Necrotizing enterocolitis: Difference between revisions
No edit summary |
|||
| (2 intermediate revisions by 2 users not shown) | |||
| Line 42: | Line 42: | ||
NEC has no definitive known cause. An infectious agent has been suspected, as cluster outbreaks in [[neonatal intensive care unit]]s (NICUs) have been seen, but no common organism has been identified. A combination of intestinal flora, inherent weakness in the neonatal immune system, alterations in mesenteric blood flow and milk feeding may be factors. | NEC has no definitive known cause. An infectious agent has been suspected, as cluster outbreaks in [[neonatal intensive care unit]]s (NICUs) have been seen, but no common organism has been identified. A combination of intestinal flora, inherent weakness in the neonatal immune system, alterations in mesenteric blood flow and milk feeding may be factors. | ||
===Drug side effect=== | |||
* [[Ibuprofen lysine]] | |||
'''NEC is almost never seen in infants before oral feedings are initiated.''' | '''NEC is almost never seen in infants before oral feedings are initiated.''' | ||
| Line 156: | Line 158: | ||
{{Certain conditions originating in the perinatal period}} | {{Certain conditions originating in the perinatal period}} | ||
[[de:Nekrotisierende Enterokolitis]] | [[de:Nekrotisierende Enterokolitis]] | ||
| Line 171: | Line 166: | ||
{{WH}} | {{WH}} | ||
{{WikiDoc Sources}} | {{WikiDoc Sources}} | ||
[[Category:Disease]] | |||
[[Category:Pediatrics]] | |||
[[Category:Neonatology]] | |||
[[Category:Digestive diseases]] | |||
[[Category:Emergency medicine]] | |||
Latest revision as of 01:36, 28 April 2015
For patient information, click here
| Necrotizing enterocolitis | |
 | |
|---|---|
| Necrotizing enterocolitis | |
| ICD-10 | P77 |
| ICD-9 | 777.5 |
| DiseasesDB | 31774 |
| MedlinePlus | 001148 |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Necrotizing enterocolitis (NEC) is a medical condition primarily seen in premature infants, where portions of the bowel undergo necrosis (tissue death).
Necrotizing enterocolitis (NEC) is one of the most common acquired, life-threatening gastrointestinal diseases in the newborn, affecting 1%–5% of neonatal intensive care unit admissions and up to 10% of neonates under 1500 g.
The incidence of NEC is inversely proportional to the gestational age.
Of term infants, congenital heart disease is the main risk factor in this group. Other risk factors include perinatal asphyxia, patent ductus arteriosus, indomethacin therapy, and decreased umbilical flow in utero.
NEC most commonly manifests within the first or second week of life.
The symptoms referable to the gastrointestinal tract include feeding intolerance, vomiting, diarrhea, and blood in the stool. However, there may also be non-specific generalized symptoms including lethargy, temperature and blood pressure instability, and apnea.
Prompt institution of therapy, which includes bowel rest with a nasogastric tube, antibiotics, and adequate hydration (total parenteral nutrition), is essential to limit clinical progression and the development of complications.
The overall mortality rate in NEC is between 20% and 40% and is higher in neonates of very low birth weight.
Because of the higher mortality rate following perforation, earlier detection of severely ischemic or necrotic loops of bowel before perforation occurs could potentially improve the morbidity and mortality in NEC.
Etiology
NEC has no definitive known cause. An infectious agent has been suspected, as cluster outbreaks in neonatal intensive care units (NICUs) have been seen, but no common organism has been identified. A combination of intestinal flora, inherent weakness in the neonatal immune system, alterations in mesenteric blood flow and milk feeding may be factors.
Drug side effect
NEC is almost never seen in infants before oral feedings are initiated.
Signs and symptoms
The condition is typically seen in premature infants, and the timing of its onset is generally inversely proportional to the gestational age of the baby at birth. i.e. the earlier a baby is born, the later signs of NEC are typically seen.
Initial symptoms include feeding intolerance, increased gastric residuals, abdominal distension and bloody stools. Symptoms may progress rapidly to abdominal discoloration with intestinal perforation and peritonitis and systemic hypotension requiring intensive medical support.
Diagnosis
The diagnosis is usually suspected clinically but often requires the aid of diagnostic imaging modalities. Plain radiographs of the abdomen are useful by showing evidence of extraluminal gas (pneumotosis, portal venous gas or pneumoperitoneum) or an abnormal bowel gas pattern, particularly a persistently unaltered gas-filled dilated loop of bowel on serial radiographs (fixed loop). More recently ultrasonography has proven to be useful as it may detect signs and complications of NEC before they are evident on radiographs.
Imaging Findings for Necrotizing enterocolitis
Plain film
- Plain abdominal radiography is the current modality of choice for the evaluation of neonates suspected of having NEC.
- The timing of follow-up plain abdominal radiographs depends on the severity of the NEC and may vary from 6 to 24 hourly.
- The main observations to be made on the plain abdominal radiograph relate primarily to the presence, amount, and distribution of gas, which includes intraluminal gas, pneumatosis, portal venous gas, and pneumoperitoneum.
- In normal neonates, gas is most often present through most of the small and large bowel and each gas-filled loop causes an impression on adjacent loops. The loops develop a multifaceted configuration, giving the gas pattern a "mosaic" appearance.
- Dilatation with loss of the mosaic pattern and the development of rounded or elongated loops is more suggestive that an abnormality is present.
Bowel Gas Pattern
- In NEC, bowel dilatation is a nonspecific finding best appreciated on the plain abdominal radiograph and may be the only sign present in many patients with either mild or severe forms of the disease. The dilatation is usually due to an ileus and may be generalized or focal, depending on the extent of bowel involvement. It is the commonest sign, being present in over 90% of patients, with the remaining 10% showing only minor or nonspecific disturbances of bowel gas pattern.
- Dilatation of bowel is an early sign and may even precede the clinical features of NEC by several hours.
- The degree of dilatation usually correlates well with the clinical severity of the disease and the distribution of the dilated loops in serial examinations is related to clinical progression.
- Worrisome if the dilated loops maintain the same appearance as fixed loops on follow-up plain abdominal radiographs. This suggests the development of full-thickness necrosis and may precede clinical deterioration including signs of peritonitis.
Pneumotosis
- Pneumotosis is also an early sign that may precede clinical signs.
- Although intramural gas may be present in other neonatal conditions, it is most commonly seen in NEC and thus has been considered a virtually pathognomonic sign of NEC.
- Pneumotosis is more commonly present in the distal small bowel and large bowel and is therefore most commonly seen in the right lower quadrant.
- On plain abdominal radiographs, intramural gas may be diffuse or localized and appears as linear or rounded radiolucencies.
- The linear lucencies often appear curvilinear; they represent intramural gas in the subserosa and appear as black lines on the radiograph, which can occasionally be confused with overlapping bowel loops filled with gas.
- A clue to differentiating intramural gas from overlapping loops are the white lines that often accompany the black lines of intramural gas. The white lines represent the mucosa and submucosa, which are lifted off the serosa and are contrasted by the subserosal intramural gas and the intraluminal gas.
Portal venous gas
- In NEC, portal venous gas is an extension of intramural gas that enters the veins of the bowel wall and passes into the portal venous system.
- Portal venous gas has been reported on plain abdominal radiographs in up to 30% of neonates with NEC, and these are usually, but not always, the more severely affected cases. Portal venous gas is not always associated with a fatal outcome.
- On a supine plain abdominal radiograph, portal venous gas appears as branching, linear, radiolucent vessels that may extend from the region of the main portal vein toward the periphery of both hepatic lobes, and the extent depends on the amount of portal venous gas present.
Pneumoperitoneum
- Free gas in the peritoneal cavity results from bowel perforation, which most commonly occurs in the distal ileum and proximal colon.
- It is the only universally accepted radiologic indication for surgical intervention.
- On the cross-table lateral view, free gas may appear as triangular lucencies between loops of bowel anteriorly just beneath the abdominal wall or as small bubbles or linear gas collections anterior to the liver.
- On the left lateral decubitus view, small amounts of gas may be seen between the right lobe of the liver and the right lateral abdominal wall.
- On the supine view, large amounts of gas may give rise to the football sign, where the gas outlines the whole of the peritoneal cavity, the under surface of the diaphragm, and the falciform ligament (the lacing of the football).
- Smaller amounts of free gas may give rise to lucency below the diaphragm without giving rise to the full-blown football sign.
- Even on the supine view, smaller amounts of free gas may be detected when both sides of the bowel wall are outlined (Rigler's sign).
Diagnostic Findings
Images shown below are courtesy of RadsWiki
Case # 1


Case # 2


Treatment
Treatment consists primarily of supportive care including providing bowel rest by stopping enteral feeds, gastric decompression with intermittent suction, fluid repletion to correct electrolyte abnormalities and third space losses, parenteral nutrition, and prompt antibiotic therapy. Monitoring is clinical, although serial supine and left lateral decubitus abdominal roentgenograms should be performed every 6 hours. Signs of radiographic worsening of NEC include dilated bowel loops, pneumatosis intestinalis, portal venous gas, and pneumoperitoneum. Where the disease is not halted through medical treatment alone, or when the bowel perforates, immediate emergency surgery to resect the dead bowel is required. This may require a colostomy, which may be able to be reversed at a later time. Some children may suffer later as a result of short bowel syndrome if extensive portions of the bowel had to be removed.
Prognosis
Typical recovery from NEC if medical, non-surgical treatment succeeds, includes 10-14 days or more without oral intake and then demonstrated ability to resume feedings and gain weight. Recovery from NEC alone may be compromised by co-morbid conditions that frequently accompany prematurity. Longterm complications of medical NEC include bowel obstruction and anemia. Despite a significant mortality risk, long-term prognosis for infants undergoing NEC surgery is improving, with survival rates of 70-80%. "Surgical NEC" survivors are at-risk for complications including short-bowel syndrome, and neurodevelopmental disability.
Pathological Findings
-
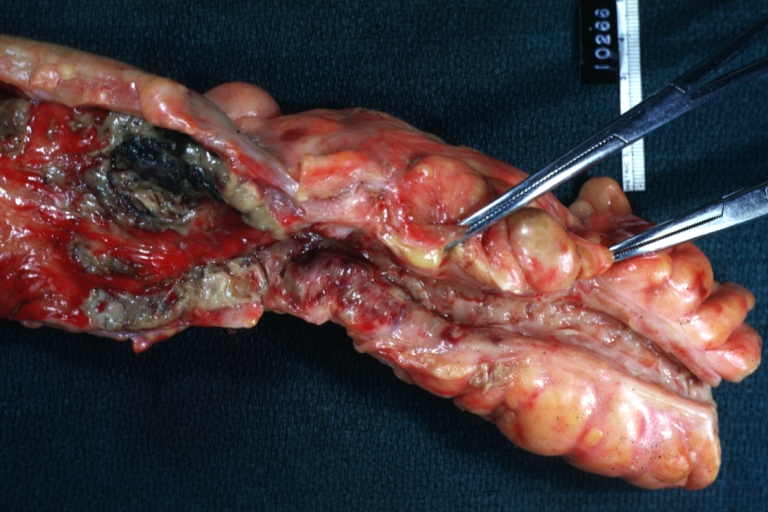 Colon: Necrotizing Enterocolitis: Gross, natural color, thickened constricted colon with linear ulcerations and mucosal hyperemia
Colon: Necrotizing Enterocolitis: Gross, natural color, thickened constricted colon with linear ulcerations and mucosal hyperemia -
 Colon: Necrotizing Enterocolitis: Gross, natural color, inflamed colon with linear ulcerations
Colon: Necrotizing Enterocolitis: Gross, natural color, inflamed colon with linear ulcerations


-
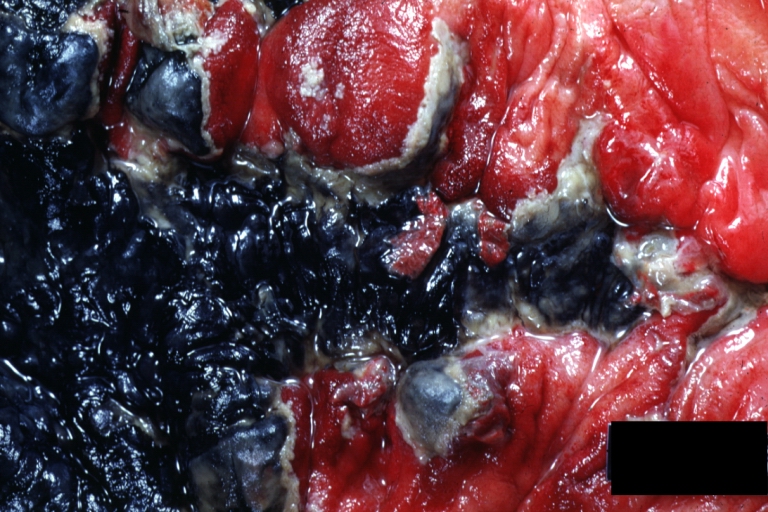
 Small intestine: Necrotizing Enterocolitis: Gross, natural color, four loops of bowel with obvious dusky cyanosis (very good example}
Small intestine: Necrotizing Enterocolitis: Gross, natural color, four loops of bowel with obvious dusky cyanosis (very good example} -
 Small intestine: Necrotizing Enterocolitis: Gross, natural color, opened body with dilated gangrenous gut
Small intestine: Necrotizing Enterocolitis: Gross, natural color, opened body with dilated gangrenous gut


References
- Monica Epelman, Alan Daneman, Oscar M. Navarro, Iris Morag, Aideen M. Moore, Jae Hong Kim, Ricardo Faingold, Glenn Taylor, and J. Ted Gerstle. Necrotizing Enterocolitis: Review of State-of-the-Art Imaging Findings with Pathologic Correlation. RadioGraphics 2007 27: 285-305.
Template:Certain conditions originating in the perinatal period