How to read an ECG
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Rim Halaby
Overview
The interpretation of an ECG should be done in a consistent step-by-step way. Each ECG should be evaluated for the following:
- Rhythm
- Rate
- Conduction
- PR interval
- QRS duration
- QT duration
- Heart axis
- P wave morphology
- QRS morphology
- ST morphology
- Compare the current ECG to previous ECG
Rhythm
The sinus node (SA), located in the roof of the right atrium, is the fastest physiological pacemaker. When the sinus node generates an electrical impulse, the surrounding cells of the right atrium depolarize. Then the depolarization wave spreads to the cells of the left atrium, the AV (atrioventricular) node, the bundle of His and then to the ventricles through the purkinje fibers.
In order to evaluate the rhythm, several parameters must be checked:
- The presence of a P wave
- A rhythm is sinus when every P wave is always followed by a QRS wave
- P wave is absent in atrial fibrillation, junctional or ventricular rhythm
- The P wave morphology
- The P wave corresponds to atrial contraction
- Normal P waves are similar in shapes in the same lead
- Variable morphologies of P waves in a single ECG lead is suggestive of an ectopic pacemaker rhythm such as wandering pacemaker or multifocal atrial tachycardia
- The maximum height of the P wave is 2.5 mm in II and/or III
- The regularity of the waves
- The distance between two R waves, called RR interval, is constant in a regular rhythm
- When the RR interval is not constant, the rhythm is said irregular. When the rhythm is irregularly irregular it is a sign of the presence of atrial fibrillation.
-
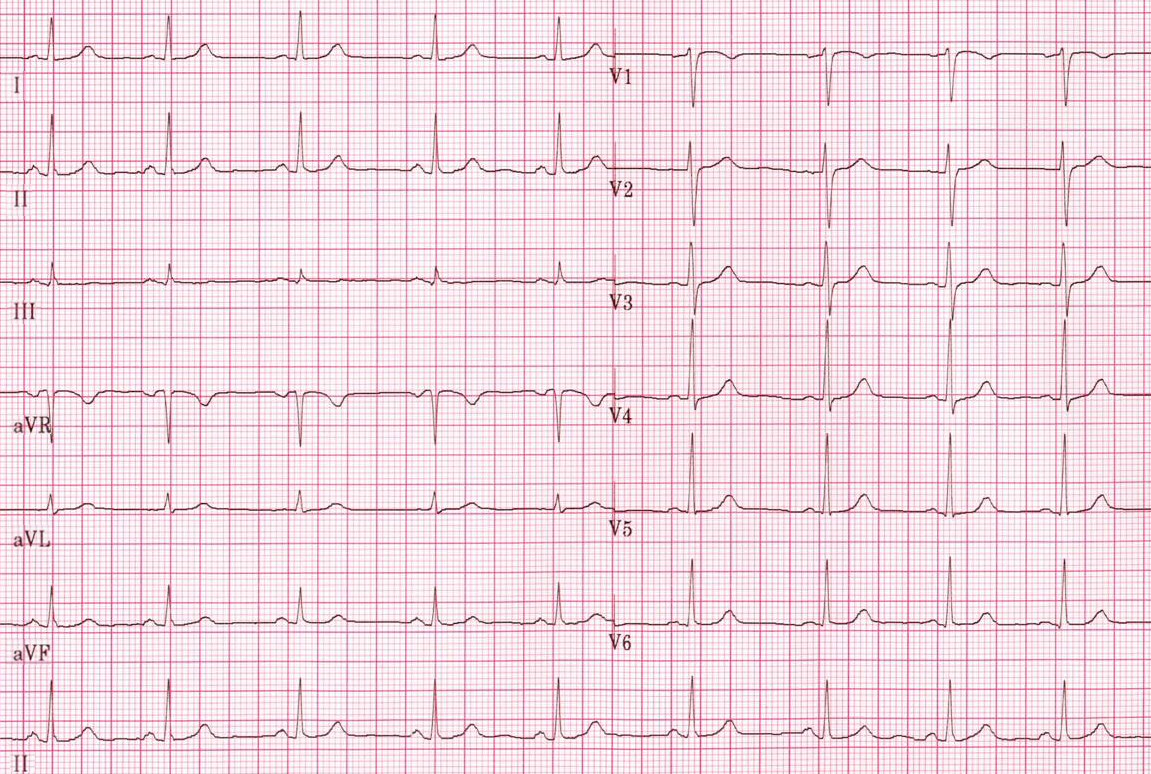
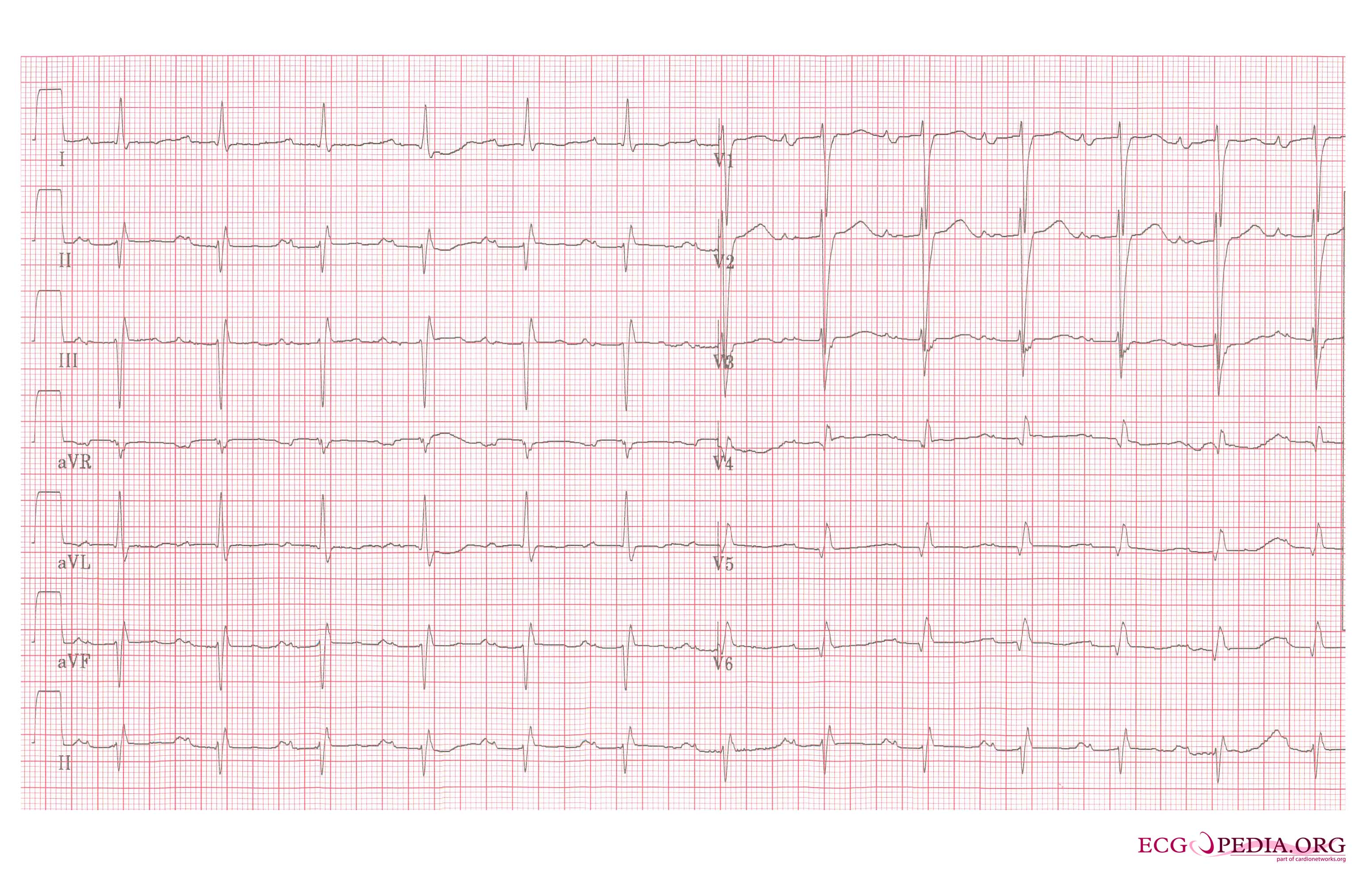
Normal sinus rhythm.
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
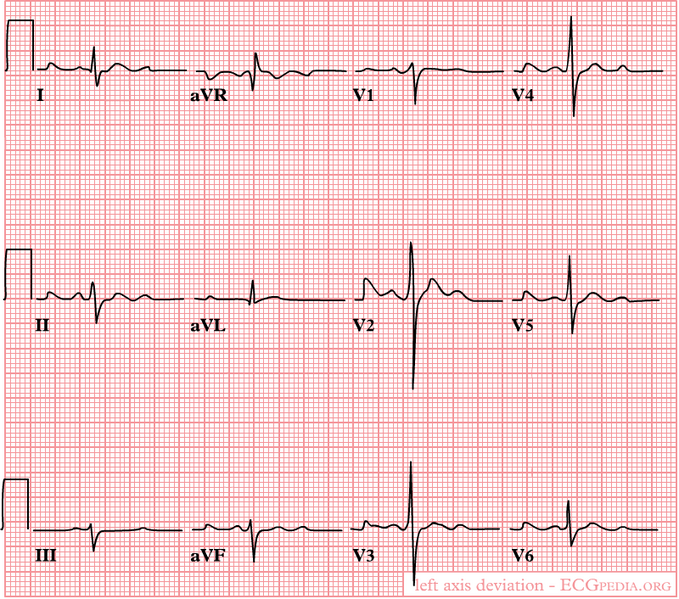
A left heart axis is present when the QRS in lead I is positive and negative in II and III.
-
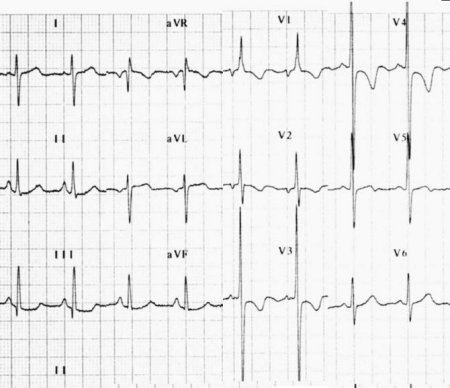
A right heart axis is present when lead I is negative and III positive.



Interpretation of an Abnormal Cardiac Axis
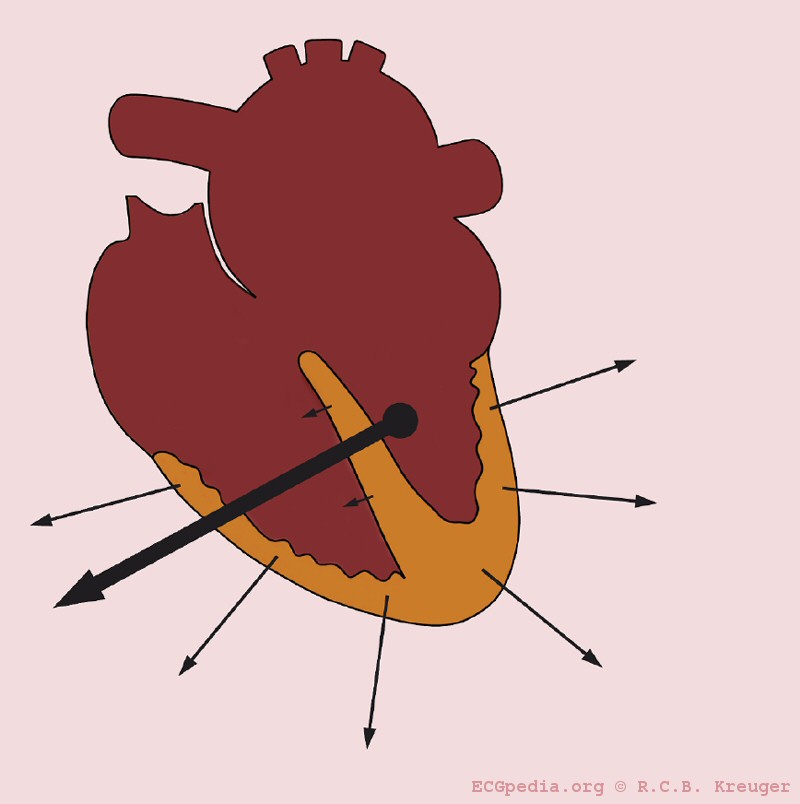
- 1- Actual rotation of the heart: When the heart itself is rotated (right ventricular overload), obviously the axis turns with it.
- The picture below illustrates heart axis deviation to the right in right ventricular load, as in COPD or pulmonary embolism. A right axis is between +90 and +180 degrees. In this case the axis is +135 degrees
-
Right axis deviation

- 2- Ventricular hypertrophy: The axis will deviate towards the greater electrical activity and the vector will turn towards the hypertrophied tissue.
- 3- Infarcted tissue: An infarcted tissue is electrically dead and thus no electrical activity is registered and the QRS vector turns away from the infarcted tissue
- The picture below illustrates heart axis deviation to the left in case of an inferior infarct. Left anterior hemiblock is a common cause. A left axis is between -30 and -90 degrees. The axis is -30 degrees.
-
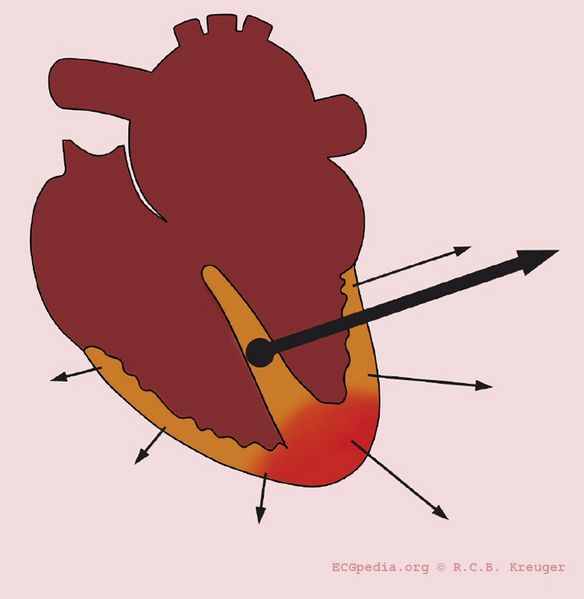
Left axis deviation in the case of an inferior infarct

- 4- Conduction problems: When RBBB is present the right ventricle depolarizes later than the left ventricle. In a normal situation the vector is influenced by the left ventricle, but in RBBB only the right ventricle determines it.
Causes of Left Axis Deviation
- Normal variation (physiologic, often with age)
- Mechanical shifts, such as expiration, high diaphragm (pregnancy, ascites, abdominal tumor)
- Left ventricular hypertrophy
- Left bundle branch block
- Left anterior fascicular block
- Congenital heart disease (e.g. atrial septal defect)
- Emphysema
- Hyperkalemia
- Ventricular ectopic rhythms
- Preexcitation syndromes
- Inferior myocardial infarction
- Pacemaker rhythm
Causes of Right Axis Deviation
- Normal variation (vertical heart with an axis of 90º)
- Mechanical shifts, such as inspiration and emphysema
- Right ventricular hypertrophy
- Right bundle branch block
- Left posterior fascicular block
- Dextrocardia
- Ventricular ectopic rhythms
- Preexcitation syndromes
- Lateral wall myocardial infarction
- Right ventricular load, for example Pulmonary Embolism or Cor Pulmonale (as in COPD)
The P Wave Morphology
Evaluation of the P wave
The P wave represents atrial depolarization (stimulation). At rapid rates, the P wave may merge with the preceding T wave and become difficult to identify.
The evaluation of the P wave should include the following:
1. Examination of the P wave contour
- The P wave contour is normally smooth, and is either entirely positive or entirely negative wave (monophasic wave) in all leads except V1.

2. Measurement of the P wave duration
- The P wave duration is normally less than 0.12 seconds
- Widened P waves can be a sign of Class Ia antiarrhythmic drugs intoxication (quinidine, etc.) and small or absent P waves can be a sign of hyperkalemia.
3. Measurement of the maximal P wave amplitude
- The maximal P-wave amplitude is normally no more than 0.2 mV in the frontal plane leads and no more than 0.1 mV in the transverse plane leads.
- If the p-wave is enlarged, the atria are enlarged.
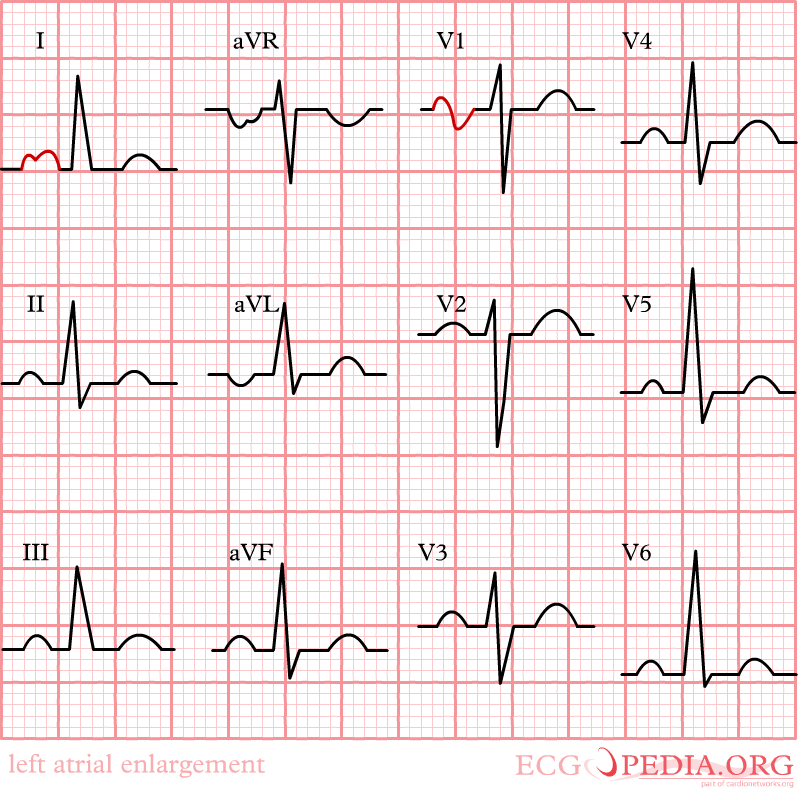
- Characteristics of the P wave in left atrial enlargement:
- P wave with a broad (>0.04 sec or 1 small square) and deeply negative (>1 mm) terminal part in V1 (P mitrale)
- P wave duration >0.12 sec in leads I and / or II
-
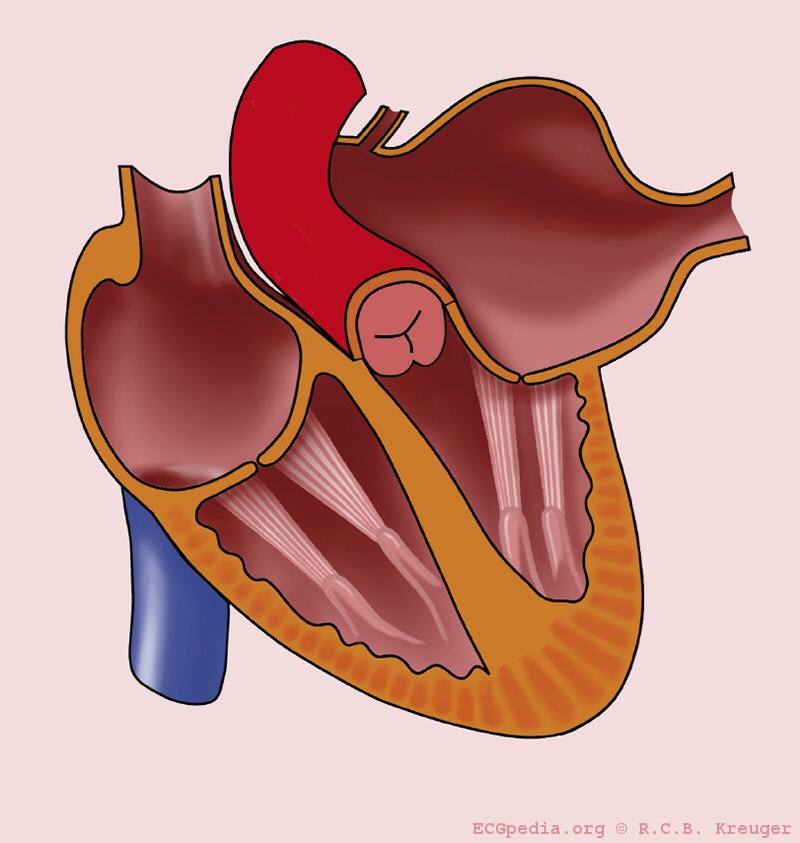
Left atrial enlargement
-
Left atrial enlargement with ECG.
-
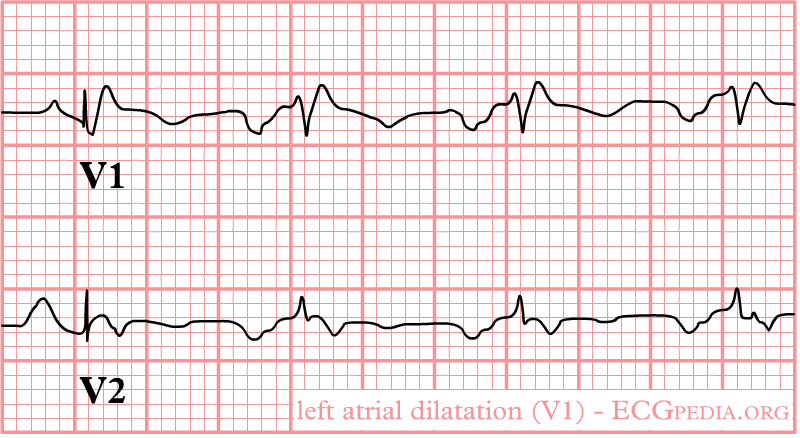
Left atrial enlargement as seen in lead V1.
-
Left atrial enlargement, a 12 lead ECG




- Characteristics of the P wave in right atrial enlargement:
- P is taller than 2.5 mm in II / III and / or aVF (P pulmonale)
- P >1.5 mm in V1
-
Right atrial enlargement

4. Estimation of the P wave axis
- The P wave normally appears entirely upright on leftward and inferiorly oriented leads such as I, II, aVF, and V4 to V6
- It is negative in aVR because of the rightward orientation of that lead, and it is variable in the other standard leads.
- Differential diagnosis of inverted P waves in I and aVL include dextrocardia and reversed arm lead

- Inverted P Wave in the Inferior Leads, as shown in the picture below, may occur in the setting of a low atrial focus as the origin of the rhythm.

5. Consistency of the P wave shape.
5. The relationship between the P wave and the QRS wave.
6. Morphology of the PTa segment
- Elevation or depression of the PTa segment (the part between the p wave and the beginning of the QRS complex) can result from atrial infarction or pericarditis.
