Adenomyosis
For patient information, click here
Template:DiseaseDisorder infobox
|
WikiDoc Resources for Adenomyosis |
|
Articles |
|---|
|
Most recent articles on Adenomyosis Most cited articles on Adenomyosis |
|
Media |
|
Powerpoint slides on Adenomyosis |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Adenomyosis at Clinical Trials.gov Clinical Trials on Adenomyosis at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Adenomyosis
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Adenomyosis Discussion groups on Adenomyosis Patient Handouts on Adenomyosis Directions to Hospitals Treating Adenomyosis Risk calculators and risk factors for Adenomyosis
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Adenomyosis |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Cafer Zorkun M.D. PhD.[2]
Overview
Adenomyosis is a medical condition characterized by the presence of ectopic endometrial tissue (the inner lining of the uterus) within the myometrium (the thick, muscular layer of the uterus).[1] [2]
The condition is typically found in women in the ages between 35 and 50. Patients with adenomyosis can have painful and/or profuse menses (dysmenorrhea & menorrhagia, respectively).
Adenomyosis may involve the uterus focally, creating an adenomyoma, or diffusely. With diffuse involvement, the uterus becomes bulky and heavier.
Causes
The cause of adenomyosis is unknown, although it has been associated with any sort of uterine trauma that may break the barrier between the endometrium and myometrium, such as a caesarean section, tubal ligation, pregnancy termination, and any pregnancy.
Some say that the reason adenomyosis is common in women between the ages of 35 and 50 is because it is between these ages that women have an excess of estrogen. Near the age of 35, women typically cease to create as much natural progesterone, which counters the effects of estrogen. After the age of 50, due to menopause, women do not create as much estrogen.
Differential Diagnosis of Adenomyosis
Adenomyosis is a cause of abnormal uterine bleeding and can result in infertility. There are several diseases which can result in excessive uterine bleeding and the following table is a description of various causes of excessive uterine bleeding.
| Clinical Features | Physical Examination | Diagnostic Findings | |
|---|---|---|---|
| Endometriosis |
|
|
|
| Adenomyosis[3] |
|
|
|
| Submucous uterine leiomyomas[4] |
|
|
|
| Pelvic Inflammatory disease[5] |
|
|
|
| Pelvic congestion Syndrome[6] |
|
|
|
Diagnosis
The uterus may be imaged using ultrasound (US) or magnetic resonance imaging (MRI). Transvaginal ultrasound is the most cost effective and most available. Either modality will show an enlarged uterus. On ultrasound, the uterus will have a heterogeneous texture, without the focal well-defined masses that characterize uterine fibroids.
MRI provides better diagnostic capability due to the increased spatial and contrast resolution, and to not being limited by the presence of bowel gas or calcified uterine fibroids (as is ultrasound). In particular, MR is better able to differentiate adenomyosis from multiple small uterine fibroids. The uterus will have a thickened junctional zone with diminished signal on both T1 and T2 weighted sequences due to susceptibility effects of iron deposition due to chronic microhemorrhage. A thickness of the junctional zone greater than 10 to 12 mm (depending on who you read) is diagnostic of adenomyosis (<8 mm is normal). Interspersed within the thickened, hypointense signal of the junctional zone, one will often see foci of hyperintensity (brightness) on the T2 weighted scans representing small cystically dilatated glands or more acute sites of microhemorrhage.
MR can be used to classify adenomyosis based on the depth of penetration of the ectopic endometrium into the myometrium.
Diagnostic Findings
Ultrasonography
- Typical appearances of adenomyosis at transvaginal ultrasound include poorly marginated hypoechoic and heterogeneous areas within the myometrium, myometrial cysts, and a globular or enlarged uterus with asymmetry.
-
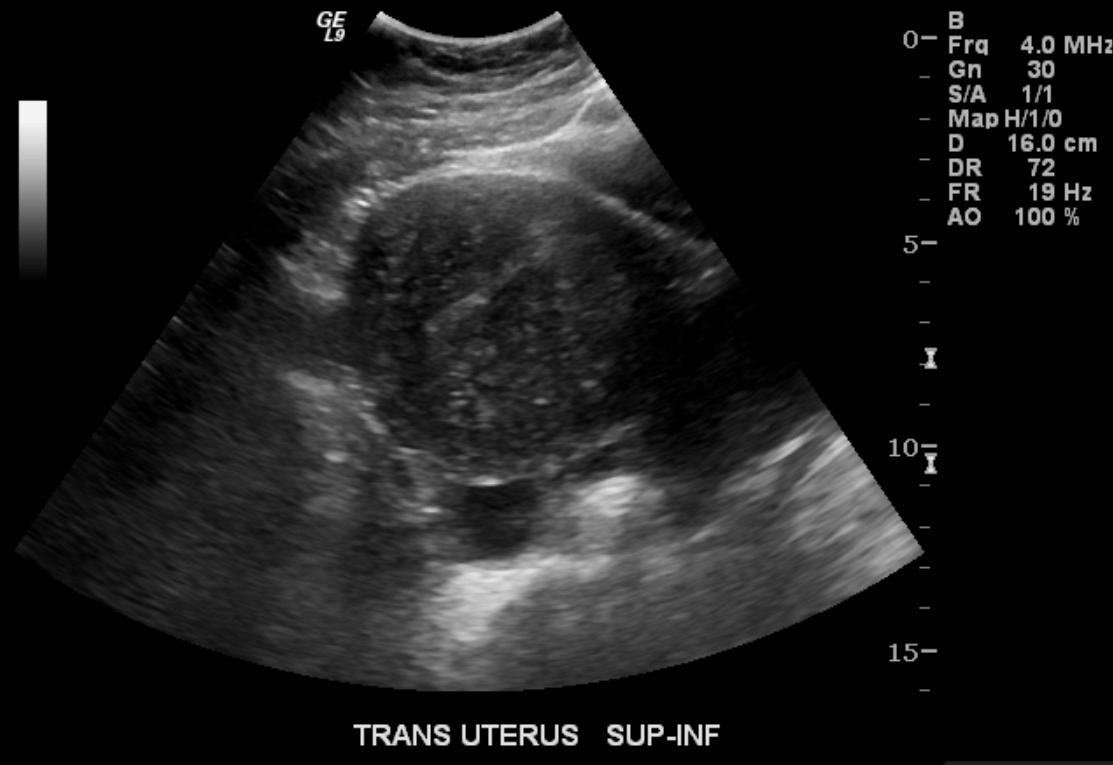
US: Adenomyosis
-
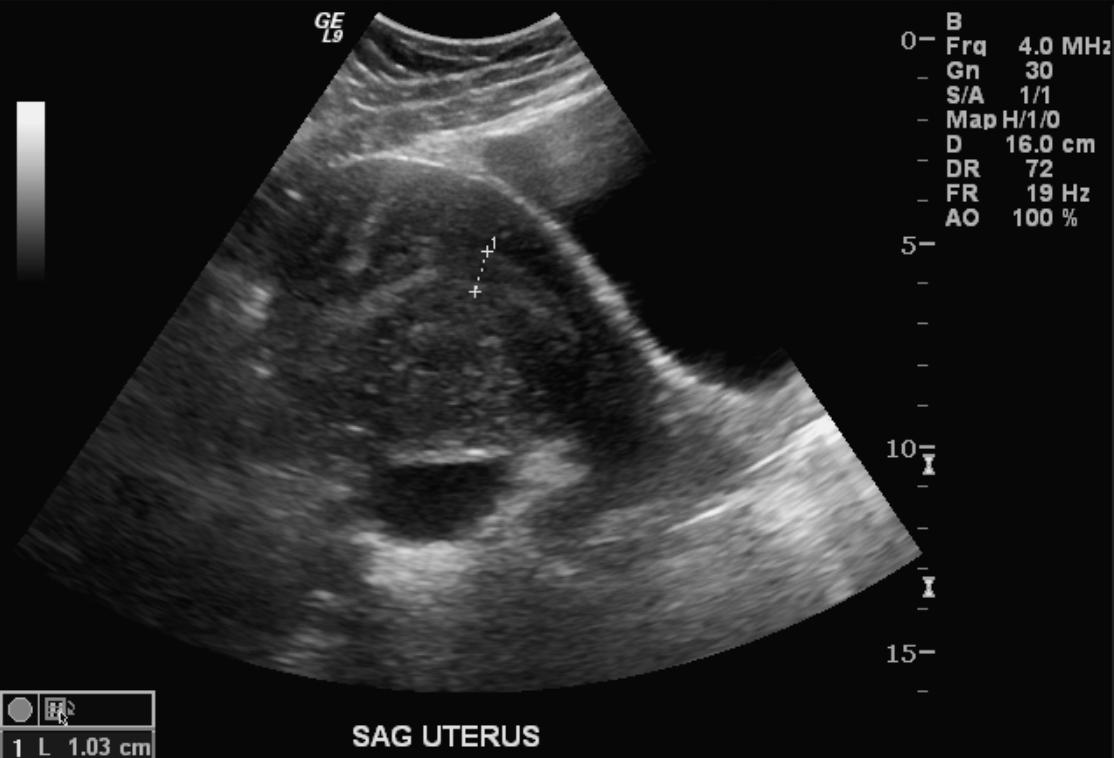
US: Adenomyosis
-
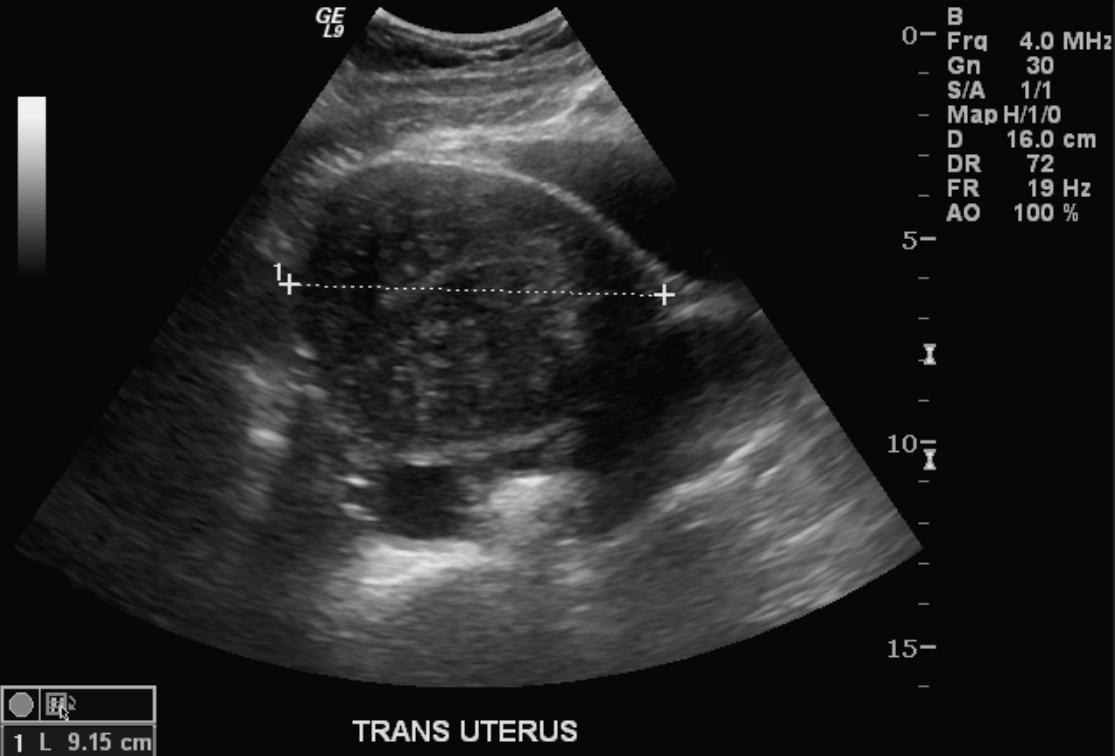
US: Adenomyosis



Computed Tomography
-

CT: Adenomyosis
-

CT: Adenomyosis


Magnetic Resonance Imaging
- Adenomyosis appears as either diffuse or focal thickening (greater than 12 mm )of the junctional zone forming an ill-defined area of low signal intensity, occasionally with embedded bright foci on T2-weighted images.
- Histologically, areas of low signal intensity correspond to smooth muscle hyperplasia, and bright foci on T2-weighted images correspond to islands of ectopic endometrial tissue and cystic dilatation of glands.
-
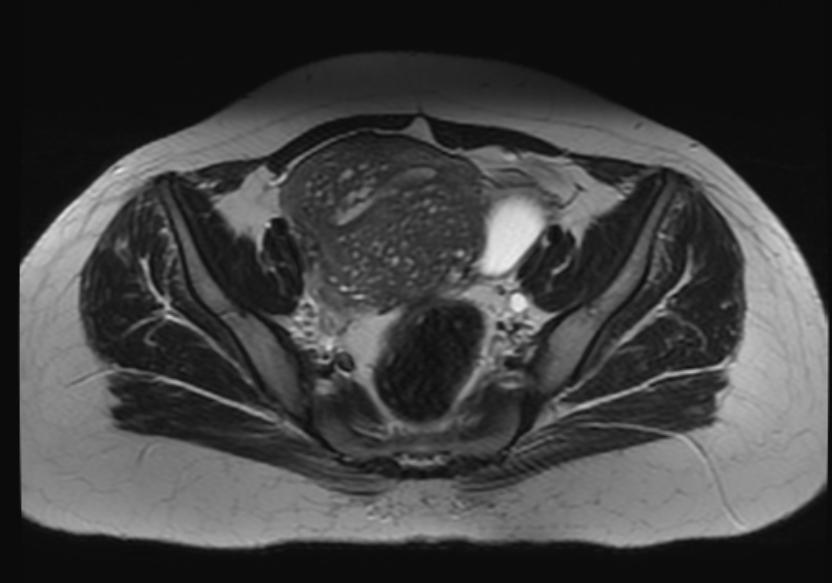
T2: Adenomyosis
-
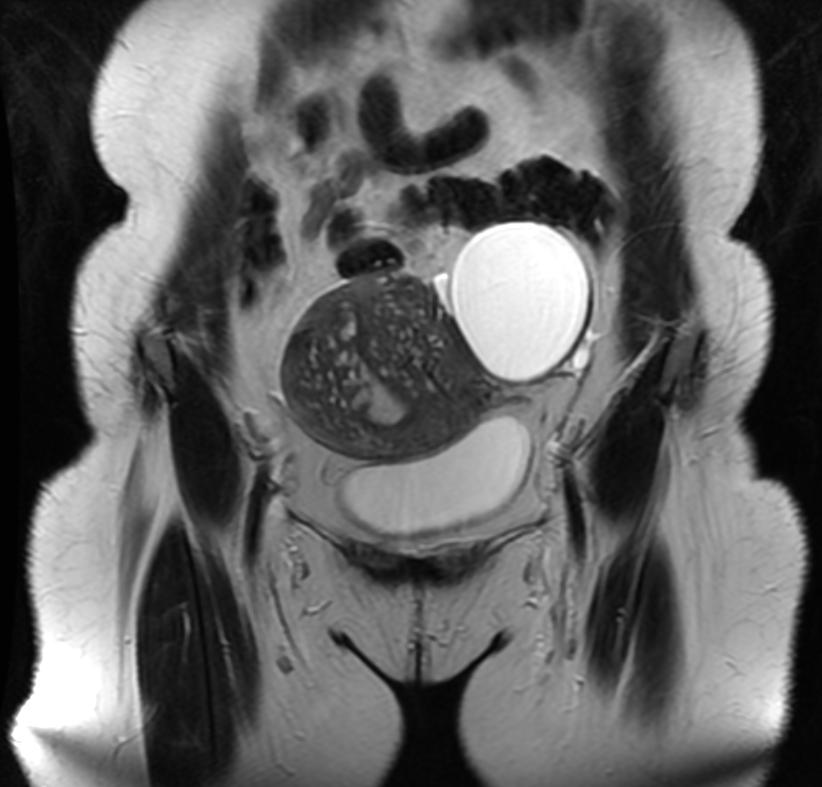
T2: Adenomyosis
-
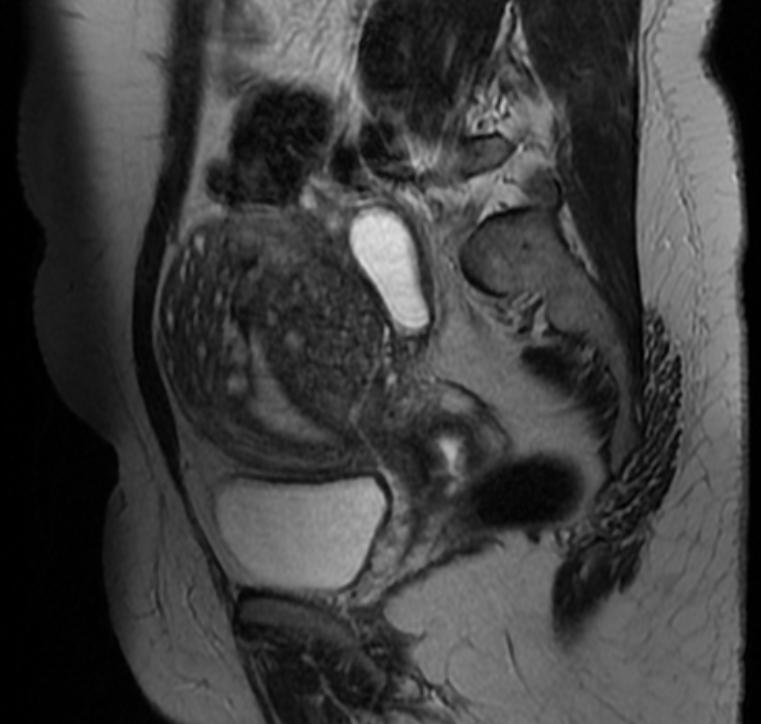
T2: Adenomyosis
-
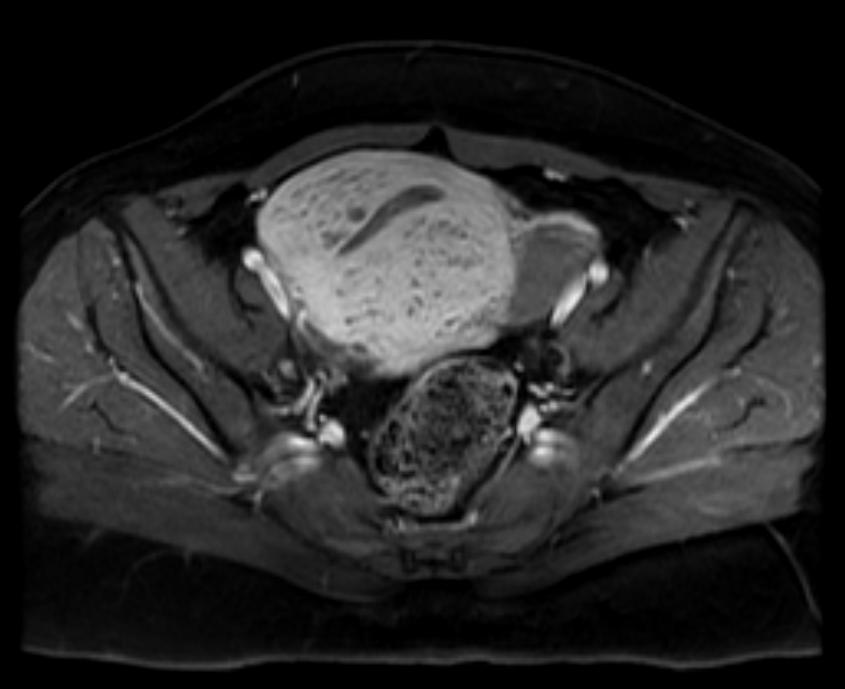
T1 fat sat contrast: Adenomyosis






Histopathology
{{#ev:youtube|nOCtpIwCZ-Y}}
Treatment
Treatment options range from use of NSAIDS & hormonal suppression for symptomatic relief, with hysterectomy the only permanent cure option. Women with Adenomyosis fail endometrial ablation because the ablation only affects the surface endometrial tissue, not the tissue that has grown into the muscle lining. This remaining tissue is still viable and will continue to cause pain. The result of failed ablation due to Adenomyosis is hysterectomy.
Those that believe an excess of estrogen is the cause or adenomyosis, or that it aggravates the symptoms, recommend avoiding products with xenoestrogens and/or recommend taking natural progesterone supplements.
Prognosis
There is no increased risk for cancer development. As the condition is estrogen-dependent, menopause presents a natural cure. Patients with adenomyosis often also have leiomyomata and/or endometriosis.
References
- ↑ Katz VL. Benign gynecologic lesions: vulva, vagina, cervix, uterus, oviduct, ovary. In: Katz VL, Lentz GM, Lobo RA, Gershenson DM, eds. Comprehensive Gynecology. 5th ed. Philadelphia, Pa: Mosby Elsevier; 2007: Chapter 18.
- ↑ Speroff L, Fritz MA. Dysfunction uterine bleeding. In. Speroff L, Fritz MA, eds. Clinical Gynecologic Endocrinology and Infertility. 7th ed. Philadelphia, Pa: Lippincott Williams and Wilkins; 2005: Chapter 15.
- ↑ Parker JD, Leondires M, Sinaii N, Premkumar A, Nieman LK, Stratton P (2006). "Persistence of dysmenorrhea and nonmenstrual pain after optimal endometriosis surgery may indicate adenomyosis". Fertil Steril. 86 (3): 711–5. doi:10.1016/j.fertnstert.2006.01.030. PMID 16782099.
- ↑ Donnez J, Donnez O, Matule D, Ahrendt HJ, Hudecek R, Zatik J; et al. (2016). "Long-term medical management of uterine fibroids with ulipristal acetate". Fertil Steril. 105 (1): 165–173.e4. doi:10.1016/j.fertnstert.2015.09.032. PMID 26477496.
- ↑ Ross J, Judlin P, Jensen J, International Union against sexually transmitted infections (2014). "2012 European guideline for the management of pelvic inflammatory disease". Int J STD AIDS. 25 (1): 1–7. doi:10.1177/0956462413498714. PMID 24216035.
- ↑ Rozenblit AM, Ricci ZJ, Tuvia J, Amis ES (2001). "Incompetent and dilated ovarian veins: a common CT finding in asymptomatic parous women". AJR Am J Roentgenol. 176 (1): 119–22. doi:10.2214/ajr.176.1.1760119. PMID 11133549.
Additional Resources
- Atri M, Reinhold C, Mehio AR. Adenomyosis: US features with histologic correlation in an in-vitro study. Radiology. Jun 2000;215(3):783-90.
- Batzer FR, Hansen L. Bizarre sonographic appearance of an adenomyoma and its presentation. J Ultrasound Med. Aug 1996;15(8):599-602.
- Bazot M, Daraï E. [Evaluation of pelvic endometriosis: the role of MRI.]. J Radiol. Nov 2008;89(11 Pt 1):1695-6.
- Byun JY, Kim SE, Choi BG, et al. Diffuse and focal adenomyosis: MR imaging findings. Radiographics. Oct 1999;19 Spec No:S161-70.
- Chiang CH, Chang MY, Hsu JJ. Tumor vascular pattern and blood flow impedance in the differential diagnosis of leiomyoma and adenomyosis by color Doppler sonography. J Assist Reprod Genet. May 1999;16(5):268-75.
- Guilbeault H, Wilson SR, Lickrish GM. Massive uterine enlargement with necrosis: an unusual manifestation of adenomyosis. J Ultrasound Med. Apr 1994;13(4):326-8.
- Haimovici JB, Tempany CM. MR of the female pelvis: benign disease. Appl Radiol. Jun 1994;7:21.
- Huang HY. Medical treatment of endometriosis. Chang Gung Med J. Sep-Oct 2008;31(5):431-40.
- Iribarne C, Plaza J, De la Fuente P, et al. Intramyometrial cystic adenomyosis. J Clin Ultrasound. Jun 1994;22(5):348-50.
- Jarlot C, Anglade E, Paillocher N, Moreau D, Catala L, Aubé C. [MR imaging features of deep pelvic endometriosis: correlation with laparoscopy.]. J Radiol. Nov 2008;89(11 Pt 1):1745-54.
- Kang S, Turner DA, Foster GS, et al. Adenomyosis: specificity of 5 mm as the maximum normal uterine junctional zone thickness in MR images. AJR Am J Roentgenol. May 1996;166(5):1145-50.
- Kim MD, Lee HS, Lee MH, Kim HJ, Cho JH, Cha SH. Long-term results of symptomatic fibroids treated with uterine artery embolization: In conjunction with MR evaluation. Eur J Radiol. Dec 10 2008;
- Ostrzenski A. Extensive iatrogenic adenomyosis after laparoscopic myomectomy. Fertil Steril. Jan 1998;69(1):143-5.
- Piketty M, Chopin N, Dousset B, Millischer-Bellaische AE, Roseau G, Leconte M, et al. Preoperative work-up for patients with deeply infiltrating endometriosis: transvaginal ultrasonography must definitely be the first-line imaging examination. Hum Reprod. Dec 17 2008;
- Piketty M, Chopin N, Dousset B, Millischer-Bellaische AE, Roseau G, Leconte M, et al. Preoperative work-up for patients with deeply infiltrating endometriosis: transvaginal ultrasonography must definitely be the first-line imaging examination. Hum Reprod. Dec 17 2008;
- Reinhold C, Atri M, Mehio A, et al. Diffuse uterine adenomyosis: morphologic criteria and diagnostic accuracy of endovaginal sonography. Radiology. Dec 1995;197(3):609-14.
- Reinhold C, Tafazoli F, Mehio A, et al. Uterine adenomyosis: endovaginal US and MR imaging features with histopathologic correlation. Radiographics. Oct 1999;19 Spec No:S147-60.
- Tamai K, Koyama T, Umeoka S, et al. Spectrum of MR features in adenomyosis. Best Pract Res Clin Obstet Gynaecol. Aug 2006;20(4):583-602.
- Tamai K, Togashi K, Ito T, et al. MR imaging findings of adenomyosis: correlation with histopathologic features and diagnostic pitfalls. Radiographics. Jan-Feb 2005;25(1):21-40.
- Utsunomiya D, Notsute S, Hayashida Y, et al. Endometrial carcinoma in adenomyosis: assessment of myometrial invasion on T2-weighted spin-echo and gadolinium-enhanced T1-weighted images. AJR Am J Roentgenol. Feb 2004;182(2):399-404.
Template:Diseases of the pelvis, genitals and breasts