Iron deficiency anemia pathophysiology
|
Iron deficiency anemia Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Iron deficiency anemia pathophysiology On the Web |
|
American Roentgen Ray Society Images of Iron deficiency anemia pathophysiology |
|
Risk calculators and risk factors for Iron deficiency anemia pathophysiology |
Please help WikiDoc by adding more content here. It's easy! Click here to learn about editing.
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Pathophysiology
There are several mechanisms that control human iron metabolism and safeguard against iron deficiency. The capacity of the body to absorb iron from the diet depends on the amount of iron in the body, the rate of red blood cell production, the amount and kind of iron in the diet, and the presence of absorption enhancers and inhibitors in the diet. Iron deficiency represents a spectrum ranging from iron depletion, which causes no physiological impairments, to iron deficiency anemia, which affects the functioning of several organ systems. A impairment in any of the above physiology can give rise to Iron deficiency anemia.
Physiology
- In the human body, iron is present in all cells and has several vital functions such as:
- A carrier of oxygen to the tissues from the lungs in the form of hemoglobin (Hb)
- Facilitator of oxygen use and storage in the muscles as myoglobin
- Transport medium for electrons within the cells in the form of cytochromes
- Integral part of enzyme reactions in various tissues.
- Total body iron averages approximately 3.8 g in men and 2.3 g in women.
Iron hemostasis (Absorption and bioavailability)
- There are several mechanisms that control human iron metabolism and safeguard against iron deficiency. The capacity of the body to absorb iron from the diet depends on the amount of iron in the body, the rate of red blood cell production, the amount and kind of iron in the diet, and the presence of absorption enhancers and inhibitors in the diet.
Gastrointestinal tract
- Regulation of iron balance occurs mainly in the gastrointestinal tract through absorption.
- When the absorptive mechanism is operating normally, a person maintains functional iron and tends to establish iron stores.
- The percentage of iron absorbed (i.e., iron bioavailability) can vary from less than 1% to greater than 50%.
- The main factor controlling iron absorption is the amount of iron stored in the body.
- The gastrointestinal tract increases iron absorption when the body's iron stores are low and decreases absorption when stores are sufficient. An increased rate of red blood cell production can also stimulate iron uptake severalfold.
- Among adults, absorption of dietary iron averages approximately 6% for men and 13% for nonpregnant women in their childbearing years.
- The higher absorption efficiency of these women reflects primarily their lower iron stores as a result of menstruation and pregnancy.
- Among iron-deficient persons, iron absorption is also high. Absorption of iron increases during pregnancy, but the amount of the increase is not well defined; as iron stores increase postpartum, iron absorption decreases.
Dietary composition
- Iron bioavailability also depends on dietary composition. Heme iron, which is found only in meat, poultry, and fish, is two to three times more absorbable than non-heme iron, which is found in plant-based foods and iron-fortified foods.
- The bioavailability of non-heme iron is strongly affected by the kind of other foods ingested at the same meal.
- Enhancers of iron absorption are heme iron (in meat, poultry, and fish) and vitamin C; inhibitors of iron absorption include polyphenols (in certain vegetables), tannins (in tea), phytates (in bran), and calcium (in dairy products).
- Vegetarian diets, by definition, are low in heme iron. However, iron bioavailability in a vegeterian diet can be increased by careful planning of meals to include other sources of iron and enhancers of iron absorption.
- In the diet of an infant, before the introduction of solid foods, the amount of iron absorbed depends on the amount and bioavailability of iron in breast milk or formula.
Iron turn over
- Red blood cell formation and destruction is responsible for most iron turnover in the body.
- In adult men, approximately 95% of the iron required for the production of red blood cells is recycled from the breakdown of red blood cells and only 5% comes from dietary sources.
- In contrast, an infant is estimated to derive approximately 70% of red blood cell iron from the breakdown of red blood cells and 30% from the diet.
- In adults, approximately 1 mg of iron is lost daily through feces and desquamated mucosal and skin cells.
- Women of childbearing age require additional iron to compensate for menstrual blood loss (an average of 0.3-0.5 mg daily during the childbearing years) and for tissue growth during pregnancy and blood loss at delivery and postpartum (an average of 3 mg daily over 280 days' gestation).
- In all persons, a minute amount of iron is lost daily from physiological gastrointestinal blood loss.
- Pathological gastrointestinal iron loss through gastrointestinal bleeding occurs in infants and children sensitive to cow's milk and in adults who have peptic ulcer disease, inflammatory bowel syndrome, or bowel cancer.
- Hookworm infections, although not common in the United States, are also associated with gastrointestinal blood loss and iron depletion
Iron stores
- Iron present in the body beyond what is immediately needed for functional purposes is stored as the soluble protein complex ferritin or the insoluble protein complex hemosiderin.
- Ferritin and hemosiderin are present primarily in the liver, bone marrow, spleen, and skeletal muscles. Small amounts of ferritin also circulate in the plasma.
- In healthy persons, most iron is stored as ferritin (an estimated 70% in men and 80% in women) and smaller amounts are stored as hemosiderin. When long-term negative iron balance occurs, iron stores are depleted before iron deficiency begins.
- Men store approximately 1.0-1.4 g of body iron, women approximately 0.2-0.4 g (18,28), and children even less.
- Full-term infants of normal or high birthweight are born with high body iron (an average of 75 mg/kg body weight), to which iron stores contribute approximately 25%.
- Preterm or low-birthweight infants are born with the same ratio of total body iron to body weight, but because their body weight is low, the amount of stored iron is low too.
Iron deficiency represents a spectrum ranging from iron depletion, which causes no physiological impairments, to iron deficiency anemia, which affects the functioning of several organ systems. A impairment in any of the above physiology can give rise to Iron deficiency anemia.
Histology
(Images shown below are courtesy of Melih Aktan MD, Istanbul Medical Faculty - Turkey)
-
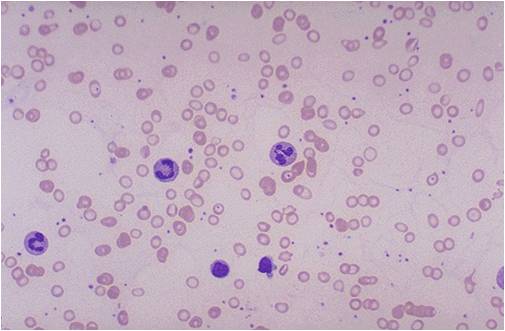
Iron deficiency anemia
-
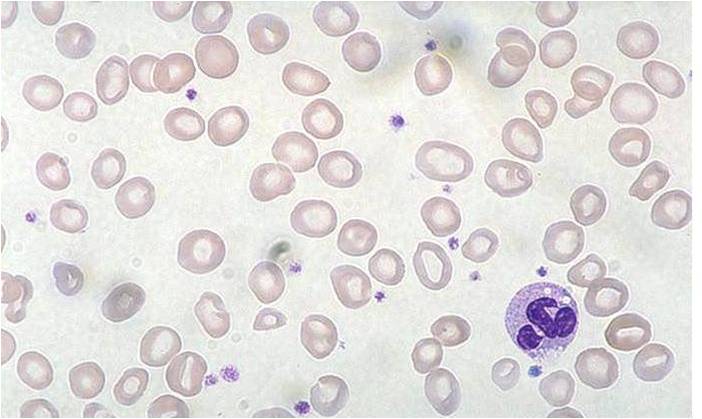
Iron deficiency anemia
-
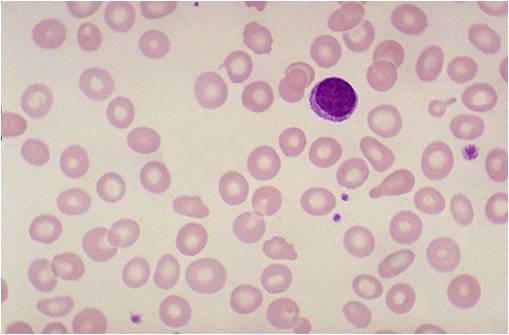
Iron deficiency anemia



Video
{{#ev:youtube|7uDbu7esZik}}
External link
Center for disease control and prevention