Fibroma pathophysiology: Difference between revisions
Simrat Sarai (talk | contribs) No edit summary |
Simrat Sarai (talk | contribs) No edit summary |
||
| Line 82: | Line 82: | ||
*Foam cells and hemosiderin deposition are present. | *Foam cells and hemosiderin deposition are present. | ||
*Mitoses are seen but cytologic atypia is absent. | *Mitoses are seen but cytologic atypia is absent. | ||
<gallery> | |||
File:1050px-Bone Metaphyseal Fibrous Defect High Power.JPG| Metaphyseal fibrous defect - high magnification. | |||
File:1068px-Bone Metaphyseal Fibrous Defect Medium Power.JPG|Metaphyseal fibrous defect - intermediate magnification. | |||
</gallery> | |||
===Location=== | ===Location=== | ||
*Metaphysis of distal femur or proximal tibia (80%) | *Metaphysis of distal femur or proximal tibia (80%) | ||
Revision as of 01:26, 29 February 2016
|
Fibroma Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Fibroma pathophysiology On the Web |
|
American Roentgen Ray Society Images of Fibroma pathophysiology |
|
Risk calculators and risk factors for Fibroma pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Simrat Sarai, M.D. [2]
Overview
On gross pathology, solid white mass which is usually well-circumscribed is characteristic findings of ovarian fibroma. On microscopic histopathological analysis, ovarian fibroma is composed of spindle cells forming variable amounts of collagen. Sectioning of a fibroma typically reveals a chalky-white surface that has a whorled appearance, similar to that of a uterine fibroid. Areas of edema, occasionally with cyst formation, are also relatively common. On gross pathology, polypoid lesion which is usually small, is characteristic findings of oral fibroma. On microscopic histopathological analysis, fibrous stroma, collagen bundles, prominent vessels, and overlying squamous mucosa with hyperkeratosis and focal ulceration are characteristic findings of oral fibroma. On gross pathology, well circumscribed, metaphyseal lesion, and fragments of white-grey rubbery tissue are characteristic findings of chondromyxoid fibroma. On microscopic histopathological analysis, spindle cells or stellate cells in a myxoid or chondroid stroma, lobules with hypocellular centers and hypercellular peripheries, giant cells in a hypercellular periphery, and scattered calcifications are characteristic findings of chondromyxoid fibroma.
Pathophysiology
Ovarian Fibroma
Gross Pathology
On gross pathology, solid white mass which is usually well-circumscribed is characteristic findings of ovarian fibroma.
Microscopic Pathology
On microscopic histopathological analysis, fibroma is composed of spindle cells forming variable amounts of collagen. Sectioning of a fibroma typically reveals a chalky-white surface that has a whorled appearance, similar to that of a uterine fibroid. Areas of edema, occasionally with cyst formation, are also relatively common.
-
Histopathology specimen of an ovarian fibroma high magnification
-

Histopathology specimen of an ovarian fibroma intermediate magnification


Oral Fibroma (Focal fibrous hyperplasia, Peripheral fibroma, Peripheral ossifying fibroma, Fibroid epulis, Fibroepithelial polyp)
Gross Pathology
On gross pathology, polypoid lesion which is usually small, is characteristic findings of oral fibroma.
Microscopic Pathology
Following features are noted on microscopic histopathological analysis of oral fibroma:
- Fibrous stroma is a key feature
- Collagen bundles may be present
- Vessels may be prominent
- Overlying squamous mucosa is benign
- Hyperkeratosis may be present
- Focal ulceration may be present
-
Histopathology specimen of a oral fibroma low magnification
-

Histopathology specimen of a oral fibroma very low magnification
-

Histopathology specimen of a oral fibroma intermediate magnification



Chondromyxoid Fibroma
Gross Pathology
On gross pathology, well circumscribed, metaphyseal lesion, and fragments of white-grey rubbery tissue are characteristic findings of chondromyxoid fibroma.
Microscopic Pathology
Following features are noted on microscopic histopathological analysis of chondromyxoid fibroma:
- Spindle cells or stellate cells in a myxoid or chondroid stroma
- Lobules with hypocellular centers and hypercellular peripheries
- Giant cells in the hypercellular periphery
- Scattered calcifications.
- No true hyaline cartilage formation is seen
- No mitotic activity is seen
-
Histopathology specimen of a chondromyxoid fibroma showing stellate cells in myxoid stroma
-
Histopathology specimen of a chondromyxoid fibroma showing lobule with calcification
-

Histopathology specimen of a chondromyxoid fibroma showing stellate cells in myxohyaline stroma
-
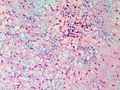
Histopathology specimen of a chondromyxoid fibroma showing stellate cells in myxoid stroma
-
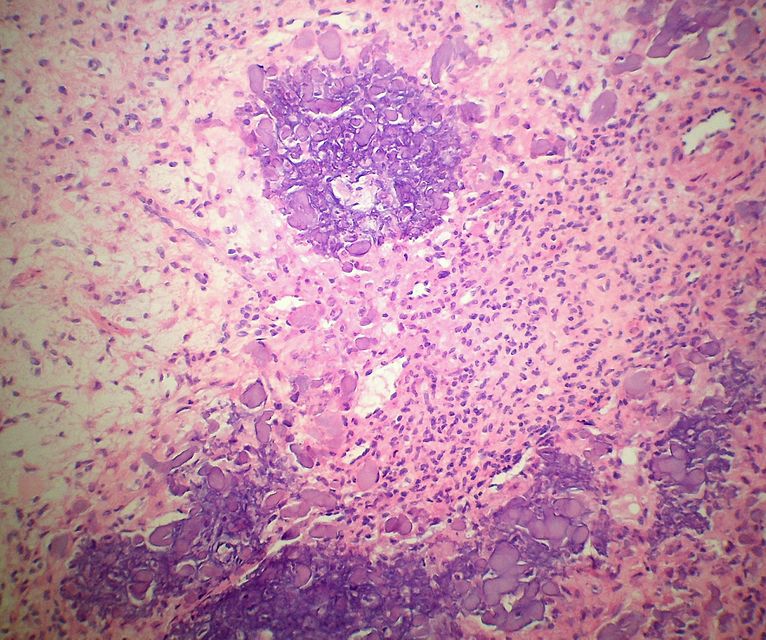
Histopathology specimen of a chondromyxoid fibroma showing focus of amorphous calcification
-

Histopathology specimen of a chondromyxoid fibroma showing foci of amorphous calcification
-
Histopathology specimen of a chondromyxoid fibroma showing stellate cells in myxohyaline stroma
-

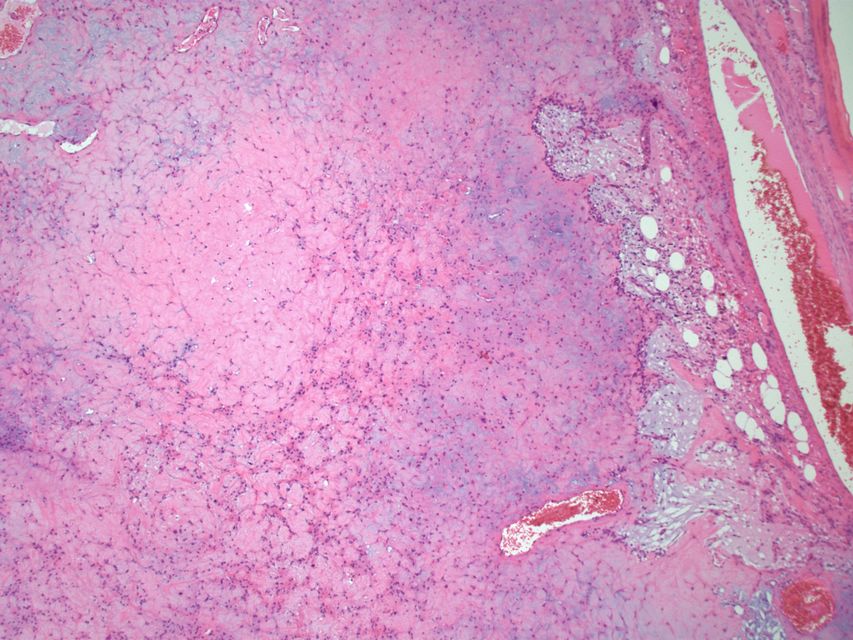
Histopathology specimen of a chondromyxoid fibroma showing Lobule with a darker (hypercellular) periphery and lighter (hypocellular) center. (SKB)
.jpg)







Ossifying Fibroma (Osteofibrous dysplasia, Congenital osteitis fibrosa)
Gross Pathology
On gross pathology, discrete mass that is well delineated from surrounding bone, tan-white, rubbery cut surface, firm to gritty and no encapsulation are characteristic findings of ossifying fibroma.
Microscopic Pathology
Following features are noted on microscopic histopathological analysis of ossifying fibroma:
- They comprise of haphazardly distributed lamellated bony spicules on a background of fibrous stroma.
- Despite being benign, they can be locally aggressive.
- Immunohistochemical staining of lesions shows positive keratin cells in the majority of the cases.
- The lesion has a zonal architecture with a center of immature bone surrounded by more mature lamellar bone.
- The central spicules of woven bony trabeculae are lined by a layer of osteoblasts. The background is a loose and storiform fibrous tissue.
Location
- Lower extremity
- Tibia: It is the most frequent site (approximately 90% of the time); there is a predilection for the cortex of the tibial diaphysis.
- Femur: It occurs in a diaphyseal location
Immunohistochemistry
- Ossifying fibromas are keratin positive - isolated cells accepted by some.
Associated Conditions
- It is associated with clonal chromosomal abnormalities such as trisomies of chromosomes 7, 8, 12,21, and/or 22
Pathogenesis
- Ossifying fibroma may be either a clonal neoplastic lesion or a developmental dysplasia.
Associated Conditions
- It be related to adamantinoma
Non-ossifying Fibroma (nonossifying fibroma, fibrous cortical defect, fibrous metaphyseal defect, fibroxanthoma of bone)
Gross Pathology
On gross pathology, fleshy, fibrous, yellow or tan-brown lesion with variable areas of haemorrhage are characteristic findings of non-ossifying fibroma.
Microscopic Pathology
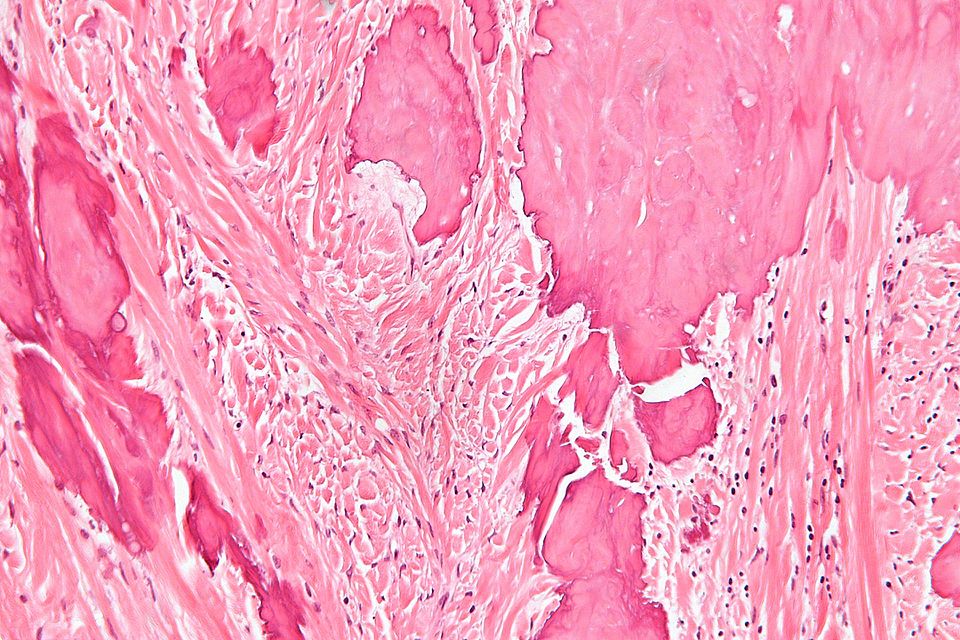
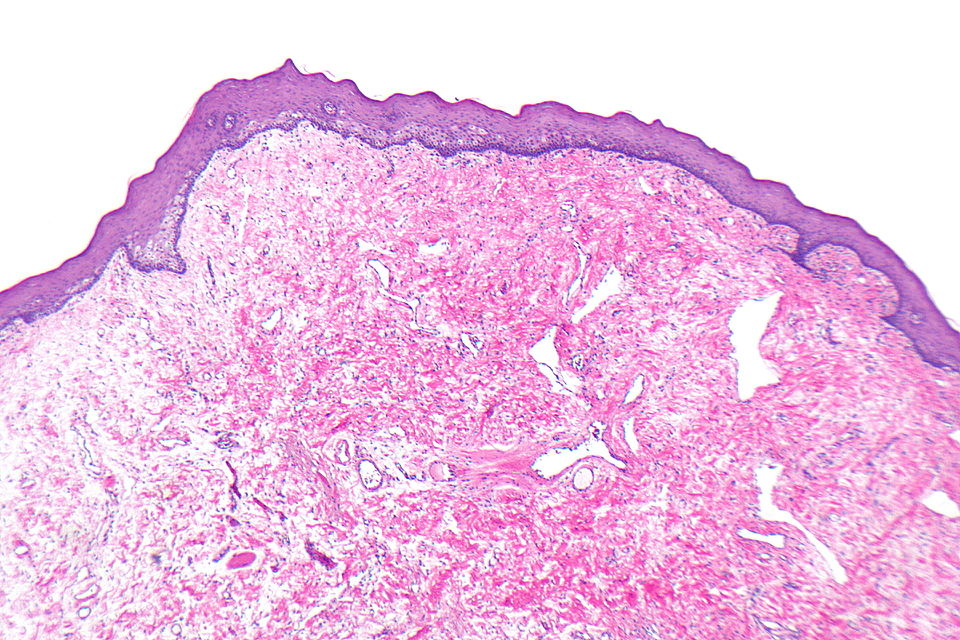
The following features are seen on microscopic histopathological analysis of non-ossifying fibroma:
- Spindle cells without cytologic atypia are arranged in a storiform pattern.
- Scattered chronic inflammatory cells and benign giant cells.
- Foam cells and hemosiderin deposition are present.
- Mitoses are seen but cytologic atypia is absent.
-

Metaphyseal fibrous defect - high magnification.
-

Metaphyseal fibrous defect - intermediate magnification.


Location
- Metaphysis of distal femur or proximal tibia (80%)
- Cortical
- Metaphysis
- Long bone
- Eccentric location
Associated Conditions
- Neurofibromatosis-type 1 (NF1)
- Fibrous dysplasia
- Jaffe-Campanacci syndrome
Desmoplastic Fibroma
Microscopic Pathology
The following features are seen on microscopic histopathological analysis of desmoplastic fibroma:
- Lamellar bone
- Fibrotic marrow space has following features:
- Collagen
- Low cellularity
- Spindle cells without significant atypia
- On histopathology, desmoplastic fibromas are identical to soft tissue desmoid tumors, with abundant collagenous stroma and little cellularity or pleomorphism.
- The main cell types that are seen include the following:
- Fibroblasts
- Myofibroblasts
- Undifferentiated mesenchymal cells
Pleural Fibroma
Microscopic Pathology
The following features are seen on microscopic histopathological analysis of pleural fibroma:
- Pleural fibromas are composed of irregularly arranged fascicles comprising of spindle cells with collagen separation.
- They originate from submesothelial mesenchymal cells.
- Myxoid or cystic degeneration can occur.
Location
- Approximately 80% of pleural fibromas arise from the visceral pleura, with the remainder arising from the parietal pleura.
- There may be a predilection towards the mid to lower zones of the chest.
Cardiac Fibroma
Microscopic Pathology
The following features are seen on microscopic histopathological analysis of cardiac fibromas:
- Cardiac fibromas are well defined, solitary, intramyocardial lesions with smooth margins and usually large, with a mean diameter of ~5 cm and may obliterate the ventricular cavity.
- Unlike many primary cardiac tumours, fibromas usually have no foci of cystic change, hemorrhage, or necrosis. Calcification is a common findings.
Associated Conditions
There is an increased prevalence of cardiac fibromas in Gorlin syndrome.
Location
The majority of cardiac fibromas arise in the ventricular septum and left ventricular free wall.
Cemento-ossifying Fibroma
Microscopic Pathology
The following features are seen on microscopic histopathological analysis of cemento-ossifying fibroma:
- Cemento -ossifying tumours are composed of fibrous tissue, calcified tissue resembling bone and/or cementum.
- The bone-like component is predominant reminiscent of woven bone and is found in more 'mature' lesions.
- In some instances, this entity has been divided into cementifying fibroma and ossifying fibroma depending on the relative amounts of the tumor's constituent tissues. However, in majority of cases both features are present, warranting the generic term cemento-ossifying fibromas.
Pathogenesis
- Cemento-ossifying tumors are thought to arise from the periodontal ligament, accounting for the usual vicinity to teeth.
Renal Medullary Fibroma
Gross pathology
On gross pathology, small, and white well circumscribed nodule in medulla typically less than 3mm are characteristic findings of renal medullary fibroma.
Microscopic Pathology
The following features are seen on microscopic histopathological analysis of renal medullary fibroma:
- Small polygonal/stellate cells
- Abundant loose/myxoid stroma
- Entrapped renal tubules may be present
Ameloblastic Fibroma
Microscopic Pathology
The following features are seen on microscopic histopathological analysis of ameloblastic fibroma:
- Palisaded nuclei
- Fibrous stroma
Desmoplastic Fibroblastoma (Collagenous Fibroma)
Location
Classically found in the shoulder region.
Microscopic Pathology
The following features are seen on microscopic histopathological analysis of desmoplastic fibroblastoma:
- Spindle cells or stellate cells without nuclear atypia
- Acellular stroma with abundant collagen
- Myxoid areas may be present
- Mitoses is rare
Immunohistochemistry
The following findings are noted on immunohistochemistry of desmoplastic fibroblastoma:
- Beta-catenin -ve
- Positive in desmoid-type fibromatosis
- Desmin negative
- S-100 negative
- CD34 negative
- MSA positive
- Alpha-SMA positive
Pathogenesis
- FOSL1 gene is involved in the pathogenesis of desmoplastic fibroblastoma, llq12 breakpoint described as being characteristic.