Sandbox:Bagheri2: Difference between revisions
Amir Bagheri (talk | contribs) No edit summary |
Amir Bagheri (talk | contribs) |
||
| (4 intermediate revisions by the same user not shown) | |||
| Line 7: | Line 7: | ||
== Special consideration when adding information from observational studies == | == Special consideration when adding information from observational studies == | ||
{{Infobox Nerve | | |||
Name = Optic nerve | | |||
Latin = nervus opticus | | |||
GraySubject = 197 | | |||
GrayPage = 882 | | |||
Image = Gray773.png | | |||
Caption = The left optic nerve and the [[optic tract]]s. | | |||
Image2 = Calf-Eye-Posterior-Outside-2005-Oct-13.jpg | | |||
Caption2 = Optic nerve leaving the back of a calf eye (from dissection).| | |||
Innervates = | | |||
BranchFrom = | | |||
BranchTo = | | |||
MeshName = Optic+Nerve | | |||
MeshNumber = A08.800.800.120.680 | | |||
}} | |||
== Overview == | == Overview == | ||
The '''optic nerve''', also known as '''cranial nerve II''', or simply as '''CN II''', is a paired cranial nerve that transmits visual information from the retina to the brain. In humans, the optic nerve is derived from optic stalks during the seventh week of development and is composed of retinal ganglion cell axons and glial cells; it extends from the optic disc to the optic chiasma and continues as the optic tract to the lateral geniculate nucleus, pretectal nuclei, and superior colliculus. | The '''optic nerve''', also known as '''cranial nerve II''', or simply as '''CN II''', is a paired cranial nerve that transmits visual information from the retina to the brain. In humans, the optic nerve is derived from optic stalks during the seventh week of development and is composed of retinal ganglion cell axons and glial cells; it extends from the optic disc to the optic chiasma and continues as the optic tract to the lateral geniculate nucleus, pretectal nuclei, and superior colliculus. | ||
The optic nerve has been classified as the second of twelve paired cranial nerves but it is technically part of the central nervous system, rather than the peripheral nervous system because it is derived from an out-pouching of the diencephalon (optic stalks) during embryonic development. As a consequence, the fibers of the optic nerve are covered with myelin produced by oligodendrocytes, rather than Schwann cells of the peripheral nervous system, and are encased within the meninges. Peripheral neuropathies like Guillain–Barré syndrome do not affect the optic nerve. However, most typically the optic nerve is grouped with the other eleven cranial nerves and is considered to be part of the peripheral nervous system. | The optic nerve has been classified as the second of twelve paired cranial nerves but it is technically part of the central nervous system, rather than the peripheral nervous system because it is derived from an out-pouching of the diencephalon (optic stalks) during embryonic development. As a consequence, the fibers of the optic nerve are covered with myelin produced by oligodendrocytes, rather than Schwann cells of the peripheral nervous system, and are encased within the meninges. Peripheral neuropathies like Guillain–Barré syndrome do not affect the optic nerve. However, most typically the optic nerve is grouped with the other eleven cranial nerves and is considered to be part of the peripheral nervous system. | ||
| Line 27: | Line 38: | ||
== Historical Perspective == | == Historical Perspective == | ||
*Discovery of cranial nerves started in the 2nd century by Galen, but these 12 cranial nerves that we recognize today was enumerated by Samuel Sömmerring in 1778.< | *Discovery of cranial nerves started in the 2nd century by Galen, but these 12 cranial nerves that we recognize today was enumerated by Samuel Sömmerring in 1778. | ||
<br /> | |||
== Function == | |||
The optic nerve transmits all visual information including brightness perception, color perception and contrast (visual acuity). It also conducts the visual impulses that are responsible for two important neurological reflexes: the light reflex and the accommodation reflex. The light reflex refers to the constriction of both pupils that occurs when light is shone into either eye. The accommodation reflex refers to the swelling of the lens of eye that occurs when one looks at a near object (for example, when reading the lens adjusts to near vision.<ref name="D'Antoni2015" /> | |||
The eye's blind spot is a result of the absence of photoreceptors in the area of the retina where the optic nerve leaves the eye.<ref name="D'Antoni2015" /> | |||
== physiology == | == physiology == | ||
| Line 54: | Line 72: | ||
The International Foundation for Optic Nerve Diseases IFOND sponsors research and information on a variety of optic nerve disorders and may provide general direction.<br /> | The International Foundation for Optic Nerve Diseases IFOND sponsors research and information on a variety of optic nerve disorders and may provide general direction.<br /> | ||
=== Physical Examination === | === Physical Examination === | ||
Visual fields are assessed by asking the patient to cover one eye while the examiner tests the opposite eye. The examiner wiggles the finger in each of the four quadrants and asks the patient to state when the finger is seen in the periphery. The examiner's visual fields should be normal, since it is used as the baseline. | |||
Visual acuity is tested in each eye separately. Ensure the patient's vision is corrected with eyeglasses or a pinhole. The patient is asked to read progressively smaller lines on the '''near card''' or ''Snellen chart''.<br /> | |||
<br /> | <br /> | ||
==Additional images== | |||
<gallery> | |||
Image:MRI_of_human_eye.jpg|MRI scan of human eye showing optic nerve. | |||
Image:Gray514.png|The [[ophthalmic artery]] and its branches. (optic nerve is yellow) | |||
Image:Gray567.png|Dura mater and its processes exposed by removing part of the right half of the skull, and the brain. | |||
Image:Gray569.png|Tentorium cerebelli from above. | |||
Image:Gray682.png|Superficial dissection of brain-stem. Lateral view. | |||
Image:Gray683.png|Dissection of brain-stem. Lateral view. | |||
Image:Gray715.png|Mesal aspect of a brain sectioned in the median sagittal plane. | |||
Image:Gray722.png|Scheme showing central connections of the optic nerves and optic tracts. | |||
Image:Gray748.png|The fornix and corpus callosum from below. | |||
Image:Gray776.png|Nerves of the orbit. Seen from above. | |||
Image:Gray777.png|Nerves of the orbit, and the ciliary ganglion. Side view. | |||
Image:Gray873.png|The arteries of the choroid and iris. The greater part of the sclera has been removed. | |||
Image:Gray874.png|The veins of the choroid. | |||
Image:Gray880.png|The terminal portion of the optic nerve and its entrance into the eyeball, in horizontal section. | |||
</gallery> | |||
== References == | == References == | ||
<references /> | <references /> | ||
Latest revision as of 17:14, 30 July 2020
CRANIAL NERVE II
Editor-In-Chief: C. Michael Gibson, M.S., M.D. Associate Editor(s)-in-Chief:
Synonyms and Keywords:
Special consideration when adding information from observational studies
Overview
The optic nerve, also known as cranial nerve II, or simply as CN II, is a paired cranial nerve that transmits visual information from the retina to the brain. In humans, the optic nerve is derived from optic stalks during the seventh week of development and is composed of retinal ganglion cell axons and glial cells; it extends from the optic disc to the optic chiasma and continues as the optic tract to the lateral geniculate nucleus, pretectal nuclei, and superior colliculus.
The optic nerve has been classified as the second of twelve paired cranial nerves but it is technically part of the central nervous system, rather than the peripheral nervous system because it is derived from an out-pouching of the diencephalon (optic stalks) during embryonic development. As a consequence, the fibers of the optic nerve are covered with myelin produced by oligodendrocytes, rather than Schwann cells of the peripheral nervous system, and are encased within the meninges. Peripheral neuropathies like Guillain–Barré syndrome do not affect the optic nerve. However, most typically the optic nerve is grouped with the other eleven cranial nerves and is considered to be part of the peripheral nervous system.
The optic nerve is ensheathed in all three meningeal layers (dura, arachnoid, and pia mater) rather than the epineurium, perineurium, and endoneurium found in peripheral nerves. Fiber tracts of the mammalian central nervous system have only limited regenerative capabilities compared to the peripheral nervous system. Therefore, in most mammals, optic nerve damage results in irreversible blindness. The fibers from the retina run along the optic nerve to nine primary visual nuclei in the brain, from which a major relay inputs into the primary visual cortex.
The optic nerve component lengths are 1 mm in the globe, 24 mm in the orbit, 9 mm in the optic canal, and 16 mm in the cranial space before joining the optic chiasm. There, partial decussation occurs, and about 53% of the fibers cross to form the optic tracts. Most of these fibers terminate in the lateral geniculate body.[1]
Based on this anatomy, the optic nerve may be divided in the four parts as indicated in the image at the top of this section (this view is from above as if you were looking into the orbit after the top of the skull had been removed): 1. the optic head (which is where it begins in the eyeball (globe) with fibers from the retina; 2. orbital part (which is the part within the orbit). 3. intracanicular part (which is the part within a bony canal known as the optic canal); and, 4. cranial part (the part within the cranial cavity, which ends at the optic chiasm).[2]
From the lateral geniculate body, fibers of the optic radiation pass to the visual cortex in the occipital lobe of the brain. In more specific terms, fibers carrying information from the contralateral superior visual field traverse Meyer's loop to terminate in the lingual gyrus below the calcarine fissure in the occipital lobe, and fibers carrying information from the contralateral inferior visual field terminate more superiorly, to the cuneus.
Historical Perspective
- Discovery of cranial nerves started in the 2nd century by Galen, but these 12 cranial nerves that we recognize today was enumerated by Samuel Sömmerring in 1778.
Function
The optic nerve transmits all visual information including brightness perception, color perception and contrast (visual acuity). It also conducts the visual impulses that are responsible for two important neurological reflexes: the light reflex and the accommodation reflex. The light reflex refers to the constriction of both pupils that occurs when light is shone into either eye. The accommodation reflex refers to the swelling of the lens of eye that occurs when one looks at a near object (for example, when reading the lens adjusts to near vision.[1]
The eye's blind spot is a result of the absence of photoreceptors in the area of the retina where the optic nerve leaves the eye.[1]
physiology
The optic nerve contains 1.2 million nerve fibers. This number is low compared to the roughly 100 million photoreceptors in the retina, and implies that substantial pre-processing takes place in the retina before the signals are sent to the brain through the optic nerve.
The eye's blind spot is a result of the absence of retina where the optic nerve leaves the eye. This is because there are no photoreceptors in this area.
Role in disease
Main article: List of eye diseases and disorders
Damage to the optic nerve typically causes permanent and potentially severe loss of vision, as well as an abnormal pupillary reflex, which is diagnostically important. The type of visual field loss will depend on which portions of the optic nerve were damaged. Generally speaking:
- Damage before the optic chiasm causes loss of vision in the visual field of the same side only.

Views of Paris showing vision with loss of both temporal visual fields - Damage in the chiasm causes loss of vision laterally in both visual fields (bitemporal hemianopia). It may occur in large pituitary adenomata.
- Damage after the chiasm causes loss of vision on one side but affecting both visual fields: the visual field affected is located on the opposite side of the lesion.

Injury to the optic nerve can be the result of congenital or inheritable problems like Leber's Hereditary Optic Neuropathy, glaucoma, trauma, toxicity, inflammation, ischemia, infection (very rarely), or compression from tumors or aneurysms. By far, the three most common injuries to the optic nerve are from glaucoma, optic neuritis (especially in those younger than 50 years of age) and anterior ischemic optic neuropathy (usually in those older than 50).
Glaucoma is a group of diseases involving loss of retinal ganglion cells causing optic neuropathy in a pattern of peripheral vision loss, initially sparing central vision.
Optic neuritis is inflammation of the optic nerve. It is associated with a number of diseases, most notably multiple sclerosis.
Anterior Ischemic Optic Neuropathy is a particular type of infarct that affects patients with an anatomical predisposition and cardiovascular risk factors.
Ophthalmologists, particularly those sub specialists who are neuro-ophthalmologists, are often best suited to diagnose and treat diseases of the optic nerve.
The International Foundation for Optic Nerve Diseases IFOND sponsors research and information on a variety of optic nerve disorders and may provide general direction.
Physical Examination
Visual fields are assessed by asking the patient to cover one eye while the examiner tests the opposite eye. The examiner wiggles the finger in each of the four quadrants and asks the patient to state when the finger is seen in the periphery. The examiner's visual fields should be normal, since it is used as the baseline.
Visual acuity is tested in each eye separately. Ensure the patient's vision is corrected with eyeglasses or a pinhole. The patient is asked to read progressively smaller lines on the near card or Snellen chart.
Additional images
-

MRI scan of human eye showing optic nerve.
-
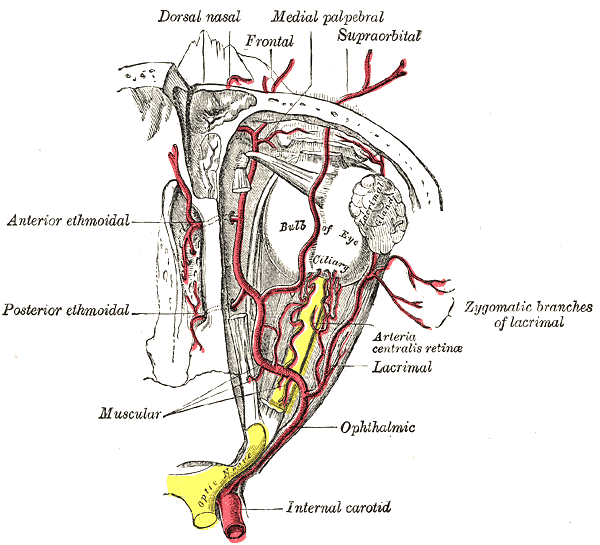
The ophthalmic artery and its branches. (optic nerve is yellow)
-
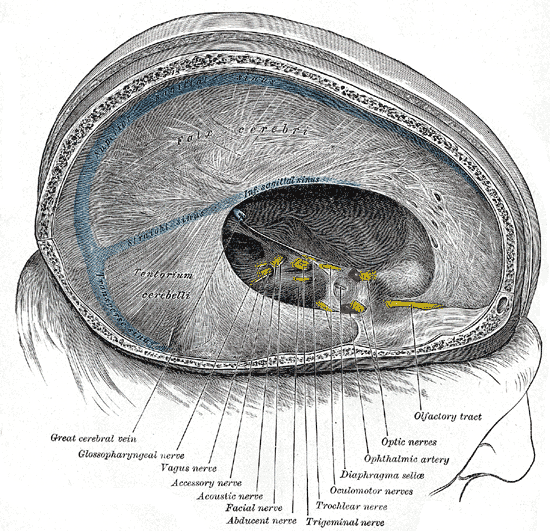
Dura mater and its processes exposed by removing part of the right half of the skull, and the brain.
-
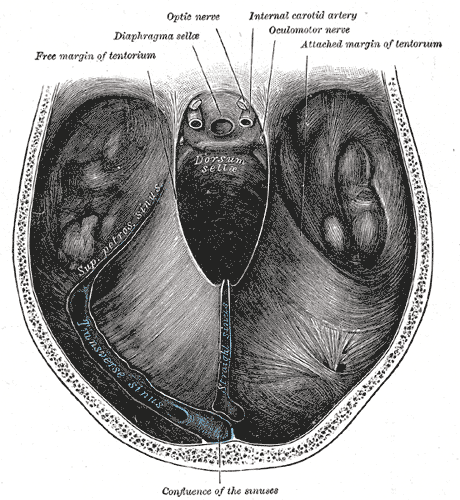
Tentorium cerebelli from above.
-
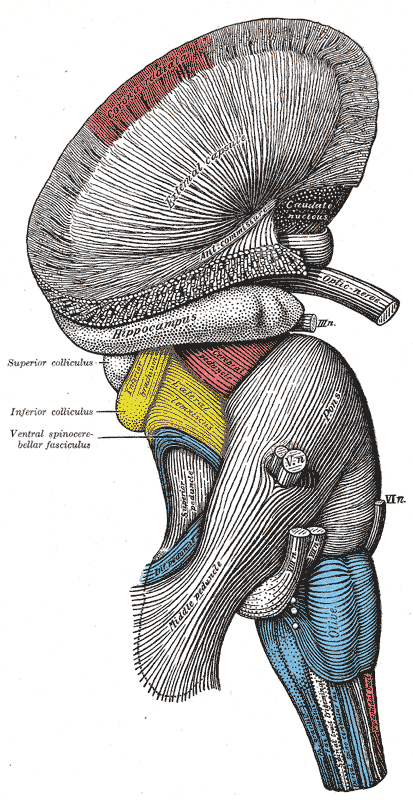
Superficial dissection of brain-stem. Lateral view.
-
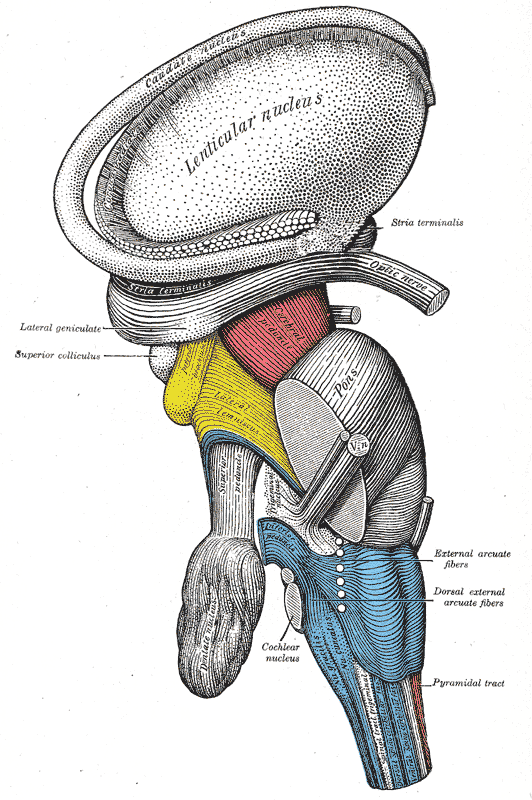
Dissection of brain-stem. Lateral view.
-
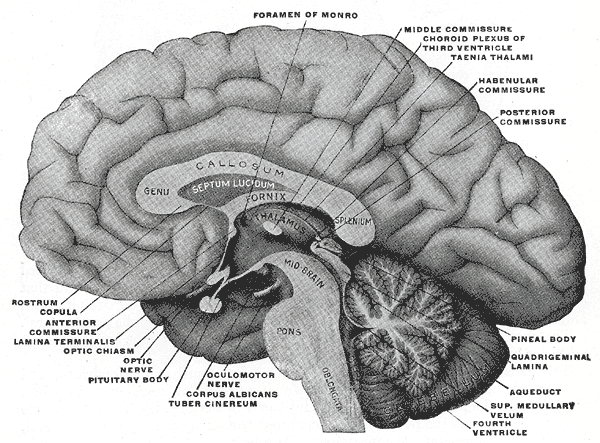
Mesal aspect of a brain sectioned in the median sagittal plane.
-
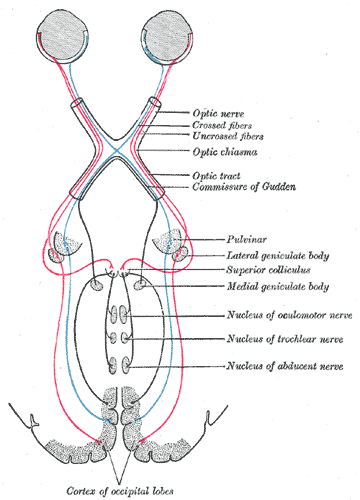
Scheme showing central connections of the optic nerves and optic tracts.
-
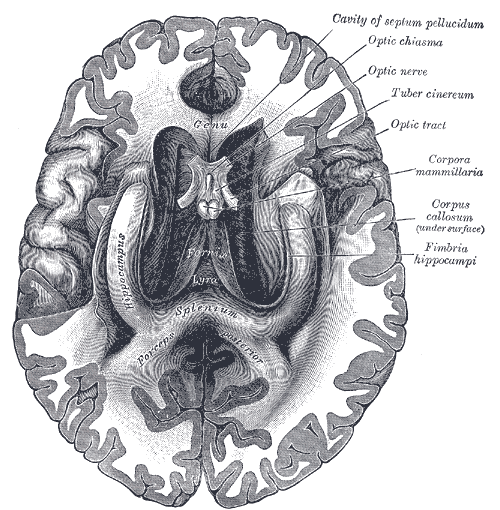
The fornix and corpus callosum from below.
-
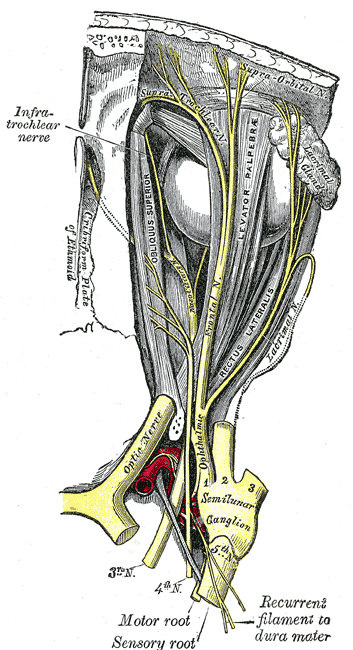
Nerves of the orbit. Seen from above.
-
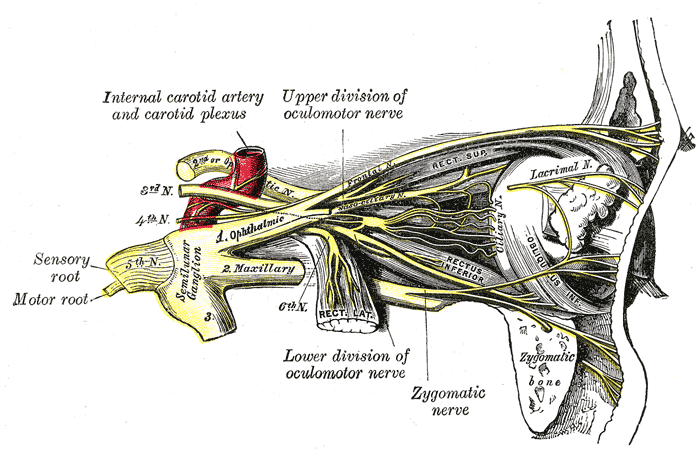
Nerves of the orbit, and the ciliary ganglion. Side view.
-
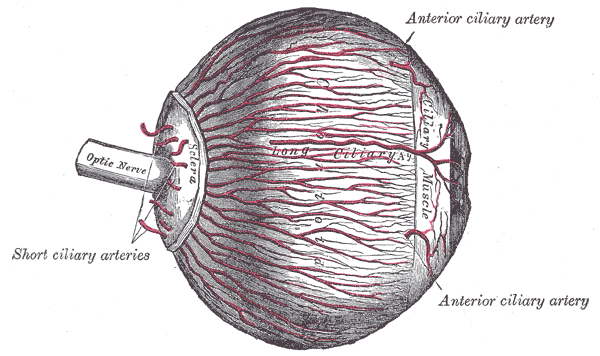
The arteries of the choroid and iris. The greater part of the sclera has been removed.
-
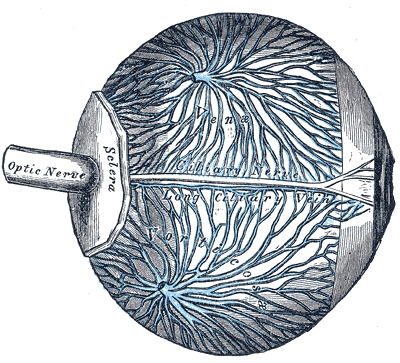
The veins of the choroid.
-
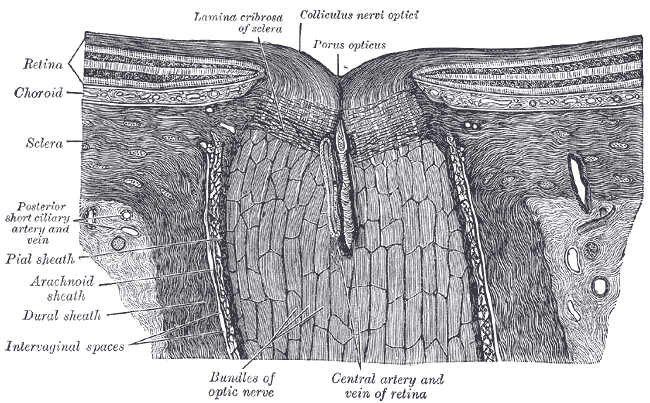
The terminal portion of the optic nerve and its entrance into the eyeball, in horizontal section.













