk calculators and risk factors for Laryngeal cancer pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Faizan Sheraz, M.D. [2]
Overview
Pathophysiology
Gross Pathology

Subclassification by site
It is generally divided the following way:[1]
| Laryngeal cancer | |||||||||||||||||||||||||||||||||
| Supraglottis | Glottis | Subglottis | |||||||||||||||||||||||||||||||
- Prevalence - glottis > supraglottis > subglottis.
- Glottic carcinoma tends to present earlier (as it affects phonation) and, therefore, has a better prognosis.
SCC is subdivided by the WHO into:[4]
- Keratinizing type (KT).
- Worst prognosis.
- Undifferentiated type (UT).
- Intermediate prognosis.
- EBV association.
- Nonkeratinizing type (NT).
- Good prognosis.
- EBV association.
Microscopic
Features based on classification:[4]
- KT subtype:
- Keratinization & intercellular bridges through-out most of the malignant lesion.
- UT:
- Non-distinct borders/syncytial pattern.
- Nucleoli.
- NT:
- Well-defined cell borders.
Invasion
Features:
- Eosinophilia.
- Extra large nuclei/bizarre nuclei.
- Inflammation (lymphocytes, plasma cells).
- Long rete ridges.
- Numerous beeds/blobs of epithelial cells that seem unlikely to be rete ridges.
Pitfalls:
- Tangential cuts.
- If you can trace the squamous cells from a gland to the surface it is less likely to be invasive cancer.
Notes on invasion:
- Nice review paper by Wenig.[5]
- See SCC of the cervix versus CIN III.
Images
-
Invasive oral SCC. (WC)
_squamous_cell_carcinoma_histopathology.jpg)
-
Laryngeal SCC - intermed. mag.
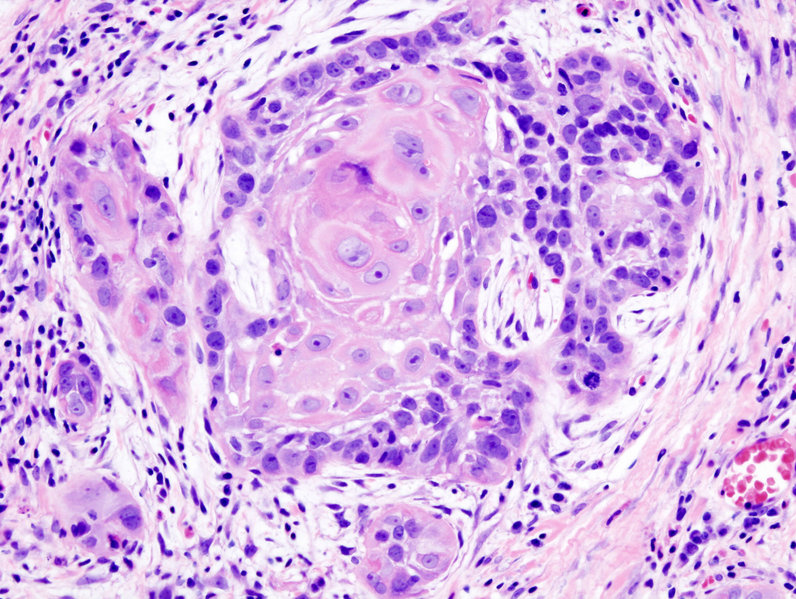
-
Laryngeal SCC - high mag.
-
Laryngeal SCC - very high mag.
{kind=link}
{kind=link}
{kind=link}
Overview of subtypes
There are several subtypes:[6]
- Basaloid - poor prognosis, usu. diagnosed by recognition of typical SCC.
- Warty (Condylomatous).
- Verrucous - good prognosis, rare.
- Papillary.
- Lymphoepithelial, rare.
- Spindle cell, a common spindle cell lesion of the H&N.
Verrucous squamous cell carcinoma
Features:
- Exophytic growth.
- Well-differentiated.
- "Glassy" appearance.
- Pushing border.
DDx: papilloma.
Spindle cell squamous carcinoma
- Key to diagnosis is finding a component of conventional squamous cell carcinoma.
IHC:
- Typically keratin -ve.
- p63 +ve.
DDx:
- Spindle cell melanoma.
- Mesenchymal neoplasm.
Basaloid squamous cell carcinoma
- May mimic adenoid cystic carcinoma.
- Classically base of tongue.[7]
- Typically poor prognosis.
Features:
- Need keratinization. (???)
DDx:
- Neuroendocrine tumour.
Lymphoepithelial (squamous cell) carcinoma
IHC
- p63 +ve.
- EBER -ve.
- Positive suggests nasopharyngeal carcinoma.
- p16 -ve.
- Positive suggests HPV-associated head and neck squamous cell carcinoma.
- Bcl2 +ve/-ve.
- Positive = poor prognosis.[8]
References
- ↑ URL: http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Larynx_11protocol.pdf. Accessed on: 2 May 2012.
- ↑ Template:Ref WMSP
- ↑ URL: http://www.health.am/cr/more/statistics-and-prognosis-for-cancer-of-the-larynx/. Accessed on: 2 May 2012.
- ↑ 4.0 4.1 Template:Ref Sternberg4
- ↑ Wenig BM (2002). "Squamous cell carcinoma of the upper aerodigestive tract: precursors and problematic variants" (PDF). Mod. Pathol. 15 (3): 229–54. doi:10.1038/modpathol.3880520. PMID 11904340. Unknown parameter
|month=ignored (help) - ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970297-2. Accessed on: March 9, 2010.
- ↑ URL: http://www.biomedcentral.com/1471-2407/6/146. Accessed on: March 9, 2010.
- ↑ Nichols AC, Finkelstein DM, Faquin WC; et al. (2010). "Bcl2 and human papilloma virus 16 as predictors of outcome following concurrent chemoradiation for advanced oropharyngeal cancer". Clin. Cancer Res. 16 (7): 2138–46. doi:10.1158/1078-0432.CCR-09-3185. PMID 20233885. Unknown parameter
|month=ignored (help)