Wide complex tachycardias
|
Wide complex tachycardia Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Wide complex tachycardias On the Web |
|
American Roentgen Ray Society Images of Wide complex tachycardias |
|
Risk calculators and risk factors for Wide complex tachycardias |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: WCT; fast and wide; wide and fast; wide-complex tachycardia; wide complex rhythm; SVT with aberrancy; SVT with aberrant conduction; supraventricular tachycardia with aberrancy; VT versus SVT
Diagnosis
History
The patient should be asked about drugs that are associated with ventricular tachycardia and if there is a history of ischemic heart disease which would dramatically increase the odds that the rhythm is VT. Wide complex tachycardia will be due to VT in 80% of cases and will be due to VT in 98% of cases if there's a history of either acute MI or structural heart disease. Only 7% of patients with SVT will have had a prior myocardial infarction (MI). VT or an accelerated idioventricular rhythm can be seen following reperfusion in STEMI. Digoxin, antiarrhythmics, phenothiazines, TCAs, and pheochromocytoma may also cause VT. Recent procedures such as cardiac catheterization, DC countershock, repair of congenital lesions are all associated iwth VT. A family history of sudden cardiac death, a history of a channelopathy associated with arrhythmias, and the hereditary Long QT syndrome, and Brugada syndrome are all associated with VT.
Symptoms
- Shortness of breath
- Syncope
- Sudden cardiac death would suggest a diagnosis of ventricular tachycardia
Physical Examination
- Vitals should be obtained to assess hemodynamic stability and guide therapy
- Cannon-a waves are a manifestation of AV dissociation and suggest VT
- Carotid sinus massage (CSM)/Valsalva: ST can gradually slow. MAT, AT, Flutter, and AF may transiently slow. An AV nodal dependent WCT may terminate. AV dissociation may become more apparent with CSM in VT. VT can terminate with CSM
Electrocardiogram
EKG examples and diagnosis here:
- Extreme axis deviation favors VT. Especially -90 to -180 or “northwest” or “superior” axis. (23% of SVT will have SAD)
- QRS duration >140 msec favors VT (21% of VT will have QRS <140 msec)
- AV dissociation is demonstrated in only 21% of VT
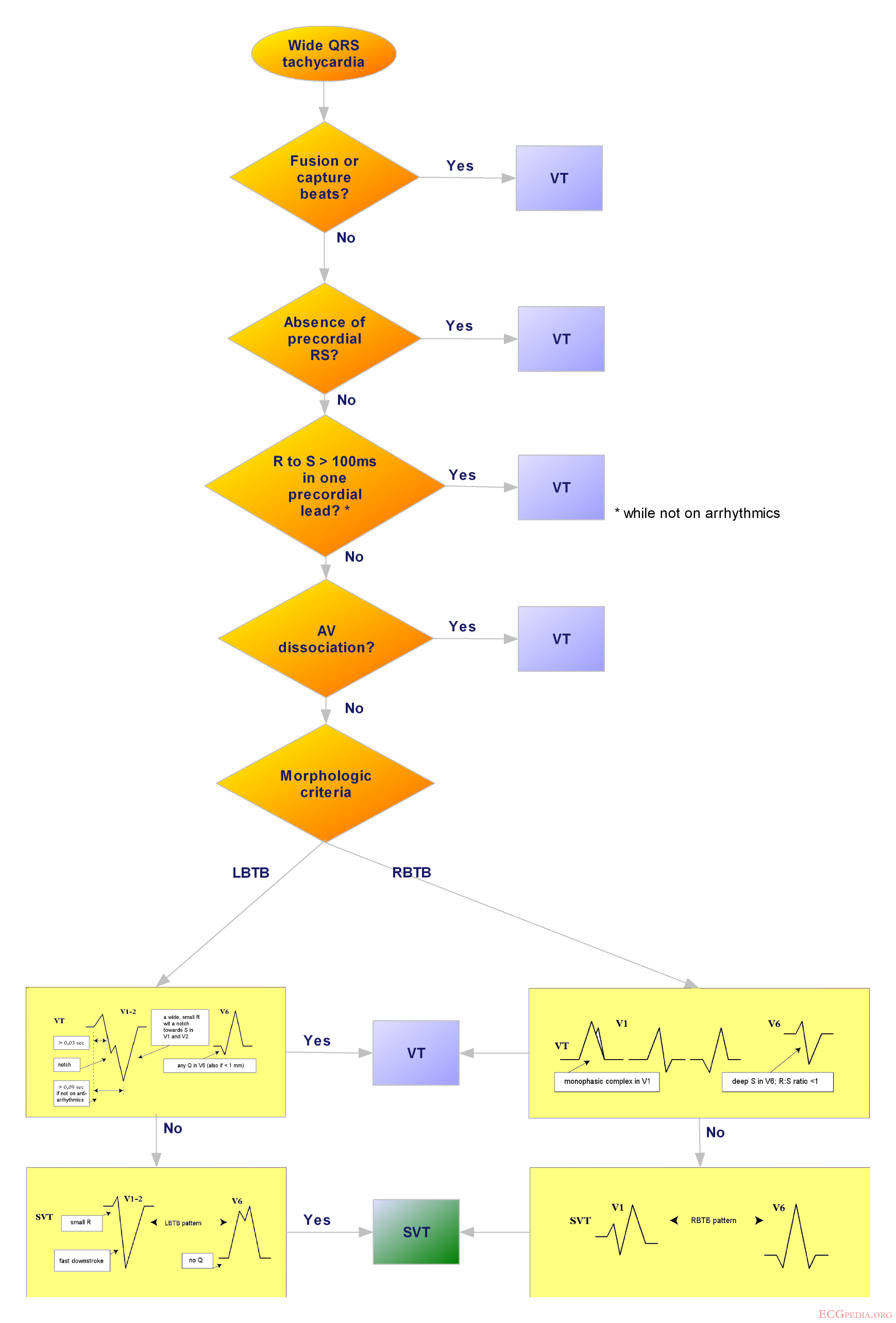
- Morphologic Criteria
- 4% of SVT and 6% of VT did not fulfill criteria in any lead
- 40% will have discordance between V1/V2 and V5/V6. One lead may suggest VT while another suggests SVT.
- An algorithmic approach was proposed by Brugada in 1991. It has a reported sensitivity of 99% and specificity of 97%.
| example | regularity | atrial frequency | ventricular frequency | origin (SVT/VT) | p-wave | effect of adenosine | |
|---|---|---|---|---|---|---|---|
| Wide complex (QRS>0.12) | |||||||
| Ventricular Tachycardia | regular (mostly) | 60-100 bpm | 110-250 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | |
| Ventricular Fibrillation | irregular | 60-100 bpm | 400-600 bpm | ventricle (VT) | AV-dissociation | none | |
| Ventricular Flutter | regular | 60-100 bpm | 150-300 bpm | ventricle (VT) | AV-dissociation | none | |
| Accelerated Idioventricular Rhythm | regular (mostly) | 60-100 bpm | 50-110 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | |
| Torsade de Pointes | regular | 150-300 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | ||
| Bundle-branch re-entrant tachycardia* | regular | 60-100 bpm | 150-300 bpm | ventricles (VT) | AV-dissociation | no rate reduction | |
| * Bundle-branch re-entrant tachycardia is extremely rare | |||||||
{kind=link}
Treatment
Defibrillation
Indications for defibrillation include the following:
- Chest pain
- Congestive heart failure (CHF)
- Hypotension with symptoms
- Loss of consciousness
- Seizure
Acute Pharmacotherapies
- If stable: (More patients than you think)
- DO NOT USE Ca2+ Channel blocker, Digoxin or Adenosine if you don't not know the etiology of the Wide Complex Tachycardia. Ca2+ Channel blockers and Digoxin can lead to accelerated conduction down a bypass tract and VF.
- Though ACLS guidelines recommend a diagnostic trial of Adenosine, it can precipitate VF in some patients with SVT. Patients who have underlying coronary disease may become ischemic from coronary steal. Rhythm can degenerate and lead to VF that cannot be resuscitated. Furthermore, some VT (esp those with structurally normal hearts) are adenosine responsive and can terminate.
- Etiology Uncertain
- Pronestyl 15mg/kg load over 30 minutes then 2-6mg/min gtt
- Ventricular Tachycardia with active ischemia
- Lidocaine 1 mg/kg q5-10 min up to 3 times then 2-6mg.min gtt
- If unsuccessful, Pronestyl as above
- If unsuccessful, IV Amiodarone 150-300 load over 15-20min. 30-60mg/hr gtt for total of 1gram
- Ventricular Tachycardia in Setting of Cardiomyopathy
- Positively SVT with aberrancy
- Antidromic AVRT
- Etiology Uncertain
Sources
Copyleft images obtained courtesy of ECGpedia, http://en.ecgpedia.org/index.php?title=Special:NewFiles&offset=&limit=500