Angiosarcoma: Difference between revisions
| Line 7: | Line 7: | ||
==Overview== | ==Overview== | ||
'''Angiosarcoma''' is a rare [[malignant]] vascular [[neoplasm]] of [[endothelial]]-type cells that line vessel walls. Angiosarcoma was first described by Dr. Juan Rosai, M.D. and colleagues in 1976.The pathogenesis of angiosarcoma is characterized by a rapid and extensively infiltrating overgrowth of vascular [[epithelial]] cells. Common angiosarcoma locations include the [[kidney]], [[liver]], [[lung]], and [[breast]]. The [[PTPRB]]/[[Phospholipase C|PLCG1]] [[genes]] are associated with the development of angiosarcoma; [[mutation]] of these genes result in aberrant [[angiogenesis]]. The imaging modality of choice for diagnosing angiosarcoma will depend on the location. For [[pulmonary]] angiosarcoma, the imaging modality of choice is enhanced CT scan. For other types angiosarcoma, the imaging modality of choice is MRI. On CT scan, findings suggestive of angiosarcoma may include vascular invasion, nodular enhancement (common), and a hypoattenuating mass. The mainstay [[adjuvant therapy]] for angiosarcoma is a [[doxorubicin]]-based regimen. The response rate for [[chemotherapy]] in patients with angiosarcoma is poor. | '''Angiosarcoma''' is a rare [[malignant]] vascular [[neoplasm]] of [[endothelial]]-type cells that line vessel walls. Angiosarcoma was first described by Dr. Juan Rosai, M.D. and colleagues in 1976.The pathogenesis of angiosarcoma is characterized by a rapid and extensively infiltrating overgrowth of vascular [[epithelial]] cells. Angiosarcoma may arise in any part of the body, but is more common in soft tissue than in bone. Common angiosarcoma locations include the [[kidney]], [[liver]], [[lung]], and [[breast]]. The [[PTPRB]]/[[Phospholipase C|PLCG1]] [[genes]] are associated with the development of angiosarcoma; [[mutation]] of these genes result in aberrant [[angiogenesis]]. The imaging modality of choice for diagnosing angiosarcoma will depend on the location. For [[pulmonary]] angiosarcoma, the imaging modality of choice is enhanced CT scan. For other types angiosarcoma, the imaging modality of choice is MRI. On CT scan, findings suggestive of angiosarcoma may include vascular invasion, nodular enhancement (common), and a hypoattenuating mass. The mainstay [[adjuvant therapy]] for angiosarcoma is a [[doxorubicin]]-based regimen. The response rate for [[chemotherapy]] in patients with angiosarcoma is poor. | ||
==Historical Perspective== | ==Historical Perspective== | ||
Revision as of 17:57, 6 February 2019
|
WikiDoc Resources for Angiosarcoma |
|
Articles |
|---|
|
Most recent articles on Angiosarcoma Most cited articles on Angiosarcoma |
|
Media |
|
Powerpoint slides on Angiosarcoma |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Angiosarcoma at Clinical Trials.gov Clinical Trials on Angiosarcoma at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Angiosarcoma
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Angiosarcoma Discussion groups on Angiosarcoma Patient Handouts on Angiosarcoma Directions to Hospitals Treating Angiosarcoma Risk calculators and risk factors for Angiosarcoma
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Angiosarcoma |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Maria Fernanda Villarreal, M.D. [2]
Synonyms and keywords: Hemangiosarcoma; Pulmonary angiosarcoma; Vascular sarcoma
Overview
Angiosarcoma is a rare malignant vascular neoplasm of endothelial-type cells that line vessel walls. Angiosarcoma was first described by Dr. Juan Rosai, M.D. and colleagues in 1976.The pathogenesis of angiosarcoma is characterized by a rapid and extensively infiltrating overgrowth of vascular epithelial cells. Angiosarcoma may arise in any part of the body, but is more common in soft tissue than in bone. Common angiosarcoma locations include the kidney, liver, lung, and breast. The PTPRB/PLCG1 genes are associated with the development of angiosarcoma; mutation of these genes result in aberrant angiogenesis. The imaging modality of choice for diagnosing angiosarcoma will depend on the location. For pulmonary angiosarcoma, the imaging modality of choice is enhanced CT scan. For other types angiosarcoma, the imaging modality of choice is MRI. On CT scan, findings suggestive of angiosarcoma may include vascular invasion, nodular enhancement (common), and a hypoattenuating mass. The mainstay adjuvant therapy for angiosarcoma is a doxorubicin-based regimen. The response rate for chemotherapy in patients with angiosarcoma is poor.
Historical Perspective
Angiosarcoma was first discovered by Dr. Juan Rosai, M.D. and colleagues in 1976.[1]
Classification
Angiosarcoma may be classified according to the clinical heterogeneity into two main groups, and every group can be subdivided into subtypes according to the anatomical location and etiology:
| Angiosarcoma | |
| Primary | Secondary |
| Cutaneous | Post Radiation Angiosarcoma |
| Breast | Lymphedema-associated Angiosarcoma |
| Soft tissue and Bone | Angiosarcoma due to exposure to mutatgens |
| Visceral | |
Pathophysiology
Pathogenesis
The pathogenesis of angiosarcoma is characterized by a rapid and extensive infiltrating overgrowth of vascular epithelial cells.[2] Angiosarcoma is a locally aggressive tumor with a high rate of lymph node infiltration and metastases.
Genetics
The PTPRB/PLCG1 genes are associated with the development of angiosarcoma by triggering aberrant angiogenesis.[2]
Gross Pathology
On gross pathology, characteristic findings of angiosarcoma may include:[2]
- Red/dark tan lesion
- Typically poorly circumscribed
Microscopic Pathology
On microscopic histopathological analysis, characteristic findings of angiosarcoma may include:
- Spindle cell lesion
- Epitheloid lesion
- Numerous irrergular capillaries
- Appears red on low power
- Pleomorphic nuclei
- Hobnail morphology
- Numerous mitotic bodies
- Cytoplasmic vacuoles
- Luminal arrangement of cells
Causes
Common causes of angiosarcoma include:[2]
- Exposure to vinyl chloride monomer (VCM) for prolonged periods
- Exposure to polyvinyl chloride (PVC) polymerisation plants
- Exposure to arsenic-containing insecticides
- Previous exposure to thorium dioxide irradiation
Differentiating Angiosarcoma from Other Diseases
Angiosarcoma must be differentiated from other diseases that cause a highly vascular mass or non-healing cutaneous ulcerations such as:
Differentials for Cutaneous Angiosarcoma
Cutaneous angiosarcoma must be differentiated from other diseases with non-healing cutaneous ulcerations such as:
Differentials for Non-cutaneous Angiosarcoma
Angiosarcoma must be differentiated from other diseases that cause a highly vascular mass such as:
- Atypical vascular lesions
- Hemangioma
- Glomangiosarcoma
- Carotid body tumor
- Malignant fibrous histiocytoma of soft tissue
Epidemiology and Demographics
Incidence
- In 2004, the age-adjusted incidence of angiosarcoma was 3.1 per 100,000 population per year.[3]
Age
- Angiosarcoma is more commonly observed among patients aged between 40 to 75 years old.[3]
Gender
- Males are more commonly affected with angiosarcoma than females.[3]
- The male to female ratio is 2:1.[3]
Race
- There is no racial predilection for angiosarcoma.
Risk Factors
Common risk factors in the development of angiosarcoma include:[2]
- Chronic lymphedema
- Chronic exposure to polyvinyl chloride (PVC)
- Radiation exposure
- Exposure to Thorotrast
Natural History, Complications and Prognosis
Natural History
- The majority of patients with angiosarcoma remain asymptomatic for years.[2]
- Early clinical features may include nonspecific symptoms, such as pain, fatigue, malaise, and nausea.
- If left untreated, the majority of patients with angiosarcoma may rapidly progress to develop metastases.[3]
Complications
Common complications of angiosarcoma include:[2]
Prognosis
- Prognosis is generally poor; the 5-year survival rate of patients with angiosarcoma is approximately 12-33%.
- Poor prognostic factors include patient age (> 65 years), retroperitoneal location, and large tumor size.[3]
Diagnosis
Symptoms
- Angiosarcoma is usually asymptomatic and found incidentally.
- Symptoms of angiosarcoma are generally non-specific.
Physical Examination
Patients with angiosarcoma may appear cachectic or normal. In cutaneous angiosarcoma, physical examination findings may include:
- Bruise or skin ulceration
- Blushed purple-red papule
Laboratory Findings
There are no specific laboratory findings associated with angiosarcoma.
Imaging Findings
- The imaging modality of choice for angiosarcoma will depend on the location.
- For pulmonary angiosarcoma, the imaging modality of choice is enhanced CT scan.[3] For other types angiosarcoma, the imaging modality of choice is MRI.
CT
On CT, findings of angiosarcoma may include:[3]
- Vascular invasion
- Nodular enhancement (common)
- Hypoattenuating mass
- Multicentric lesions
-
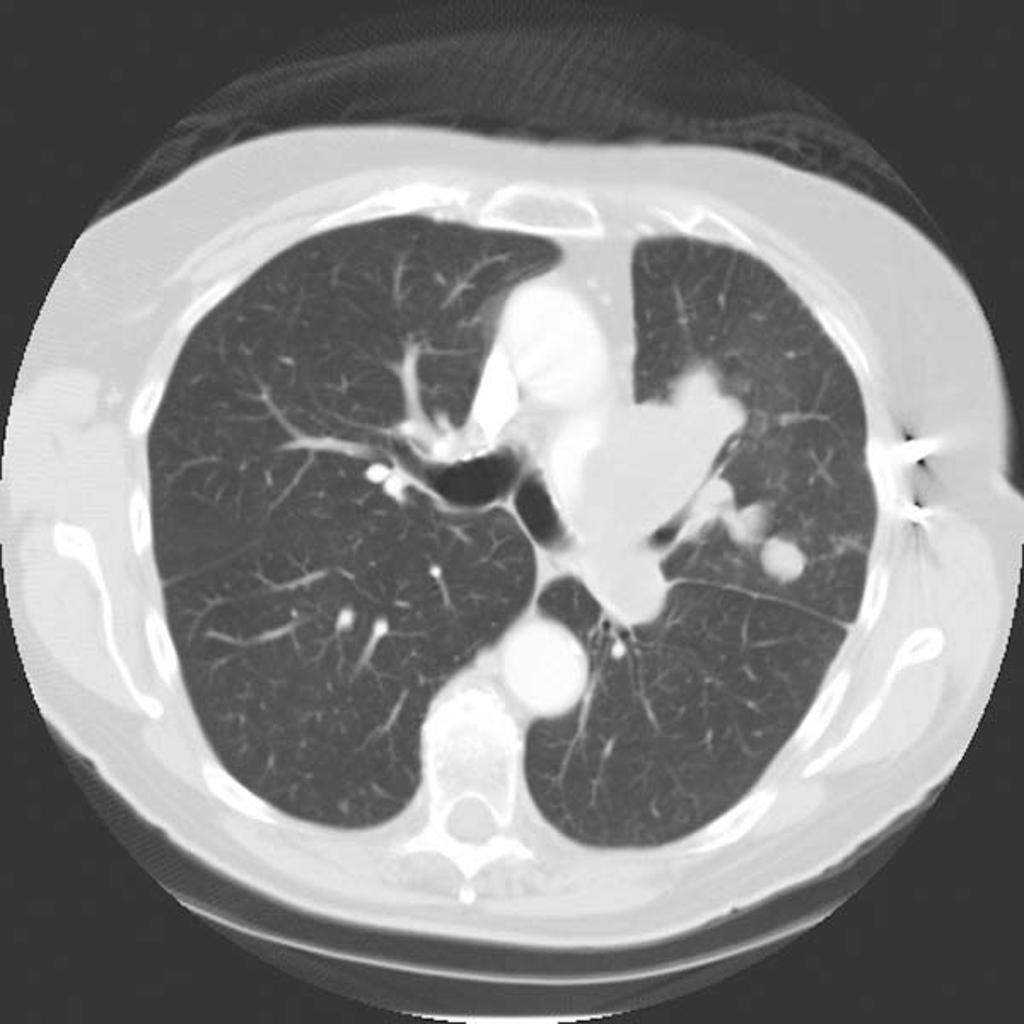
CT Pulmonary angiosarcoma
Courtesy of Radiopedia

MRI
On MRI, findings of angiosarcoma may include:
- T1/T2: heterogeneous areas of hyperintensity suggestive of a mixed tumour and hemorrhage
- T1 C+ (Gd): heterogeneous enhancement
Treatment
The mainstay of treatment for angiosarcoma is complete surgical resection with wide margins for local and locoregional disease in combination with preoperative or postoperative radiotherapy.[4] The role of adjuvant chemotherapy, is unclear.Adjuvant chemotherapy and/or radiotheray provide less mutilating surgery, and for patients with unresectable tumors or those who refuse surgery is an option.[5][6]
Medical Therapy
- The main adjuvant therapy for angiosarcoma is a doxorubicin-based regimen.[2] For angiosarcoma, doxorubicin monotherapy is indicated as first-line therapy.[2]
- Common complications of doxorubicin include:
- For patients with pulmonary angiosarcoma, a combination of radiotherapy and immunotherapy with recombinant interleukin-2 is the treatment of choice.[7] The response rate to chemotherapy in patients with angiosarcoma is poor.[2]
Surgery
Surgical resection in combination with radiation therapy is the treatment of choice for small angiosarcomas.[2]
- Surgical treatment for patients with cutaneous angiosarcoma is surgical resection with wide margins.[2] Surgery is not recommended on patients with large sized angiosarcomas. The recurrence rate of angiosarcoma after surgery is 80%.
Prevention
Primary Prevention
There are no primary preventive measures available for angiosarcoma.
Secondary Prevention
Once diagnosed and successfully treated, patients with angiosarcoma are followed-up every 3, 6, or 12 months depending on the stage at diagnosis. Follow-up testing for angiosarcoma may include:[2]
- Periodic imaging/angiography evaluation
- Laboratory testing: complete blood count (e.g., anemia)
References
- ↑ Barber W, Scriven P, Turner D, Hughes D, Wyld D (2010). "Epithelioid angiosarcoma: Use of angiographic embolisation and radiotherapy to control recurrent haemorrhage". J Surg Case Rep. 2010 (5): 7. doi:10.1093/jscr/2010.5.7. PMC 3649120. PMID 24946325.
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 2.12 Young RJ, Brown NJ, Reed MW, Hughes D, Woll PJ (2010). "Angiosarcoma". Lancet Oncol. 11 (10): 983–91. doi:10.1016/S1470-2045(10)70023-1. PMID 20537949.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 3.6 3.7 Sturgis EM, Potter BO. Sarcomas of the head and neck region. Curr Opin Oncol. 2003 May. 15(3):239-52
- ↑ W. M. Lydiatt, A. R. Shaha & J. P. Shah (1994). "Angiosarcoma of the head and neck". American journal of surgery. 168 (5): 451–454. PMID 7977971. Unknown parameter
|month=ignored (help) - ↑ Robin J. Young, Nicola J. Brown, Malcolm W. Reed, David Hughes & Penella J. Woll (2010). "Angiosarcoma". The Lancet. Oncology. 11 (10): 983–991. doi:10.1016/S1470-2045(10)70023-1. PMID 20537949. Unknown parameter
|month=ignored (help) - ↑ Guy Lahat, Asha R. Dhuka, Hen Hallevi, Lianchun Xiao, Changye Zou, Kerrington D. Smith, Thuy L. Phung, Raphael E. Pollock, Robert Benjamin, Kelly K. Hunt, Alexander J. Lazar & Dina Lev (2010). "Angiosarcoma: clinical and molecular insights". Annals of surgery. 251 (6): 1098–1106. doi:10.1097/SLA.0b013e3181dbb75a. PMID 20485141. Unknown parameter
|month=ignored (help) - ↑ Duck L, Baurain JF, Machiels JP (2004). "Treatment of a primary pulmonary angiosarcoma". Chest. 126 (1): 317–8, author reply 318. doi:10.1378/chest.126.1.317. PMID 15249484.