Dupuytrens contracture
| Dupuytren's contracture | |
 | |
|---|---|
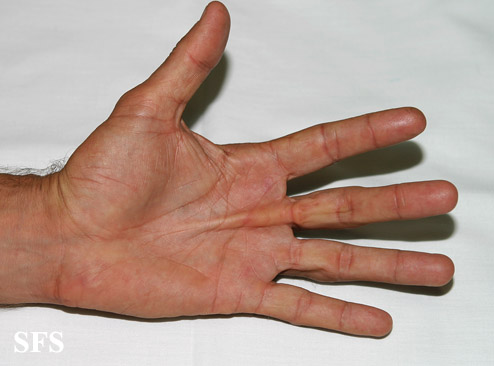
| Dupuytren's contracture of the fourth digit (ring finger). | |
| ICD-10 | M72.0 |
| ICD-9 | 728.6 |
| OMIM | 126900 |
| DiseasesDB | 4011 |
| MedlinePlus | 001233 |
Editors-In-Chief: Matthew I. Leibman, M.D.[1]; Mark R. Belsky, M.D.[2]; David E. Ruchelsman, M.D.[3]Kiran Singh, M.D. [4]
Synonyms and keywords: Dupuytren contracture I, included; DUPC1; palmar fascial fibromatosis; palmar fibromatosis
Overview
Dupuytren's contracture (also known as Morbus Dupuytren) is a fixed flexion contracture of the hand where the fingers bend towards the palm and cannot be fully extended (straightened). It is named after the famous surgeon Baron Guillaume Dupuytren, who described an operation to correct the affliction.
The ring finger and little finger are the fingers most commonly affected; the middle finger may be affected in advanced cases, but index finger and thumb are nearly always spared. Dupuytren's contracture progresses slowly and is usually painless. In patients with this condition, the tissues under the skin on the palm of the hand thicken and shorten so that the tendons connected to the fingers cannot move freely. The palmar aponeurosis becomes hyperplastic and undergoes contracture. As a result, the affected fingers start to bend more and more and cannot be straightened.
Incidence increases after the age of 40; at this age men are affected more often than women. After the age of 80 the distribution is about even.
Historical Perspective
- Dupuytren's contracture was named after Baron Guillaume Dupuytren, a famous surgeon, following describing an operation to correct the affliction.
Pathophysiology
Pathogenesis
- The exact pathogenesis of Dupuytren's contracture is not fully understood.
- It is thought that Dupuytren's contracture is the result of microvascular angiopathy.
Associated Conditions
Causes
The cause of Dupuytren's contracture has not been identified.
Symptoms
In Dupuytren's disease, the tough connective tissue within one's hand becomes abnormally thick, which can cause the fingers to curl, and can result in impaired function of the fingers, especially the small and ring fingers. It usually has a gradual onset, often beginning as a tender lump in the palm. Over time, pain associated with the condition tends to go away, but tough bands of tissue may develop. These bands, which are the source of the reduced mobility commonly associated with the condition, are visible on the surface of the palm, and may appear similar to a small callus. It commonly develops in both hands, and has no connection to dominant- or non-dominant hands, nor any correlation with right- or left-handedness.
The contracture sets on very slowly, especially in women. However, when present in both hands, and when there is associated foot involvement, it tends to accelerate more rapidly.
Epidemiology and Demographics
Prevalence
- The prevalence of Dupuytren's contracture among the UK population is 3-5%.
Age
- The incidence of Dupuytren's contracture increases with age; the median age at diagnosis is 50-70 years.
Race
- Dupuytren's contracture usually affects individuals of the northern Europeans race (Icelandic and Scandinavian populations).
Gender
- Males are more commonly affected by Dupuytren's contracture than females. The male to female ratio is approximately 3 to 1.
Risk Factors
Common risk factors in the development of Dupuytren's contracture include:
- Family history: genetic predisposition may account for 80% of cases.
- Diabetes and its medications
- Smoking
- Alcohol intake
- Antiepileptic medications
- There is also some speculation that Dupuytren's contracture may be caused by physical trauma, such as manual labor or other over-exertion of the hands. However, the fact that Dupuytren's is not connected with handedness casts some doubt on this claim.
- Surgery of the hand may trigger growth of Dupuytren nodules and cords if an inclination existed before.
- Certain occupations with repetitive hand trauma
Natural History, Complications and Prognosis
Natural History
- Dupuytren’s disease is progressive in nature with no available cure.
- Improvement of the painful nodules may occur with time, and many patients never experience a contracture.[1]
Prognosis
- Prognosis is generally poor.
- Development of Dupuytren's disease at an earlier age is associated with more severe deformities.[2]
Diagnosis
Diagnostic Study of Choice
Dupuytren’s disease is primarily diagnosed based on the clinical presentation.
History and Symptoms
Physical Examination
Skin
Hand
-

Dupuytren contracture. Adapted from Dermatology Atlas.
-

Dupuytren contracture. Adapted from Dermatology Atlas.
-
Dupuytren contracture. Adapted from Dermatology Atlas.
-
![Dupuytren contracture. Adapted from Dermatology Atlas.[3]](/images/1/1f/Dupuytren_contracture04.jpg)
Dupuytren contracture. Adapted from Dermatology Atlas.[3]
-
![Dupuytren contracture. Adapted from Dermatology Atlas.[3]](/images/2/2f/Dupuytren_contracture05.jpg)
Dupuytren contracture. Adapted from Dermatology Atlas.[3]
-
![Dupuytren contracture. Adapted from Dermatology Atlas.[3]](/images/e/e1/Dupuytren_contracture06.jpg)
Dupuytren contracture. Adapted from Dermatology Atlas.[3]



![Dupuytren contracture. Adapted from Dermatology Atlas.[3]](/index.php/File:Dupuytren_contracture04.jpg)
![Dupuytren contracture. Adapted from Dermatology Atlas.[3]](/index.php/File:Dupuytren_contracture05.jpg)
![Dupuytren contracture. Adapted from Dermatology Atlas.[3]](/index.php/File:Dupuytren_contracture06.jpg)
Treatment
- Surgery (in cases of severe contracture removes the contracture)
- Radiation therapy (specifically in early stages inhibits development of contracture)
- Needle aponeurotomy (releases the contracture)
- Triamcinolone (kenalog) injections provide some relief
Surgical management consists of opening the skin over the affected cords and excising, removing, the fibrous tissue. The fingers may then be brought out to length with the help of postoperative therapy. The procedure is not curative in that remaining non-affected fascia may still develop Dupuytren's disease later on, and therefore the patients may need repeat surgery. In addition, the thickened fascia often invests the digital nerves and arteries, so there is some risk of nerve and/or arterial injury.
Treatment of Dupuytren's disease with low energy x-rays (radiotherapy) may cure Morbus Dupuytren on a long term, specifically if applied in early stages of the disease. Needle aponevrotomy is a minimal invasive technique where the cords are weakened through the insertion and manipulation of a small needle. Once weakened, the offending cords may be snapped by simply pulling the finger(s) straight. The nodules are not removed and might start growing again. Currently in phase III of Food and Drug Administration (FDA) approval is another promising therapy, the injection of collagenase. This procedure is similar to needle aponevrotomy, however the chords are weakened through the injection of small amounts of an enzyme that dissolves them.
Dupuytren's contracture is not a dangerous condition, and often no treatment is necessary. Even when treatment is used, there is no permanent way to stop or cure the infliction. If there is a painful lump present, an injection can often help alleviate the pain. If pain persists or the function of the hand becomes seriously impaired, individuals often choose to have surgery. This surgery usually entails removing or separating the thickened bands, and is unlikely to cause any major complications or side effects, although in serious cases, some minor skin grafting may be necessary. Any damaged skin or tissue in the surgically affected area of the hand will heal fairly quickly, and reducing bloodflow during the healing period helps reduce pain. This may be done by keeping the hand raised or elevated so that blood does not pool in the affected area.
After surgical treatment, the condition may worsen in inadequately excised diseased tissue or re-develop in previously normal tissue.
External links
http://www.nlm.nih.gov/medlineplus/ency/article/001233.htm
Template:Diseases of the musculoskeletal system and connective tissue
de:Morbus Dupuytren
it:Malattia di Dupuytren
nl:Ziekte van Dupuytren
- ↑ Schmoldt A, Benthe HF, Haberland G (1975). "Digitoxin metabolism by rat liver microsomes". Biochem Pharmacol. 24 (17): 1639–41. PMID https://doi.org/10.1136/bmj.n1308 Check
|pmid=value (help). - ↑ Gudmundsson KG, Arngrimsson R, Jónsson T (2001). "Eighteen years follow-up study of the clinical manifestations and progression of Dupuytren's disease". Scand J Rheumatol. 30 (1): 31–4. doi:10.1080/030097401750065292. PMID 11252689.
- ↑ 3.0 3.1 3.2 "Dermatology Atlas".