Granulomatosis with polyangiitis
Template:DiseaseDisorder infobox
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Click here for The heart in Wegener's granulomatosis
Overview
Wegener's granulomatosis is a form of vasculitis that affects the lungs, kidneys and other organs. Due to its end-organ damage, it can be a serious disease that requires long-term immune suppression.[1] It is named after Dr. Friedrich Wegener, who described the disease in 1936.[2]
Wegener's granulomatosis is part of a larger group of vasculitic syndromes, all of which feature the presence of an abnormal type of circulating antibody termed ANCAs (antineutrophil cytoplasmic antibodies) and affect small and medium-size blood vessels. Apart from Wegener's, this category includes Churg-Strauss syndrome and microscopic polyangiitis.[1] Although Wegener's granulomatosis affects small and medium-sized vessels,[3] it is formally classified as one of the small vessel vasculitides in the Chapel Hill system.[4]
History
Scottish otolaryngologist Peter McBride (1854–1946) first described the condition in 1897 in a British Medical Journal article entitled "Photographs of a case of rapid destruction of the nose and face"[5]. Heinz Karl Ernst Klinger (1907– ) would add information on the anatomical pathology, but the full picture was presented by Friedrich Wegener (1907–1990), a German pathologist, in two reports in 1936 and 1939.[2]
An earlier name for the disease was pathergic granulomatososis.[6] The disease is still sometimes confused with lethal midline granuloma and lymphomatoid granulomatosis, both malignant lymphomas.[7]
In 2006, Dr. Alexander Woywodt (Preston, United Kingdom) and Dr. Eric Matteson (Mayo Clinic, USA) investigated Dr. Wegener's past, and discovered that he was, at least at some point of his career, a follower of the Nazi regime. In addition, their data indicate that Dr. Wegener was wanted by Polish authorities and that his files were forwarded to the United Nations War Crimes Commission. Finally, Dr. Wegener worked in close proximity to the genocide machinery in Lodz. Their data raise serious concerns about Dr. Wegener's professional conduct. They suggest that the eponym be abandoned and propose "ANCA-associated granulomatous vasculitis."[8] The authors have since campaigned for other medical eponyms to be abandoned, too.[9]
Epidemiology
The incidence is 10 cases per million per year.[10] 90% of the patients are whites. While it mainly occurs in the middle-aged, it has been reported in much younger and older patients.
Pathophysiology
Inflammation with granuloma formation against a nonspecific inflammatory background is the classical tissue abnormality in all organs affected by Wegener's granulomatosis.[1]
It is now widely presumed that the anti-neutrophil cytoplasmic antibodies (ANCAs) are responsible for the inflammation in Wegener's.[1] The typical ANCAs in Wegener's are those that react with proteinase 3, an enzyme prevalent in neutrophil granulocytes.[11] This type of ANCA is also known as cANCA, with the c indicating cytoplasmic (in contrast to pANCA, which is perinuclear).
ANCAs activate neutrophils, increase their adherence to endothelium, and lead to their degranulation. This causes extensive damage to the vessel wall, particularly of arterioles.[1]
The exact cause for the production of ANCAs is unknown, although some drugs have been implicated in secondary forms of Wegener's. As with many autoimmune disorders, the cause is probably genetic predisposition combined with molecular mimicry caused by a virus or bacterium.
Signs and symptoms
Initial signs are protean, and diagnosis can be severely delayed due to the non-specific nature of the symptoms. The rhinitis is generally the first sign in most patients.[1]
- Upper airway, eye and ear disease:
- Nose: pain, stuffiness, nosebleeds, rhinitis, crusting, saddle-nose deformity due to a perforated septum
- Ears: conductive hearing loss due to Eustachian tube dysfunction, sensorineural hearing loss (unclear mechanism)
- Eyes: pseudotumours, scleritis, conjunctivitis, uveitis, episcleritis
- Airways:
- Trachea: subglottal stenosis
- Lungs: pulmonary nodules (referred to as "coin lesions"), infiltrates (often interpreted as pneumonia), cavitary lesions, pulmonary hemorrhage causing hemoptysis), and rarely bronchial stenosis.
- Kidney: rapidly progressive segmental necrotising glomerulonephritis (75%), leading to chronic renal failure
- Arthritis: Pain or swelling (60%), often initially diagnosed as rheumatoid arthritis
- Skin: nodules on the elbow, purpura, various others (see cutaneous vasculitis)
- Nervous system: occasionally sensory neuropathy (10%) and rarely mononeuritis multiplex
- Heart, gastrointestinal tract, brain other organs: rarely affected.
Symptoms in Detail
The first symptoms of Wegener's granulomatosis are often vague and frequently include upper respiratory tract symptoms, joint pains, weakness, and tiredness.
Upper respiratory tract
The most common sign of Wegener's granulomatosis is involvement of the upper respiratory tract, which occurs in nearly all patients. Symptoms include sinus pain, discolored or bloody fluid from the nose, and, occasionally, nasal ulcers. A common sign of the disease is almost constant rhinorrhea ("runny nose") or other cold symptoms that do not respond to usual treatment or that become increasingly worse.
Rhinorrhea can result from nasal inflammation or sinus drainage and can cause pain. A hole may develop in the cartilage of the nose, which may lead to collapse (called saddle-nose deformity). The eustachian tubes, which are important for normal ear function, may become blocked, causing chronic ear problems and hearing loss. Bacterial infection can cause Wegener's-related sinusitis (inflammation of the sinuses) with congestion and chronic sinus pain.
Lungs
The lungs are affected in most people with Wegener's granulomatosis, although no symptoms may be present. If symptoms are present, they include cough, hemoptysis (coughing up blood), shortness of breath, and chest discomfort.
Kidneys
Kidney involvement, which occurs in more than three-fourths of people with this disorder, usually does not cause symptoms. If detected by blood and urine tests, a doctor can start proper treatment, preventing long-term damage to the kidneys.
Musculoskeletal system
Pain in the muscles and joints or, occasionally, joint swelling affects two-thirds of people with Wegener's granulomatosis. Although joint pain can be very uncomfortable, it does not lead to permanent joint damage or deformities.
Eyes
Wegener's granulomatosis can affect the eyes in several ways. People may develop;
- Conjunctivitis (inflammation of the conjunctiva, the inner lining of the eyelid)
- Scleritis (inflammation of the scleral layer, the white part of the eyeball)
- Episcleritis (inflammation of the episcleral layer, the outer surface of the sclera)
- Mass lesion behind the eye globe
Symptoms in the eye include redness, burning, or pain. Double vision or a decrease in vision are serious symptoms requiring immediate medical attention.
Skin lesions
Nearly half of people with Wegener's granulomatosis develop skin lesions. These often have the appearance of small red or purple raised areas or blister-like lesions, ulcers, or nodules that may or may not be painful.
Other symptoms
Some people experience narrowing of the trachea. The symptoms can include voice change, hoarseness, shortness of breath, or cough.
The nervous system and heart occasionally may be affected. Fever and night sweats may occur. Fever also may signal an infection, often of the upper respiratory tract.
Diagnosis
Vasculitis such as Wegener's granulomatosis is usually only suspected when a patient has had unexplained symptoms for a longer period of time. Determination of ANCAs can aid in the diagnosis, but positivity is not conclusive and negative ANCAs are not sufficient to reject the diagnosis. Cytoplasmic staining ANCAs that react with the enzyme proteinase 3 (cANCA) in neutrophils (a type of white blood cell) are associated with Wegener's.[1]
If the patient has renal failure or cutaneous vasculitis, these are the most logical organs to obtain a biopsy from. Rarely, thoracoscopic lung biopsy is required. On histopathological examination, a biopsy will show leukocytoclastic vasculitis with necrotic changes and granulomatous inflammation (clumps of typically arranged white blood cells) on microscopy. The latter is the main reason for the appellation of "Wegener's granulomatosis", although it is not an essential feature. Unfortunately, many biopsies can be non-specific and 50% provide too little information for the diagnosis of Wegener's.[1]
Differential diagnosis (alternative possible diagnoses) can be extensive. ANCAs can be positive after the use of certain drugs, and other forms of vasculitis can present with very similar symptoms. The saddle nose deformity may also seen in cocaine abuse and in congenital syphilis.
Diagnostic Criteria
In 1990, the American College of Rheumatology accepted classification criteria for Wegener's. They were not intended for diagnosis, but for inclusion in randomized controlled trials. Two or more positive criteria have a sensitivity of 88.2% and a specificity of 92.0% of describing Wegener's.[12]
- Nasal or oral inflammation:
- painful or painless oral ulcers or
- purulent or bloody nasal discharge
- Lungs: abnormal chest X-ray with:
- nodules,
- infiltrates or
- cavities
- Kidneys: urinary sediment with:
- microhematuriaor
- red cell casts
- Biopsy: granulomatous inflammation
- within the arterial wall or
- in the perivascular area
According to the Chapel Hill Consensus Conference (CHCC) on the nomenclature of systemic vasculitis (1992), establishing the diagnosis of Wegener's granulomatosis demands:[13]
- a granulomatous inflammation involving the respiratory tract, and
- a vasculitis of small- to medium-sized vessels.
Several investigators have compared the ACR and Chapel Hill criteria.[14]
Diagnostic Findings
Computed Tomography
-

CT: Wegener's granulomatosis
-
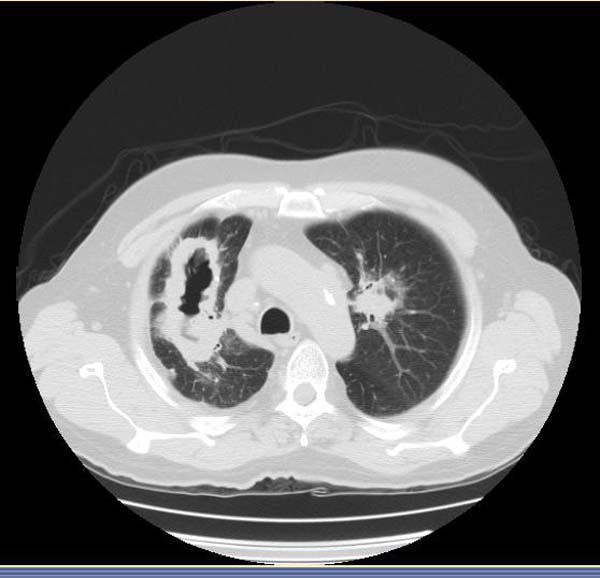
CT: Wegener's granulomatosis
-

CT: Wegener's granulomatosis



Immunofluorescence
-
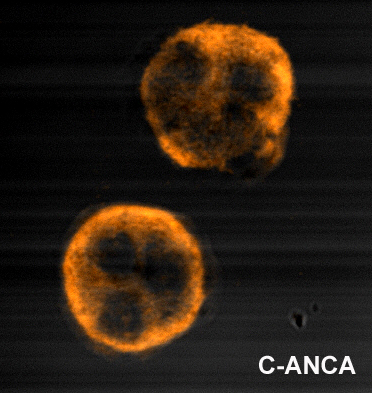
Immunofluorescence pattern produced by binding of ANCA from a patient with Wegener's Granulomatosis to ethanol-fixed neutrophils

Treatment
Before steroid treatment became available, mortality within one year was over 90%, with average survival being 5 months. Steroids prolonged average survival to 8 months. The introduction of cyclophosphamide (CYC) in the 1970s was a major breakthrough.[10]
Initial treatment is generally with corticosteroids and oral cyclophosphamide (CYC), 1 mg/kg/day and 2 mg/kg/day, respectively. Occasionally CYC is given in monthly intravenous (IV) doses. Monitoring of the white blood count is essential during CYC therapy. Once remission is attained (normally 3 to 6 months), treatment is frequently changed to azathioprine or methotrexate, which are less toxic drugs. Total duration of therapy should be at least one year, or longer in high risk patients. Corticosteroids are tapered to a low maintenance dose, 5-10 mg/day. Plasmapheresis may be beneficial in severe disease or pulmonary hemorrhage. Experience with other treatment agents is very limited.[1].
A systematic review of 84 trials examined the evidence for various treatments in Wegener's granulomatosis. Many trials include data on pooled groups of patients with Wegener's and microscopic polyangiitis. In this review, cases are divided between localized disease, non-organ threatening, generalized organ-threatening disease and severe renal vasculitis and immediately life-threatening disease.[10]
- In localized disease, treatment with the antibiotic co-trimoxazole is recommended, with steroids in case of treatment failure.[15]
- In generalized non-organ threatening disease, remission can be induced with methotrexate and steroids, where the steroid dose is reduced after a remission has been achieved and methotrexate used as maintenance.
- In case of organ-threatening disease, pulsed intravenous cyclophosphamide with steroids is recommended. Once remission has been achieved, azathioprine and steroids can be used to maintain remission.
- In severe renal vasculitis, the same regimen is used but with the addition of plasma exchange.
- In pulmonary hemorrhage, high doses of cyclophosphamide with pulsed methylprednisolone may be used, or alternatively CYC, steroids, and plasma exchange.
In severe disease not responsive to previously mentioned treatment, the review is positive about mycophenolate mofetil, 15-deoxyspergualin, anti-thymocyte globulin, rituximab and infliximab; data was less favourable for intravenous immunoglobulin (IVIG) and etanercept.[10]
In some patients with severe subglottic stenosis, tracheotomy is required to maintain an airway.
Follow-up: general well-being and laboratory organ markers are checked on a regular basis to ascertain the patient has remained in remission.
Prognosis
25 to 40% of patients suffer from flare-ups, but a majority responds well to treatment. Anatomical problems (sinusitis, tracheal stenosis) may require surgery in a small proportion. Relapses can be long and troublesome.
Long-term complications are very common (86%): mainly chronic renal failure, hearing loss and deafness.[1]
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 Seo P, Stone JH. The antineutrophil cytoplasmic antibody-associated vasculitides. Am J Med 2004;117:39-50. PMID 15210387.
- ↑ 2.0 2.1 Template:WhoNamedIt
- ↑ "Wegener's Granulomatosis: Vasculitis: Merck Manual Professional". Retrieved 2009-01-08.
- ↑ Silva, Fred; Jennette, J. Charles; Heptinstall, Robert H.; Olson, Jean T.; Schwartz, Melvin (2007). Hepinstall's pathology of the kidney. Hagerstwon, MD: Lippincott Williams & Wilkins. p. 677. ISBN 0-7817-4750-3.
- ↑ Friedmann I (1982). "McBride and the midfacial granuloma syndrome. (The second 'McBride Lecture', Edinburgh, 1980)". The Journal of laryngology and otology. 96 (1): 1–23. PMID 7057076.
- ↑ Fienberg R (1955). "Pathergic granulomatosis". Am. J. Med. 19 (6): 829–31. doi:10.1016/0002-9343(55)90150-9. PMID 13275478.
- ↑ Mendenhall WM, Olivier KR, Lynch JW Jr, Mendenhall NP (2006). "Lethal midline granuloma-nasal natural killer/T-cell lymphoma". Am J Clin Oncol. 29 (2): 202–6. doi:10.1097/01.coc.0000198738.61238.eb. PMID 16601443.
- ↑ Woywodt A, Matteson EL (2006). "Wegener's granulomatosis--probing the untold past of the man behind the eponym". Rheumatology (Oxford). 45 (10): 1303–6. doi:10.1093/rheumatology/kel258. PMID 16887845.
- ↑ Woywodt A, Matteson E (2007). "Should eponyms be abandoned? Yes". BMJ. 335 (7617): 424. doi:10.1136/bmj.39308.342639.AD. PMID 17762033.
- ↑ 10.0 10.1 10.2 10.3 Bosch X, Guilabert A, Espinosa G, Mirapeix E (2007). "Treatment of antineutrophil cytoplasmic antibody associated vasculitis: a systematic review". JAMA. 298 (6): 655–69. doi:10.1001/jama.298.6.655. PMID 17684188.
- ↑ van der Woude FJ, Rasmussen N, Lobatto S, Wiik A, Permin H, van Es LA, van der Giessen M, van der Hem GK, The TH. Autoantibodies against neutrophils and monocytes: tool for diagnosis and marker of disease activity in Wegener's granulomatosis. Lancet 1985;1(8426):425-9. PMID 2857806.
- ↑ Leavitt RY, Fauci AS, Bloch DA, Michel BA, Hunder GG, Arend WP, et al. The American College of Rheumatology 1990 criteria for the classification of Wegener's granulomatosis. Arthritis Rheum 1990;33:1101-7. PMID 2202308.
- ↑ Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, Hagen EC, Hoffman GS, Hunder GG, Kallenberg CG, et al. Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum 1994;37:187-92. PMID 8129773.
- ↑ Bruce IN, Bell AL. A comparison of two nomenclature systems for primary systemic vasculitis. Br J Rheumatol 1997;36:453-8. PMID 9159539.
- ↑ Stegeman CA, Tervaert JW, de Jong PE, Kallenberg CG (1996). "Trimethoprim-sulfamethoxazole (co-trimoxazole) for the prevention of relapses of Wegener's granulomatosis. Dutch Co-Trimoxazole Wegener Study Group". N. Engl. J. Med. 335 (1): 16–20. PMID 8637536.
External links
- Classification criteria by the American College of Rheumatology
- Vasculitis Foundation Formerly the Wegener's Granulomatosis Association
- Wegener's Granulomatosis Info
- WegenersNet A Wegener's Granulomatosis Community Portal
Template:SIB Template:Diseases of the musculoskeletal system and connective tissue
Template:Skin and subcutaneous tissue symptoms and signs Template:Nervous and musculoskeletal system symptoms and signs Template:Urinary system symptoms and signs Template:Cognition, perception, emotional state and behaviour symptoms and signs Template:Speech and voice symptoms and signs Template:General symptoms and signs