Inguinal hernia: Difference between revisions
m (Robot: Automated text replacement (-{{SIB}} + & -{{EH}} + & -{{EJ}} + & -{{Editor Help}} + & -{{Editor Join}} +)) |
|||
| Line 1: | Line 1: | ||
{{CMG}} | {{CMG}} | ||
==Overview== | ==Overview== | ||
| Line 106: | Line 106: | ||
* [http://www.geocities.com/desarda/canal2 Posterior wall of the inguinal canal during raised intra-abdominal pressure] | * [http://www.geocities.com/desarda/canal2 Posterior wall of the inguinal canal during raised intra-abdominal pressure] | ||
{{Gastroenterology}} | {{Gastroenterology}} | ||
Revision as of 16:24, 9 August 2012
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Template:DiseaseDisorder infobox
|
WikiDoc Resources for Inguinal hernia |
|
Articles |
|---|
|
Most recent articles on Inguinal hernia Most cited articles on Inguinal hernia |
|
Media |
|
Powerpoint slides on Inguinal hernia |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Inguinal hernia at Clinical Trials.gov Trial results on Inguinal hernia Clinical Trials on Inguinal hernia at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Inguinal hernia NICE Guidance on Inguinal hernia
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Inguinal hernia Discussion groups on Inguinal hernia Patient Handouts on Inguinal hernia Directions to Hospitals Treating Inguinal hernia Risk calculators and risk factors for Inguinal hernia
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Inguinal hernia |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Inguinal hernias (Template:IPAEng) are protrusions of abdominal cavity contents through the inguinal canal. They are very common and their repair is one of the most frequently performed surgical operations.
There are two types of inguinal hernia, direct and indirect. Direct inguinal hernias occur when abdominal contents herniate through a weak point in the fascia of the abdominal wall and into the inguinal canal. Indirect inguinal hernias occur when abdominal contents protrude through the deep inguinal ring; this is ultimately caused by failure of embryonic closure of the internal inguinal ring.
Origin
In men, inguinal hernias usually arise as a consequence of the descent of the testes from the abdomen into the scrotum during the development of the urinary and reproductive organs. They are more commonly seen in men due to larger size of their inguinal canal, which transmitted the testicle and accommodates the structures of the spermatic cord. Men are 25 times more likely to have an inguinal hernia than women, but since this is such a common problem in the general population (it is estimated that 5% of the population will develop an abdominal wall hernia), inguinal hernia does occur in women to some extent.
Clinical presentation
Hernias present as bulges in the groin area that can become more prominent when coughing, straining, or standing up. They are often painful, and the bulge commonly disappears on lying down. The inability to "reduce" the bulge back into the abdomen usually means the hernia is "incarcerated," often necessitating emergency surgery.
As the hernia progresses, contents of the abdominal cavity, such as the intestines, can descend into the hernia and run the risk of being pinched within the hernia, causing an intestinal obstruction. If the blood supply of the portion of the intestine caught in the hernia is compromised, the hernia is deemed "strangulated," and gut ischemia and gangrene can result, with potentially fatal consequences. The timing of complications is not predictable; some hernias remain static for years, others progress rapidly from the time of onset. Recent data questions the routine elective repair of all inguinal hernias. Some studies indicate that inguinal hernias can be left alone with no greater risk than prompt elective treatment. Nevertheless, the bias remains toward surgical repair. Provided there are no serious co-existing medical problems, patients are advised to get the hernia repaired surgically at the earliest convenience after a diagnosis is made. Emergency surgery for complications such as incarceration and strangulation carry much higher risk than planned, "elective" procedures.
Diagnosis
The diagnosis of inguinal hernia rests on the history given by the patient and the physician's examination of the groin. Further tests are rarely needed to confirm the diagnosis. However, in unclear cases an ultrasound scan or a CT scan might be of help, especially to rule out a hydrocele.
CT images demonstrates a large right inguinal hernia






Surgical treatment
- See main article at herniorrhaphy.
Surgical correction of inguinal hernias, called a herniorrhaphy or hernioplasty, is now often performed as an ambulatory, or "day surgery," procedure. There are various surgical strategies which may be considered in the planning of inguinal hernia repair. These include the consideration of mesh use, type of open repair, use of laparoscopy, type of anesthesia, appropriateness of bilateral repair, etc. During surgery conducted under local anaesthesia, the patient will be asked to cough and strain during the procedure to help in demonstrating that the repair is "tension free" and sound. [1]
Subtypes of inguinal hernias
| Type | Description | Relationship to inferior epigastric vessels | Covered by internal spermatic fascia? | Usual onset |
| indirect inguinal hernia | protrudes through the inguinal ring and is ultimately the result of the failure of embryonic closure of the internal inguinal ring after the testicle passes through it | Lateral | Yes | Congenital |
| direct inguinal hernia | enters through a weak point in the fascia of the abdominal wall | Medial | No | Adult |
Inguinal hernias, in turn, belongs to groin hernias, which also includes femoral hernias. A femoral hernia is not via the inguinal canal, but via the femoral canal, which normally allows passage of the common femoral artery and vein from the pelvis to the leg.
Additional images
-
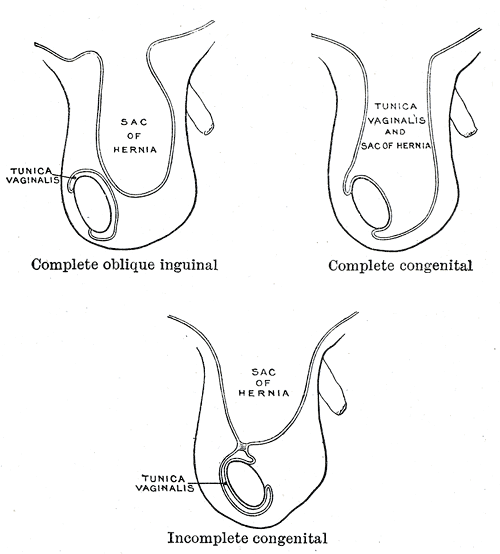
Different types of inguinal hernias.
-
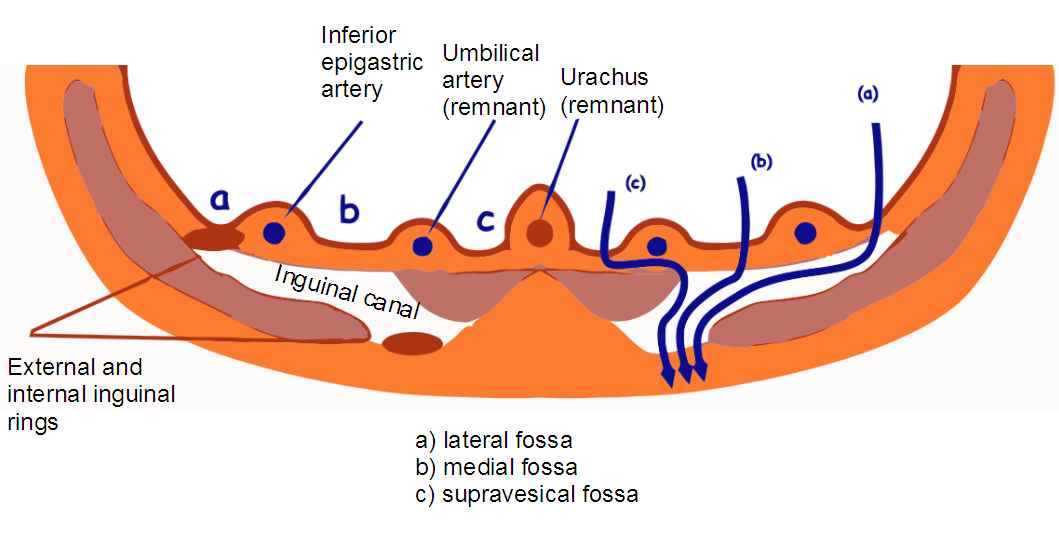
Inguinal fossae


References
External links
External images
- Posterior wall of the inguinal canal at rest
- Posterior wall of the inguinal canal during raised intra-abdominal pressure
de:Leistenbruch el:Βουβωνοκήλη it:Ernia#Ernia inguinale nl:Liesbreuk