Essential thrombocytosis pathophysiology
|
Essential thrombocytosis Microchapters |
|
Differentiating Essential thrombocytosis from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Essential thrombocytosis pathophysiology On the Web |
|
American Roentgen Ray Society Images of Essential thrombocytosis pathophysiology |
|
Risk calculators and risk factors for Essential thrombocytosis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Soujanya Thummathati, MBBS [2]
Overview
Essential thrombocytosis is a clonal proliferation of pluripotent stem cells with predominantly megakaryocytic differentiation and proliferation in the bone marrow resulting in an abnormally increased number of platelets released into the circulation.[1] The defective platelets eventually result in vascular complications like blood clots and to a lesser extent, bleeding. Defective platelet granules make the aggregation process ineffective and thus impair the clotting process. Thrombopoietin (TPO) levels are paradoxically high or normal in essential thrombocytosis. A point mutation in the janus kinase 2 (JAK2) gene has been identified in about 50% of the patients that is being studied for a probable targeted gene therapy in future.
Pathophysiology
- As defined by WHO, essential thrombocytosis is a clonal proliferation of pluripotent stem cells with predominantly megakaryocytic differentiation in the bone marrow, resulting in an abnormally increased number of platelets released into the circulation.[1]
- Recent studies have shown that other cell lineages can also be affected to some degree, resulting in their respective cell proliferation.
- Thrombopoietin (TPO) is a hormone produced predominantly by the liver, bone marrow and kidney, that regulates the stimulation, production and proliferation of megakaryocytes. Once thrombopoietin binds to the TPO receptors on the megakaryocytes, it is destroyed thus making the megakaryocyte unavailable for further hormonal interaction.[2]
- Given the higher platelet count, essential thrombocytosis should hypothetically present with lower thrombopoietin levels. However, there is a paradoxical increase in free circulating levels of thrombopoietin as the abnormal platelets in essential thrombocytosis have defective TPO receptors that do not allow proper binding of thrombopoietin.
- Platelets contain different types of granules: alpha (contain P-selectin, platelet factor 4, transforming growth factor-β1, platelet-derived growth factor, fibronectin, B-thromboglobulin, vWF, fibrinogen, and coagulation factors V and XIII), delta (δ) or dense granules (contain ADP or ATP, calcium, and serotonin), gamma (γ) and lambda (λ) granules[3]. With defective granules in essential thrombocytosis, there is a deficiency in clotting factors like fibrinogen and von Willebrand (vWF) that impairs the process of aggregation.
- On the other hand, patients with secondary or reactive thrombocytosis have normal platelet activity with no defects in aggregation.
- No specific pathologic markers were identified for essential thrombocytosis for a long time until some studies showed mutations in the janus kinase 2 (JAK2) gene. Though not a standardized test, about 50% of the patients have this mutation.
- Janus kinase 2 a non-receptor tyrosine kinase protein belonging to the Janus kinase family that helps in signaling pathways involved in hematopoiesis (including thrombopoietin, erythropoietin, granulocyte-colony stimulating factor, Bcl-2, interleukin-3,5).[4] Mutation in JAK2 results in the activation of the janus kinase that results in abnormal differentiation and proliferation of the precursor cells, resulting in the increased pool of platelets in the circulation.
- A point mutation G to T, results in the substitution of valine for phenylalanine at amino acid 617 of the JAK2 protein that activates the tyrosine kinase in JAK2.
- JAK2 mutations are also found in other malignancies and they should be ruled out before making a diagnosis of essential thrombocytosis. The mutation may be used in the diagnosis and probably in targeted gene therapy in future.
-
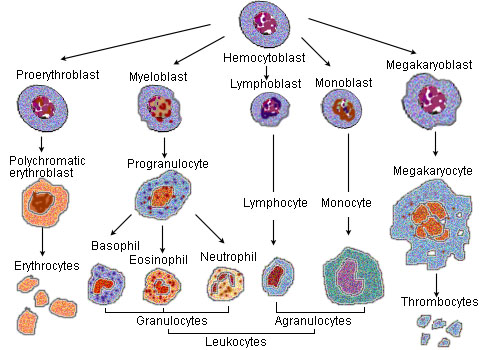
CFU-Me (pluripotential hemopoietic stem cell or hemocytoblast) -> megakaryoblast -> promegakaryocyte -> megakaryocyte.

Genetics
- Essential thrombocytosis is associated with mutations in janus kinase 2 (JAK2) gene in 50% of the patients.
- For unknown reasons, a point mutation in the amino acid 617 of JAK2 protein, results in the substitution of valine for phenylalanine from a G to T replacement. This activates the janus kinase protein, signaling the process of hematopoiesis that results in the differentiation and proliferation of platelets.
- In recent studies, another mutation in the Calreticulin (CALR) gene has been identified in patients with essential thrombocytosis who lacked JAK2 mutations.[5] The mechanism by which the mutation triggers the disease remains unknown.
Microscopic findings of essential thrombocytosis
- A complete blood count shows marked elevation of platelet count greater than or equal to 600,000/μL of blood and sometimes even higher.
- The platelet shape and size usually remain unchanged, but variations may occur.
- The red cell morphology depends on the presence and severity of bleeding.
- The white cell count remains slightly elevated.
- Bonemarrow biopsy is a definitive test of diagnosis. The bone marrow is usually hypercellular though it can be normocellular. The megakaryocytes are bigger in size and have hyperlobated nuclei which is the characteristic feature of increased thrombopoiesis. Cells are usually stainable with iron provided the patient had no significant hemorrhagic events. Collagen fibrosis is typically absent.[1]
-
![This represents a platelet count between 1.5 and 2 million per microliter (normal range is between 0.150 and 0.450 million). The patient had had an elevated count for at least 15 years but is asymptomatic.[6]](/images/0/0c/Essential_Thrombocythemia%2C_Peripheral_Blood.jpg)
This represents a platelet count between 1.5 and 2 million per microliter (normal range is between 0.150 and 0.450 million). The patient had had an elevated count for at least 15 years but is asymptomatic.[6]
-
![Histopathological image representing a bone marrow aspirate in a patient with essential thrombocythemia. Hematoxylin & eosin stain.[7]](/images/3/31/Bone_marrow_biopsy_ET.jpg)
Histopathological image representing a bone marrow aspirate in a patient with essential thrombocythemia. Hematoxylin & eosin stain.[7]
![This represents a platelet count between 1.5 and 2 million per microliter (normal range is between 0.150 and 0.450 million). The patient had had an elevated count for at least 15 years but is asymptomatic.[6]](/index.php/File:Essential_Thrombocythemia,_Peripheral_Blood.jpg)
![Histopathological image representing a bone marrow aspirate in a patient with essential thrombocythemia. Hematoxylin & eosin stain.[7]](/index.php/File:Bone_marrow_biopsy_ET.jpg)
References
- ↑ 1.0 1.1 1.2 Sanchez S, Ewton A (2006). "Essential thrombocythemia: a review of diagnostic and pathologic features". Arch Pathol Lab Med. 130 (8): 1144–50. doi:10.1043/1543-2165(2006)130[1144:ET]2.0.CO;2. PMID 16879015 PMID: 16879015 Check
|pmid=value (help). - ↑ Thrombopoietin. Wikipedia. https://en.wikipedia.org/wiki/Thrombopoietin#Function_and_regulation. Accessed on Novenber 3rd,2015.
- ↑ Platelet. Wikipedia.https://en.wikipedia.org/wiki/Platelet#Granule_secretion. Accessed on Novenber 3rd,2015.
- ↑ Jones AV, Kreil S, Zoi K, Waghorn K, Curtis C, Zhang L; et al. (2005). "Widespread occurrence of the JAK2 V617F mutation in chronic myeloproliferative disorders". Blood. 106 (6): 2162–8. doi:10.1182/blood-2005-03-1320. PMID 15920007.
- ↑ Rotunno, G.; Mannarelli, C.; Guglielmelli, P.; Pacilli, A.; Pancrazzi, A.; Pieri, L.; Fanelli, T.; Bosi, A.; Vannucchi, A. M. (2013). "Impact of calreticulin mutations on clinical and hematological phenotype and outcome in essential thrombocythemia". Blood. 123 (10): 1552–1555. doi:10.1182/blood-2013-11-538983. ISSN 0006-4971.
- ↑ File:Essential Thrombocythemia, Peripheral Blood (10189570483).jpg. Wikimedia Commons. https://commons.wikimedia.org/wiki/File:Essential_Thrombocythemia,_Peripheral_Blood_(10189570483).jpg Accessed on November 12, 2015.
- ↑ File:Essential thrombocythemia (1).jpg. Wikimedia commons. https://commons.wikimedia.org/wiki/File:Essential_thrombocythemia_(1).jpg Accessed on November 12, 2015.
.jpg){kind=link}
.jpg){kind=link}