Elastofibroma: Difference between revisions
No edit summary |
No edit summary |
||
| (39 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
__NOTOC__ | __NOTOC__ | ||
{{SI}} | {{SI}} | ||
Elastofibroma dorsi {{CMG}}; {{AE}}{{ADS}}{{MA}}{{Ammu}} | |||
Elastofibroma dorsi {{CMG}}; {{AE}} | |||
{{SK}}elastofibroma dorsi | {{SK}}elastofibroma dorsi | ||
==Overview== | ==Overview== | ||
Elastofibroma dorsi is a rare, slow growing, ill-defined [[soft tissue]] [[mass]] of the [[chest wall]]. It occurs most in the periscapular region.Elastofibroma was first discovered by Jarvi and Saxen, in 1961. Elastofibroma dorsi is a rare, slow growing, ill-defined [[soft tissue]] [[mass]] of the [[chest wall]]. It occurs most in the periscapular region. It is commonly located beneath [[latissimus dorsi]] and [[Rhomboid major muscle|rhomboid major muscles]] near to the [[Inferior angle of the scapula|inferior angle of the scapula.]] It is a benign [[neoplasm]] with clinical appearance of a [[malignant tumor]]. The exact pathogenesis of elastofibroma dorsi is not fully understood. It is thought that elastofibroma dorsi is the result of subclinical microtrauma, reactive [[hyperplasia]] of [[elastic fibers]] and increased production of [[fibrous tissue]]. The area between [[thoracic wall]] and [[scapula]] is the area of maximum and repeated friction and it was postulated as one of the reason of pathogenesis of elastofibroma. Elastofibroma often has bilateral location in the [[thoracic wall]]. On gross pathology, characteristic findings of elastofibroma include [[solitary]], poorly circumscribed, [[heterogeneous]], [[Soft tissue|soft-tissue]] mass. On microscopic [[histopathological]] analysis, characteristic findings of Elastofibroma include [[Eosinophilic]], beaded [[elastic fibers]] with Verhoeff's elastic stain. many fragmented fibers with appearance of beads on a string can be seen also. Elastofibroma dorsi must be differentiated from [[lipoma]], desmoid tumours, [[neurofibroma]] and [[liposarcoma]]. The [[prevalence]] of elastofibroma is approximately 11200 in men and 24400 in women per 100,000 individuals in each gender autopsies. Elastofibroma commonly affects elderly female and age can be ranging from 35-94 years. The female to male ratio is approximately 2.1. The majority of elastofibroma cases are reported in Japan. The majority of patients with elastofibroma dorsi are asymptomatic. Elastofibroma may present with painless [[swelling]], pain (less than 10% of patients), scapular snapping, limitation of motion, clunking sensation in the shoulder [[adduction]]-[[abduction]] movement. Patients with elastofibroma usually appear normal and physical examination findings of Elastofibroma can include limited [[range of motion]] and [[swelling]]. An x-ray may be helpful in the diagnosis of elastofibroma and the findings include soft tissue density in the periscapular region. X-ray may be normal. CT scan may show a heterogenous [[soft tissue]] mass with poorly defined margins.Magnetic resonance imaging is the first diagnostic tool for diagnosis of elastofibroma dorsi. Findings on MRI suggestive of elastofibroma include solitary heterogeneous, poorly circumscribed, [[soft-tissue]] mass which is isointense to muscle in T1 and T2WI images.Positron emission tomography/computed tomography (PET/CT) may show low to moderate metabolic activity in these patients. PET/CT shows low-grade diffuse 18F [[fluorodeoxyglucose]] uptake. Needle aspiration biopsy confirms the diagnosis exclude [[sarcoma]]. Surgical resection is considered only in symptomatic cases. | |||
==Historical Perspective== | ==Historical Perspective== | ||
Elastofibroma was first discovered by Jarvi and Saxen, in 1961.<ref name="pmid13789598">{{cite journal |vauthors=JARVI O, SAXEN E |title=Elastofibroma dorse |journal=Acta Pathol Microbiol Scand Suppl |volume=51(Suppl 144) |issue= |pages=83–4 |date=1961 |pmid=13789598 |doi= |url=}}</ref> | Elastofibroma was first discovered by Jarvi and Saxen, in 1961.<ref name="pmid13789598">{{cite journal |vauthors=JARVI O, SAXEN E |title=Elastofibroma dorse |journal=Acta Pathol Microbiol Scand Suppl |volume=51(Suppl 144) |issue= |pages=83–4 |date=1961 |pmid=13789598 |doi= |url=}}</ref><ref name="pmid11246542">{{cite journal| author=Järvi OH, Länsimies PH| title=Subclinical elastofibromas in the scapular region in an autopsy series. | journal=Acta Pathol Microbiol Scand A | year= 1975 | volume= 83 | issue= 1 | pages= 87-108 | pmid=1124654 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1124654 }}</ref> | ||
==Classification== | ==Classification== | ||
There is no established system for the classification of | There is no established system for the classification of elastofibroma. | ||
==Pathophysiology== | ==Pathophysiology== | ||
Elastofibroma dorsi is a rare, slow growing, ill-defined soft tissue mass of the chest wall. It occurs most in the periscapular region.It is commonly located beneath latissimus dorsi and rhomboid major muscles near to the inferior angle of the scapula. It is a benign neoplasm with clinical | *Elastofibroma dorsi is a rare, slow growing, ill-defined [[soft tissue]] [[mass]] of the [[chest wall]]. It occurs most in the periscapular region. | ||
*It is commonly located beneath [[latissimus dorsi]] and [[Rhomboid major muscle|rhomboid major muscles]] near to the [[Inferior angle of the scapula|inferior angle of the scapula.]] | |||
*It is a benign [[neoplasm]] with clinical appearance of a [[malignant tumor]].<ref name="pmid18407963">{{cite journal |vauthors=Freixinet J, Rodríguez P, Hussein M, Sanromán B, Herrero J, Gil R |title=Elastofibroma of the thoracic wall |journal=Interact Cardiovasc Thorac Surg |volume=7 |issue=4 |pages=626–8 |date=August 2008 |pmid=18407963 |doi=10.1510/icvts.2007.174722 |url=}}</ref> | |||
*The exact pathogenesis of elastofibroma dorsi is not fully understood. | |||
*It is thought that elastofibroma dorsi is the result of subclinical microtrauma, reactive [[hyperplasia]] of [[elastic fibers]] and increased production of [[fibrous tissue]].<ref name="pmid1417241">{{cite journal |vauthors=Machens HG, Mechtersheimer R, Göhring U, Schlag PN |title=Bilateral elastofibroma dorsi |journal=Ann. Thorac. Surg. |volume=54 |issue=4 |pages=774–6 |date=October 1992 |pmid=1417241 |doi= |url=}}</ref><ref name="pmid169615222">{{cite journal| author=Cota C, Solivetti F, Kovacs D, Cristiani R, Amantea A| title=Elastofibroma dorsi: histologic and echographic considerations. | journal=Int J Dermatol | year= 2006 | volume= 45 | issue= 9 | pages= 1100-3 | pmid=16961522 | doi=10.1111/j.1365-4632.2004.02550.x | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16961522 }}</ref> | |||
*The area between [[thoracic wall]] and [[scapula]] is the area of maximum and repeated friction and it was postulated as one of the reason of pathogenesis of elastofibroma.<ref name="pmid169615222" /> | |||
*Another theory regarding pathogenesis includes genetic alteration using [[comparative genomic hybridization]](CGH). | |||
*Hernandez ''et al'' found changes in [[DNA sequences|DNA-sequences]] in [[chromosomes]] 1p, 13q, 19p and 22q.<ref name="pmid20422214">{{cite journal| author=Hernández JL, Rodríguez-Parets JO, Valero JM, Muñoz MA, Benito MR, Hernandez JM et al.| title=High-resolution genome-wide analysis of chromosomal alterations in elastofibroma. | journal=Virchows Arch | year= 2010 | volume= 456 | issue= 6 | pages= 681-7 | pmid=20422214 | doi=10.1007/s00428-010-0911-y | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=20422214 }}</ref> | |||
*Nishio ''et al.'' noted an increase of [[DNA]] copies on [[X chromosome]]<nowiki/>s ' long arm using CGH.<ref name="pmid12165800">{{cite journal| author=Nishio JN, Iwasaki H, Ohjimi Y, Ishiguro M, Koga T, Isayama T et al.| title=Gain of Xq detected by comparative genomic hybridization in elastofibroma. | journal=Int J Mol Med | year= 2002 | volume= 10 | issue= 3 | pages= 277-80 | pmid=12165800 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12165800 }}</ref> | |||
*Elastofibroma often has bilateral location in the [[thoracic wall]].<ref name="JenaPatnayak20163">{{cite journal|last1=Jena|first1=Amitabh|last2=Patnayak|first2=Rashmi|last3=Settipalli|first3=Sarla|last4=Nagesh|first4=N|title=Elastofibroma: An uncommon tumor revisited|journal=Journal of Cutaneous and Aesthetic Surgery|volume=9|issue=1|year=2016|pages=34|issn=0974-2077|doi=10.4103/0974-2077.178543}}</ref><ref name="SariciBasbay2014">{{cite journal|last1=Sarici|first1=Inanc Samil|last2=Basbay|first2=Elif|last3=Mustu|first3=Mehdi|last4=Eskut|first4=Burak|last5=Kala|first5=Ferhat|last6=Agcaoglu|first6=Orhan|last7=Akici|first7=Murat|last8=Ozkurt|first8=Enver|title=Bilateral elastofibroma dorsi: A case report|journal=International Journal of Surgery Case Reports|volume=5|issue=12|year=2014|pages=1139–1141|issn=22102612|doi=10.1016/j.ijscr.2014.10.032}}</ref> | |||
===Gross pathology=== | |||
On gross pathology, characteristic findings of elastofibroma include:<ref name="JenaPatnayak20163" /> | |||
* A [[solitary]], poorly circumscribed, [[heterogeneous]], [[Soft tissue|soft-tissue]] mass. | |||
*Cut section are firm with grayish-white areas. | |||
===Microscopic findings=== | |||
On microscopic [[histopathological]] analysis, characteristic findings of Elastofibroma include:<ref name="JenaPatnayak20163" /><ref name="pmid16961522">{{cite journal| author=Cota C, Solivetti F, Kovacs D, Cristiani R, Amantea A| title=Elastofibroma dorsi: histologic and echographic considerations. | journal=Int J Dermatol | year= 2006 | volume= 45 | issue= 9 | pages= 1100-3 | pmid=16961522 | doi=10.1111/j.1365-4632.2004.02550.x | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=16961522 }}</ref> | |||
[ | |||
*Cut section are firm with grayish-white areas | |||
On microscopic histopathological analysis, characteristic findings of Elastofibroma include: <ref name=" | |||
*[[Eosinophilic]], beaded [[elastic fibers]] with Verhoeff's elastic stain. | |||
*Many fragmented fibers with appearance of beads on a string. | |||
===Gallery=== | |||
<gallery heights="175" widths="175"> | |||
File:1-s2.0-S2210261214002806-gr2 lrg.jpg| Bilateral Elastofibroma dorsi. Source:''Science direct(under creative commons)''<ref name="SariciBasbay2014">{{cite journal|last1=Sarici|first1=Inanc Samil|last2=Basbay|first2=Elif|last3=Mustu|first3=Mehdi|last4=Eskut|first4=Burak|last5=Kala|first5=Ferhat|last6=Agcaoglu|first6=Orhan|last7=Akici|first7=Murat|last8=Ozkurt|first8=Enver|title=Bilateral elastofibroma dorsi: A case report|journal=International Journal of Surgery Case Reports|volume=5|issue=12|year=2014|pages=1139–1141|issn=22102612|doi=10.1016/j.ijscr.2014.10.032}}</ref> | |||
Image:Elastofibroma of mitral valve 001.jpg|Elastofibroma | |||
File:1-s2.0-S2210261214002806-gr3 lrg.jpg| Bilateral Elastofibroma dorsi. Source:''Science direct(under creative commons)''<ref name="SariciBasbay2014">{{cite journal|last1=Sarici|first1=Inanc Samil|last2=Basbay|first2=Elif|last3=Mustu|first3=Mehdi|last4=Eskut|first4=Burak|last5=Kala|first5=Ferhat|last6=Agcaoglu|first6=Orhan|last7=Akici|first7=Murat|last8=Ozkurt|first8=Enver|title=Bilateral elastofibroma dorsi: A case report|journal=International Journal of Surgery Case Reports|volume=5|issue=12|year=2014|pages=1139–1141|issn=22102612|doi=10.1016/j.ijscr.2014.10.032}}</ref> | |||
Image:Papillary fibroelastoma 001.jpg|Papillary Fibroelastoma: When located on the mitral valve, these tumors are usually on the anterior leaflet of the atrial surface. | |||
</gallery> | |||
==Causes== | ==Causes== | ||
The cause of elastofibroma dorsi has not been identified. Subclinical microtrauma could be one of the reasons.<ref name="pmid1417241" /> | |||
<br /> | |||
The cause of elastofibroma dorsi has not been identified. Subclinical microtrauma could be one of the reasons. <ref name="pmid1417241" /> | |||
==Differentiating Elastofibroma dorsi from Other Diseases== | ==Differentiating Elastofibroma dorsi from Other Diseases== | ||
Elastofibroma dorsi must be differentiated from desmoid tumours, neurofibroma and liposarcoma. <ref name=" | Elastofibroma dorsi must be differentiated from desmoid tumours, neurofibroma and liposarcoma.<ref name="JenaPatnayak20163" /> | ||
==Epidemiology and Demographics== | ==Epidemiology and Demographics== | ||
The prevalence of elastofibroma is approximately 11200 in men and 24400 in women per 100,000 individuals in each gender autopsies. <ref name=" | *The prevalence of elastofibroma is approximately 11200 in men and 24400 in women per 100,000 individuals in each gender autopsies.<ref name="JenaPatnayak20163" /> | ||
*Elastofibroma commonly affects elderly female.<ref name="JenaPatnayak20163" /> | |||
*Elastofibroma commonly affects females ranging from 35-94 years.<ref name="JenaPatnayak20163" /> | |||
*Females are more commonly affected by elastofibroma than men. The female to male ratio is approximately 2.1 | |||
*The majority of elastofibroma cases are reported in Japan.<ref name="JenaPatnayak20163" /> | |||
Elastofibroma commonly affects elderly female. <ref name=" | |||
Elastofibroma commonly affects females ranging from 35-94 years. <ref name=" | |||
The majority of elastofibroma cases are reported in Japan. <ref name=" | |||
==Risk Factors== | ==Risk Factors== | ||
There are no established risk factors for | There are no established risk factors for elastofibroma. | ||
==Screening== | ==Screening== | ||
There is insufficient evidence to recommend routine screening for | There is insufficient evidence to recommend routine screening for elastofibroma. | ||
==Natural History, Complications, and Prognosis== | ==Natural History, Complications, and Prognosis== | ||
Prognosis is generally excellent. | |||
Prognosis is generally excellent | |||
==Diagnosis== | ==Diagnosis== | ||
===Diagnostic Study of Choice=== | ===Diagnostic Study of Choice=== | ||
There are no established criteria for the diagnosis of elastofibroma. | |||
There are no established criteria for the diagnosis of | |||
===History and Symptoms=== | ===History and Symptoms=== | ||
The majority of patients with elastofibroma dorsi are asymptomatic. Elastofibroma may present with:<ref name="pmid2652048">{{cite journal |vauthors=Greenberg JA, Lockwood RC |title=Elastofibroma dorsi. A case report and review of the literature |journal=Orthop Rev |volume=18 |issue=3 |pages=329–33 |date=March 1989 |pmid=2652048 |doi= |url=}}</ref> | The majority of patients with elastofibroma dorsi are asymptomatic. Elastofibroma may present with:<ref name="pmid2652048">{{cite journal |vauthors=Greenberg JA, Lockwood RC |title=Elastofibroma dorsi. A case report and review of the literature |journal=Orthop Rev |volume=18 |issue=3 |pages=329–33 |date=March 1989 |pmid=2652048 |doi= |url=}}</ref> | ||
* Painless swelling | * Painless [[swelling]] | ||
* Pain ( less than 10% of patients) | * Pain (less than 10% of patients) | ||
* Scapular snapping | * Scapular snapping | ||
* Limitation of motion, | * Limitation of motion, | ||
* Clunking sensation in the shoulder adduction-abduction movement<ref name="pmid25437657">{{cite journal |vauthors=Sarici IS, Basbay E, Mustu M, Eskut B, Kala F, Agcaoglu O, Akici M, Ozkurt E |title=Bilateral elastofibroma dorsi: A case report |journal=Int J Surg Case Rep |volume=5 |issue=12 |pages=1139–41 |date=2014 |pmid=25437657 |pmc=4275815 |doi=10.1016/j.ijscr.2014.10.032 |url=}}</ref> | * Clunking sensation in the shoulder [[adduction]]-[[abduction]] movement<ref name="pmid25437657">{{cite journal |vauthors=Sarici IS, Basbay E, Mustu M, Eskut B, Kala F, Agcaoglu O, Akici M, Ozkurt E |title=Bilateral elastofibroma dorsi: A case report |journal=Int J Surg Case Rep |volume=5 |issue=12 |pages=1139–41 |date=2014 |pmid=25437657 |pmc=4275815 |doi=10.1016/j.ijscr.2014.10.032 |url=}}</ref> | ||
===Physical Examination=== | ===Physical Examination=== | ||
Patients with | *Patients with elastofibroma usually appear normal. | ||
*Physical examination findings of Elastofibroma can include limited [[range of motion]] and [[swelling]] <ref name="pmid25437657">{{cite journal |vauthors=Sarici IS, Basbay E, Mustu M, Eskut B, Kala F, Agcaoglu O, Akici M, Ozkurt E |title=Bilateral elastofibroma dorsi: A case report |journal=Int J Surg Case Rep |volume=5 |issue=12 |pages=1139–41 |date=2014 |pmid=25437657 |pmc=4275815 |doi=10.1016/j.ijscr.2014.10.032 |url=}}</ref> | |||
===Laboratory Findings=== | ===Laboratory Findings=== | ||
There are no diagnostic laboratory findings associated with elastofibroma. | |||
There are no diagnostic laboratory findings associated with | |||
===Electrocardiogram=== | ===Electrocardiogram=== | ||
There are no ECG findings associated with | There are no ECG findings associated with elastofibroma. | ||
===X-ray=== | ===X-ray=== | ||
An x-ray may be helpful in the diagnosis of elastofibroma. Findings on an x-ray suggestive of elastofibroma include soft tissue density in the periscapular region. X-ray may be normal.<ref name="pmid18551204">{{cite journal |vauthors=Tetikkurt C, Tetikkurt S, Bayar N |title=Diagnosis of elastofibroma |journal=Can. Respir. J. |volume=15 |issue=4 |pages=217–8 |date=2008 |pmid=18551204 |pmc=2677955 |doi=10.1155/2008/638624 |url=}}</ref> | |||
An x-ray may be helpful in the diagnosis of elastofibroma. Findings on an x-ray suggestive of elastofibroma include soft tissue density in the periscapular region. X-ray may be normal. <ref name="pmid18551204">{{cite journal |vauthors=Tetikkurt C, Tetikkurt S, Bayar N |title=Diagnosis of elastofibroma |journal=Can. Respir. J. |volume=15 |issue=4 |pages=217–8 |date=2008 |pmid=18551204 |pmc=2677955 |doi=10.1155/2008/638624 |url=}}</ref> | |||
===Echocardiography or Ultrasound=== | ===Echocardiography or Ultrasound=== | ||
There are no echocardiography/ultrasound | There are no echocardiography/ultrasound findings associated with elastofibroma. | ||
===CT scan=== | ===CT scan=== | ||
CT scan may be helpful in the diagnosis of elastofibroma dorsi. Findings on CT scan suggestive of elastofibroma dorsi include a heterogenous soft tissue mass with poorly defined margins. <ref name="pmid8998883">{{cite journal |vauthors=Hoffman JK, Klein MH, McInerney VK |title=Bilateral elastofibroma: a case report and review of the literature |journal=Clin. Orthop. Relat. Res. |volume= |issue=325 |pages=245–50 |date=April 1996 |pmid=8998883 |doi= |url=}}</ref> | CT scan may be helpful in the diagnosis of elastofibroma dorsi. Findings on CT scan suggestive of elastofibroma dorsi include a heterogenous [[soft tissue]] mass with poorly defined margins.<ref name="pmid8998883">{{cite journal |vauthors=Hoffman JK, Klein MH, McInerney VK |title=Bilateral elastofibroma: a case report and review of the literature |journal=Clin. Orthop. Relat. Res. |volume= |issue=325 |pages=245–50 |date=April 1996 |pmid=8998883 |doi= |url=}}</ref><ref name="pmid1503030">{{cite journal| author=Kransdorf MJ, Meis JM, Montgomery E| title=Elastofibroma: MR and CT appearance with radiologic-pathologic correlation. | journal=AJR Am J Roentgenol | year= 1992 | volume= 159 | issue= 3 | pages= 575-9 | pmid=1503030 | doi=10.2214/ajr.159.3.1503030 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1503030 }}</ref> | ||
===MRI=== | ===MRI=== | ||
Magnetic resonance imaging is the most useful diagnostic tool for diagnosis of elastofibroma dorsi. <ref name="pmid14648789">{{cite journal |vauthors=Domanski HA, Carlén B, Sloth M, Rydholm A |title=Elastofibroma dorsi has distinct cytomorphologic features, making diagnostic surgical biopsy unnecessary: cytomorphologic study with clinical, radiologic, and electron microscopic correlations |journal=Diagn. Cytopathol. |volume=29 |issue=6 |pages=327–33 |date=December 2003 |pmid=14648789 |doi=10.1002/dc.10381 |url=}}</ref> | *Magnetic resonance imaging is the most useful diagnostic tool for diagnosis of elastofibroma dorsi.<ref name="pmid15030302">{{cite journal| author=Kransdorf MJ, Meis JM, Montgomery E| title=Elastofibroma: MR and CT appearance with radiologic-pathologic correlation. | journal=AJR Am J Roentgenol | year= 1992 | volume= 159 | issue= 3 | pages= 575-9 | pmid=1503030 | doi=10.2214/ajr.159.3.1503030 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1503030 }}</ref><ref name="pmid14648789">{{cite journal |vauthors=Domanski HA, Carlén B, Sloth M, Rydholm A |title=Elastofibroma dorsi has distinct cytomorphologic features, making diagnostic surgical biopsy unnecessary: cytomorphologic study with clinical, radiologic, and electron microscopic correlations |journal=Diagn. Cytopathol. |volume=29 |issue=6 |pages=327–33 |date=December 2003 |pmid=14648789 |doi=10.1002/dc.10381 |url=}}</ref> | ||
*Findings on MRI suggestive of elastofibroma include solitary heterogeneous, poorly circumscribed, [[soft-tissue]] mass.<ref name="pmid15030303">{{cite journal| author=Kransdorf MJ, Meis JM, Montgomery E| title=Elastofibroma: MR and CT appearance with radiologic-pathologic correlation. | journal=AJR Am J Roentgenol | year= 1992 | volume= 159 | issue= 3 | pages= 575-9 | pmid=1503030 | doi=10.2214/ajr.159.3.1503030 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1503030 }}</ref><ref name="pmid21655005">{{cite journal |vauthors=Go PH, Meadows MC, Deleon EM, Chamberlain RS |title=Elastofibroma dorsi: A soft tissue masquerade |journal=Int J Shoulder Surg |volume=4 |issue=4 |pages=97–101 |date=October 2010 |pmid=21655005 |pmc=3100815 |doi=10.4103/0973-6042.79797 |url=}}</ref> | |||
Findings on MRI suggestive of elastofibroma include solitary heterogeneous, poorly circumscribed, soft-tissue mass.<ref name="pmid21655005">{{cite journal |vauthors=Go PH, Meadows MC, Deleon EM, Chamberlain RS |title=Elastofibroma dorsi: A soft tissue masquerade |journal=Int J Shoulder Surg |volume=4 |issue=4 |pages=97–101 |date=October 2010 |pmid=21655005 |pmc=3100815 |doi=10.4103/0973-6042.79797 |url=}}</ref> | *The lesion is isointense to muscle in T1 and T2WI images | ||
The lesion is isointense to muscle in T1 and T2WI images | |||
===Other Imaging Findings=== | ===Other Imaging Findings=== | ||
Positron emission tomography/computed tomography (PET/CT) may be helpful in the diagnosis of elastofibroma. Findings on PET/CT suggestive of elastofibroma include low to moderate metabolic activity in these patients. PET/CT shows low-grade diffuse 18F [[fluorodeoxyglucose]] uptake.<ref name="pmid16100483">{{cite journal |vauthors=Patrikeos A, Breidahl W, Robins P |title=F-18 FDG uptake associated with Elastofibroma dorsi |journal=Clin Nucl Med |volume=30 |issue=9 |pages=617–8 |date=September 2005 |pmid=16100483 |doi= |url=}}</ref> | |||
Positron emission tomography/computed tomography (PET/CT) may be helpful in the diagnosis of elastofibroma. Findings on PET/CT suggestive of elastofibroma include low to moderate metabolic activity in these patients. PET/CT shows low-grade diffuse 18F fluorodeoxyglucose uptake. <ref name="pmid16100483">{{cite journal |vauthors=Patrikeos A, Breidahl W, Robins P |title=F-18 FDG uptake associated with Elastofibroma dorsi |journal=Clin Nucl Med |volume=30 |issue=9 |pages=617–8 |date=September 2005 |pmid=16100483 |doi= |url=}}</ref> | |||
===Other Diagnostic Studies=== | ===Other Diagnostic Studies=== | ||
Needle aspiration biopsy is helpful in the diagnosis of elastofibroma and exclude [[sarcoma]].<ref name="pmid18551204">{{cite journal |vauthors=Tetikkurt C, Tetikkurt S, Bayar N |title=Diagnosis of elastofibroma |journal=Can. Respir. J. |volume=15 |issue=4 |pages=217–8 |date=2008 |pmid=18551204 |pmc=2677955 |doi=10.1155/2008/638624 |url=}}</ref> | |||
Needle aspiration biopsy is helpful in the diagnosis of elastofibroma and exclude | |||
==Treatment== | ==Treatment== | ||
===Surgery=== | ===Surgery=== | ||
Surgical resection is considered only in symptomatic cases. <ref name=" | Surgical resection is considered only in symptomatic cases.<ref name="JenaPatnayak20163" /> | ||
===Primary Prevention=== | ===Primary Prevention=== | ||
There are no established measures for the primary prevention of | There are no established measures for the primary prevention of elastofibroma. | ||
===Secondary Prevention=== | ===Secondary Prevention=== | ||
There are no established measures for the secondary prevention of | There are no established measures for the secondary prevention of elastofibroma. | ||
==References== | ==References== | ||
| Line 402: | Line 124: | ||
{{WikiDoc Help Menu}} | {{WikiDoc Help Menu}} | ||
{{WikiDoc Sources}} | {{WikiDoc Sources}} | ||
[[Category:Oncology]] | [[Category:Oncology]] | ||
[[Category:Up-To-Date]] | |||
[[Category:Oncology]] | [[Category:Oncology]] | ||
[[Category:Medicine]] | [[Category:Medicine]] | ||
Latest revision as of 20:59, 3 October 2019
|
WikiDoc Resources for Elastofibroma |
|
Articles |
|---|
|
Most recent articles on Elastofibroma Most cited articles on Elastofibroma |
|
Media |
|
Powerpoint slides on Elastofibroma |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Elastofibroma at Clinical Trials.gov Trial results on Elastofibroma Clinical Trials on Elastofibroma at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Elastofibroma NICE Guidance on Elastofibroma
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Elastofibroma Discussion groups on Elastofibroma Patient Handouts on Elastofibroma Directions to Hospitals Treating Elastofibroma Risk calculators and risk factors for Elastofibroma
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Elastofibroma |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Elastofibroma dorsi Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Amandeep Singh M.D.[2]Mahda Alihashemi M.D. [3]Ammu Susheela, M.D. [4] Synonyms and keywords:elastofibroma dorsi
Overview
Elastofibroma dorsi is a rare, slow growing, ill-defined soft tissue mass of the chest wall. It occurs most in the periscapular region.Elastofibroma was first discovered by Jarvi and Saxen, in 1961. Elastofibroma dorsi is a rare, slow growing, ill-defined soft tissue mass of the chest wall. It occurs most in the periscapular region. It is commonly located beneath latissimus dorsi and rhomboid major muscles near to the inferior angle of the scapula. It is a benign neoplasm with clinical appearance of a malignant tumor. The exact pathogenesis of elastofibroma dorsi is not fully understood. It is thought that elastofibroma dorsi is the result of subclinical microtrauma, reactive hyperplasia of elastic fibers and increased production of fibrous tissue. The area between thoracic wall and scapula is the area of maximum and repeated friction and it was postulated as one of the reason of pathogenesis of elastofibroma. Elastofibroma often has bilateral location in the thoracic wall. On gross pathology, characteristic findings of elastofibroma include solitary, poorly circumscribed, heterogeneous, soft-tissue mass. On microscopic histopathological analysis, characteristic findings of Elastofibroma include Eosinophilic, beaded elastic fibers with Verhoeff's elastic stain. many fragmented fibers with appearance of beads on a string can be seen also. Elastofibroma dorsi must be differentiated from lipoma, desmoid tumours, neurofibroma and liposarcoma. The prevalence of elastofibroma is approximately 11200 in men and 24400 in women per 100,000 individuals in each gender autopsies. Elastofibroma commonly affects elderly female and age can be ranging from 35-94 years. The female to male ratio is approximately 2.1. The majority of elastofibroma cases are reported in Japan. The majority of patients with elastofibroma dorsi are asymptomatic. Elastofibroma may present with painless swelling, pain (less than 10% of patients), scapular snapping, limitation of motion, clunking sensation in the shoulder adduction-abduction movement. Patients with elastofibroma usually appear normal and physical examination findings of Elastofibroma can include limited range of motion and swelling. An x-ray may be helpful in the diagnosis of elastofibroma and the findings include soft tissue density in the periscapular region. X-ray may be normal. CT scan may show a heterogenous soft tissue mass with poorly defined margins.Magnetic resonance imaging is the first diagnostic tool for diagnosis of elastofibroma dorsi. Findings on MRI suggestive of elastofibroma include solitary heterogeneous, poorly circumscribed, soft-tissue mass which is isointense to muscle in T1 and T2WI images.Positron emission tomography/computed tomography (PET/CT) may show low to moderate metabolic activity in these patients. PET/CT shows low-grade diffuse 18F fluorodeoxyglucose uptake. Needle aspiration biopsy confirms the diagnosis exclude sarcoma. Surgical resection is considered only in symptomatic cases.
Historical Perspective
Elastofibroma was first discovered by Jarvi and Saxen, in 1961.[1][2]
Classification
There is no established system for the classification of elastofibroma.
Pathophysiology
- Elastofibroma dorsi is a rare, slow growing, ill-defined soft tissue mass of the chest wall. It occurs most in the periscapular region.
- It is commonly located beneath latissimus dorsi and rhomboid major muscles near to the inferior angle of the scapula.
- It is a benign neoplasm with clinical appearance of a malignant tumor.[3]
- The exact pathogenesis of elastofibroma dorsi is not fully understood.
- It is thought that elastofibroma dorsi is the result of subclinical microtrauma, reactive hyperplasia of elastic fibers and increased production of fibrous tissue.[4][5]
- The area between thoracic wall and scapula is the area of maximum and repeated friction and it was postulated as one of the reason of pathogenesis of elastofibroma.[5]
- Another theory regarding pathogenesis includes genetic alteration using comparative genomic hybridization(CGH).
- Hernandez et al found changes in DNA-sequences in chromosomes 1p, 13q, 19p and 22q.[6]
- Nishio et al. noted an increase of DNA copies on X chromosomes ' long arm using CGH.[7]
- Elastofibroma often has bilateral location in the thoracic wall.[8][9]
Gross pathology
On gross pathology, characteristic findings of elastofibroma include:[8]
- A solitary, poorly circumscribed, heterogeneous, soft-tissue mass.
- Cut section are firm with grayish-white areas.
Microscopic findings
On microscopic histopathological analysis, characteristic findings of Elastofibroma include:[8][10]
- Eosinophilic, beaded elastic fibers with Verhoeff's elastic stain.
- Many fragmented fibers with appearance of beads on a string.
Gallery
-
![Bilateral Elastofibroma dorsi. Source:Science direct(under creative commons)[9]](/images/1/19/1-s2.0-S2210261214002806-gr2_lrg.jpg)
Bilateral Elastofibroma dorsi. Source:Science direct(under creative commons)[9]
-
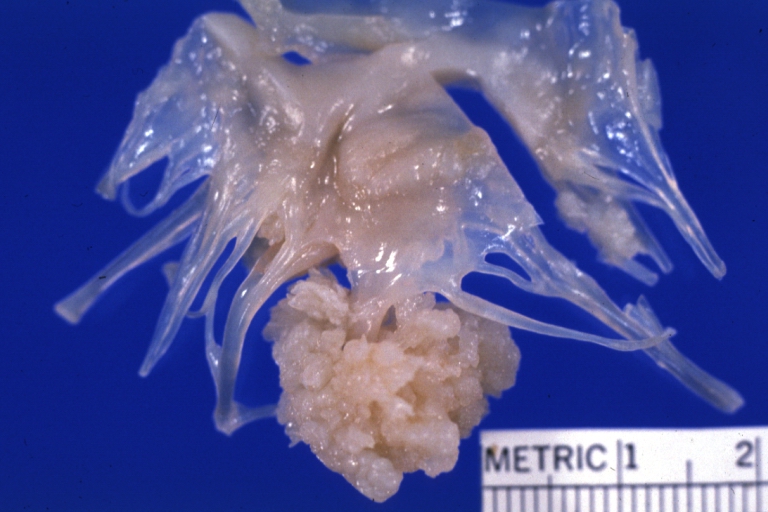
Elastofibroma
-
![Bilateral Elastofibroma dorsi. Source:Science direct(under creative commons)[9]](/images/4/4e/1-s2.0-S2210261214002806-gr3_lrg.jpg)
Bilateral Elastofibroma dorsi. Source:Science direct(under creative commons)[9]
-
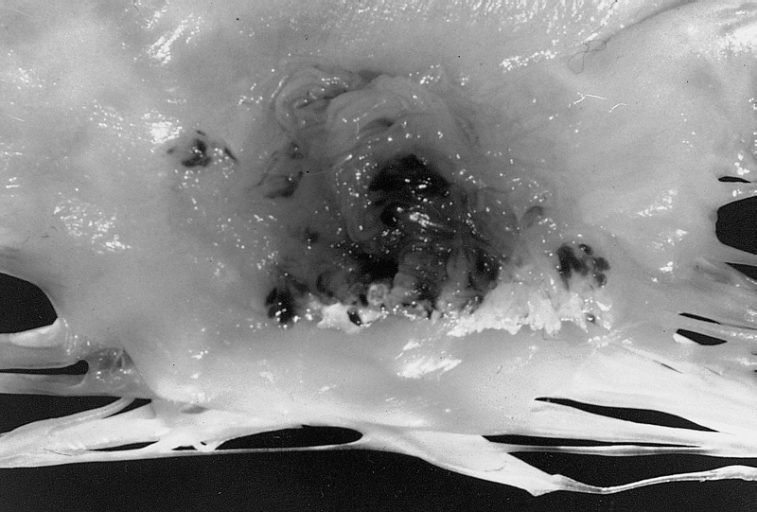
Papillary Fibroelastoma: When located on the mitral valve, these tumors are usually on the anterior leaflet of the atrial surface.
![Bilateral Elastofibroma dorsi. Source:Science direct(under creative commons)[9]](/index.php/File:1-s2.0-S2210261214002806-gr2_lrg.jpg)

![Bilateral Elastofibroma dorsi. Source:Science direct(under creative commons)[9]](/index.php/File:1-s2.0-S2210261214002806-gr3_lrg.jpg)

Causes
The cause of elastofibroma dorsi has not been identified. Subclinical microtrauma could be one of the reasons.[4]
Differentiating Elastofibroma dorsi from Other Diseases
Elastofibroma dorsi must be differentiated from desmoid tumours, neurofibroma and liposarcoma.[8]
Epidemiology and Demographics
- The prevalence of elastofibroma is approximately 11200 in men and 24400 in women per 100,000 individuals in each gender autopsies.[8]
- Elastofibroma commonly affects elderly female.[8]
- Elastofibroma commonly affects females ranging from 35-94 years.[8]
- Females are more commonly affected by elastofibroma than men. The female to male ratio is approximately 2.1
- The majority of elastofibroma cases are reported in Japan.[8]
Risk Factors
There are no established risk factors for elastofibroma.
Screening
There is insufficient evidence to recommend routine screening for elastofibroma.
Natural History, Complications, and Prognosis
Prognosis is generally excellent.
Diagnosis
Diagnostic Study of Choice
There are no established criteria for the diagnosis of elastofibroma.
History and Symptoms
The majority of patients with elastofibroma dorsi are asymptomatic. Elastofibroma may present with:[11]
- Painless swelling
- Pain (less than 10% of patients)
- Scapular snapping
- Limitation of motion,
- Clunking sensation in the shoulder adduction-abduction movement[12]
Physical Examination
- Patients with elastofibroma usually appear normal.
- Physical examination findings of Elastofibroma can include limited range of motion and swelling [12]
Laboratory Findings
There are no diagnostic laboratory findings associated with elastofibroma.
Electrocardiogram
There are no ECG findings associated with elastofibroma.
X-ray
An x-ray may be helpful in the diagnosis of elastofibroma. Findings on an x-ray suggestive of elastofibroma include soft tissue density in the periscapular region. X-ray may be normal.[13]
Echocardiography or Ultrasound
There are no echocardiography/ultrasound findings associated with elastofibroma.
CT scan
CT scan may be helpful in the diagnosis of elastofibroma dorsi. Findings on CT scan suggestive of elastofibroma dorsi include a heterogenous soft tissue mass with poorly defined margins.[14][15]
MRI
- Magnetic resonance imaging is the most useful diagnostic tool for diagnosis of elastofibroma dorsi.[16][17]
- Findings on MRI suggestive of elastofibroma include solitary heterogeneous, poorly circumscribed, soft-tissue mass.[18][19]
- The lesion is isointense to muscle in T1 and T2WI images
Other Imaging Findings
Positron emission tomography/computed tomography (PET/CT) may be helpful in the diagnosis of elastofibroma. Findings on PET/CT suggestive of elastofibroma include low to moderate metabolic activity in these patients. PET/CT shows low-grade diffuse 18F fluorodeoxyglucose uptake.[20]
Other Diagnostic Studies
Needle aspiration biopsy is helpful in the diagnosis of elastofibroma and exclude sarcoma.[13]
Treatment
Surgery
Surgical resection is considered only in symptomatic cases.[8]
Primary Prevention
There are no established measures for the primary prevention of elastofibroma.
Secondary Prevention
There are no established measures for the secondary prevention of elastofibroma.
References
- ↑ JARVI O, SAXEN E (1961). "Elastofibroma dorse". Acta Pathol Microbiol Scand Suppl. 51(Suppl 144): 83–4. PMID 13789598.
- ↑ Järvi OH, Länsimies PH (1975). "Subclinical elastofibromas in the scapular region in an autopsy series". Acta Pathol Microbiol Scand A. 83 (1): 87–108. PMID 1124654.
- ↑ Freixinet J, Rodríguez P, Hussein M, Sanromán B, Herrero J, Gil R (August 2008). "Elastofibroma of the thoracic wall". Interact Cardiovasc Thorac Surg. 7 (4): 626–8. doi:10.1510/icvts.2007.174722. PMID 18407963.
- ↑ 4.0 4.1 Machens HG, Mechtersheimer R, Göhring U, Schlag PN (October 1992). "Bilateral elastofibroma dorsi". Ann. Thorac. Surg. 54 (4): 774–6. PMID 1417241.
- ↑ 5.0 5.1 Cota C, Solivetti F, Kovacs D, Cristiani R, Amantea A (2006). "Elastofibroma dorsi: histologic and echographic considerations". Int J Dermatol. 45 (9): 1100–3. doi:10.1111/j.1365-4632.2004.02550.x. PMID 16961522.
- ↑ Hernández JL, Rodríguez-Parets JO, Valero JM, Muñoz MA, Benito MR, Hernandez JM; et al. (2010). "High-resolution genome-wide analysis of chromosomal alterations in elastofibroma". Virchows Arch. 456 (6): 681–7. doi:10.1007/s00428-010-0911-y. PMID 20422214.
- ↑ Nishio JN, Iwasaki H, Ohjimi Y, Ishiguro M, Koga T, Isayama T; et al. (2002). "Gain of Xq detected by comparative genomic hybridization in elastofibroma". Int J Mol Med. 10 (3): 277–80. PMID 12165800.
- ↑ 8.0 8.1 8.2 8.3 8.4 8.5 8.6 8.7 8.8 Jena, Amitabh; Patnayak, Rashmi; Settipalli, Sarla; Nagesh, N (2016). "Elastofibroma: An uncommon tumor revisited". Journal of Cutaneous and Aesthetic Surgery. 9 (1): 34. doi:10.4103/0974-2077.178543. ISSN 0974-2077.
- ↑ 9.0 9.1 9.2 Sarici, Inanc Samil; Basbay, Elif; Mustu, Mehdi; Eskut, Burak; Kala, Ferhat; Agcaoglu, Orhan; Akici, Murat; Ozkurt, Enver (2014). "Bilateral elastofibroma dorsi: A case report". International Journal of Surgery Case Reports. 5 (12): 1139–1141. doi:10.1016/j.ijscr.2014.10.032. ISSN 2210-2612.
- ↑ Cota C, Solivetti F, Kovacs D, Cristiani R, Amantea A (2006). "Elastofibroma dorsi: histologic and echographic considerations". Int J Dermatol. 45 (9): 1100–3. doi:10.1111/j.1365-4632.2004.02550.x. PMID 16961522.
- ↑ Greenberg JA, Lockwood RC (March 1989). "Elastofibroma dorsi. A case report and review of the literature". Orthop Rev. 18 (3): 329–33. PMID 2652048.
- ↑ 12.0 12.1 Sarici IS, Basbay E, Mustu M, Eskut B, Kala F, Agcaoglu O, Akici M, Ozkurt E (2014). "Bilateral elastofibroma dorsi: A case report". Int J Surg Case Rep. 5 (12): 1139–41. doi:10.1016/j.ijscr.2014.10.032. PMC 4275815. PMID 25437657.
- ↑ 13.0 13.1 Tetikkurt C, Tetikkurt S, Bayar N (2008). "Diagnosis of elastofibroma". Can. Respir. J. 15 (4): 217–8. doi:10.1155/2008/638624. PMC 2677955. PMID 18551204.
- ↑ Hoffman JK, Klein MH, McInerney VK (April 1996). "Bilateral elastofibroma: a case report and review of the literature". Clin. Orthop. Relat. Res. (325): 245–50. PMID 8998883.
- ↑ Kransdorf MJ, Meis JM, Montgomery E (1992). "Elastofibroma: MR and CT appearance with radiologic-pathologic correlation". AJR Am J Roentgenol. 159 (3): 575–9. doi:10.2214/ajr.159.3.1503030. PMID 1503030.
- ↑ Kransdorf MJ, Meis JM, Montgomery E (1992). "Elastofibroma: MR and CT appearance with radiologic-pathologic correlation". AJR Am J Roentgenol. 159 (3): 575–9. doi:10.2214/ajr.159.3.1503030. PMID 1503030.
- ↑ Domanski HA, Carlén B, Sloth M, Rydholm A (December 2003). "Elastofibroma dorsi has distinct cytomorphologic features, making diagnostic surgical biopsy unnecessary: cytomorphologic study with clinical, radiologic, and electron microscopic correlations". Diagn. Cytopathol. 29 (6): 327–33. doi:10.1002/dc.10381. PMID 14648789.
- ↑ Kransdorf MJ, Meis JM, Montgomery E (1992). "Elastofibroma: MR and CT appearance with radiologic-pathologic correlation". AJR Am J Roentgenol. 159 (3): 575–9. doi:10.2214/ajr.159.3.1503030. PMID 1503030.
- ↑ Go PH, Meadows MC, Deleon EM, Chamberlain RS (October 2010). "Elastofibroma dorsi: A soft tissue masquerade". Int J Shoulder Surg. 4 (4): 97–101. doi:10.4103/0973-6042.79797. PMC 3100815. PMID 21655005.
- ↑ Patrikeos A, Breidahl W, Robins P (September 2005). "F-18 FDG uptake associated with Elastofibroma dorsi". Clin Nucl Med. 30 (9): 617–8. PMID 16100483.