Wide QRS complex tachycardias: Difference between revisions
Jump to navigation
Jump to search
m (Robot: Automated text replacement (-{{SIB}} +, -{{EH}} +, -{{EJ}} +, -{{Editor Help}} +, -{{Editor Join}} +)) |
m (Robot: Automated text replacement (-{{reflist}} +{{reflist|2}}, -<references /> +{{reflist|2}}, -{{WikiDoc Cardiology Network Infobox}} +)) |
||
| Line 1: | Line 1: | ||
{{SI}} | {{SI}} | ||
{{CMG}} | {{CMG}} | ||
__NOEDITSECTION__ | __NOEDITSECTION__ | ||
Revision as of 15:58, 6 September 2012
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief Jiwon Kim
Differential Diagnosis of Tachycardia with Wide QRS Complex
- A regular tachycardia with a rate of 120 to 200 BPM with a QRS duration of .12 seconds or longer may be due to:
- Paroxysmal VT
- Supraventricular tachycardia with abnormally wide QRS
- Sinus tachycardia
- SA nodal reentrant tachycardia
- Paroxysmal atrial tachycardia
- Intraatrial reentrant tachycardia
- Atrial flutter with 2:1 conduction and occasional 1:1 conduction
- AV nodal reentrant tachycardia
- Automatic junctional tachycardia
- AV reentrant tachycardia using a bypass tract
Differential Diagnosis of Wide QRS Complexes
- Aberrant ventricular conduction
- Preexisting left or right bundle branch block
- Preexisting nonspecific IVCD
- Antegrade conduction through the bypass tract in patients with WPW
Clues to the Diagnosis of VT
- Morphology of Premature Beats During Sinus Rhythm:
- Previous EKG may show preexisting IVCD.
- If PVCs are present, and if the morphology of the arrhythmia is the same, then it is likely to be ventricular in origin.
- If there are PACs with aberrant conduction, then the origin of the arrhythmia may be supraventricular.
- Onset of the Tachycardia:
- Diagnosis of SVT made if the episode is initiated by a premature P wave.
- If the paroxysm begins with a QRS then the tachycardia may be either ventricular or junctional in origin.
- If the first QRS of the tachycardia is preceded by a sinus p wave with a PR interval shorter than that of the conducted sinus beats, the tachycardia is ventricular.
- AV Dissociation:
- Although is highly suggestive of VT, it may also be seen in junctional tachycardias with retrograde block.
- Morphology of the QRS Complexes and QRS Axis:
- 80 to 85% of aberrant beats have a RBBB pattern, but ectopic beats that arise from the LV have a similar morphology.
- The finding of a positive or negative QRS complex in all precordial leads is in favor of ventricular ectopy.
- A QRS duration of > .14 seconds (A Wellens criterion)
- Left axis deviation (A Wellens criterion)
- A monophasic or biphasic RBBB QRS complex in V1. But none of their patients with SVT had a preexisting RBBB. Therefore, this finding is of limited importance. (A Wellens criterion)
- Akhtar studied 150 patients with a wide complex tachycardia. The following were helpful in the diagnosis of VT:
- all patients with VT had a QRS duration > 120 msecond.
- QRS > .14 with a RBBB, QRS > .16 with LBBB.
- V1 - V6 all show a positive deflection.
- QRS axis between -90 and + 180 degrees.
- The QRS complexes have a LBBB but the QRS axis is rightward.
- In patients with preexisting bundle branch block, there is a change in the QRS pattern during the tachycardia.
- Capture beats:
- Rare, but one of the strongest pieces of evidence in favor of VT.
- Aberrancy rarely follows a beat of such short cycle length.
- Fusion beats:
- Rare but also strongly suggests VT.
- Vagal Stimulation:
- VT is not affected by vagal stimulation.
- May terminate reentrant arrhythmias
- Atrial pacing:
- A pacing wire is placed in the RA and the atrium is stimulated at a rate faster than the tachycardia.
- If ventricular capture occurs and the QRS is normal in duration, then one can exclude the possibility of aberrant conduction.
- His bundle recording:
- In SVT, each QRS is preceded by a His bundle potential.
- In VT there is no preceding His deflection.
- The retrograde His deflection is usually obscured by the much larger QRS complex.
| example | regularity | atrial frequency | ventricular frequency | origin (SVT/VT) | p-wave | effect of adenosine | |
|---|---|---|---|---|---|---|---|
| Wide complex (QRS>0.12) | |||||||
| Ventricular Tachycardia | regular (mostly) | 60-100 bpm | 110-250 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | |
| Ventricular Fibrillation | irregular | 60-100 bpm | 400-600 bpm | ventricle (VT) | AV-dissociation | none | |
| Ventricular Flutter | regular | 60-100 bpm | 150-300 bpm | ventricle (VT) | AV-dissociation | none | |
| Accelerated Idioventricular Rhythm | regular (mostly) | 60-100 bpm | 50-110 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | |
| Torsade de Pointes | regular | 150-300 bpm | ventricle (VT) | AV-dissociation | no rate reduction (sometimes accelerates) | ||
| Bundle-branch re-entrant tachycardia* | regular | 60-100 bpm | 150-300 bpm | ventricles (VT) | AV-dissociation | no rate reduction | |
| *) Bundle-branch re-entrant tachycardia is extremely rare | |||||||
{kind=link}
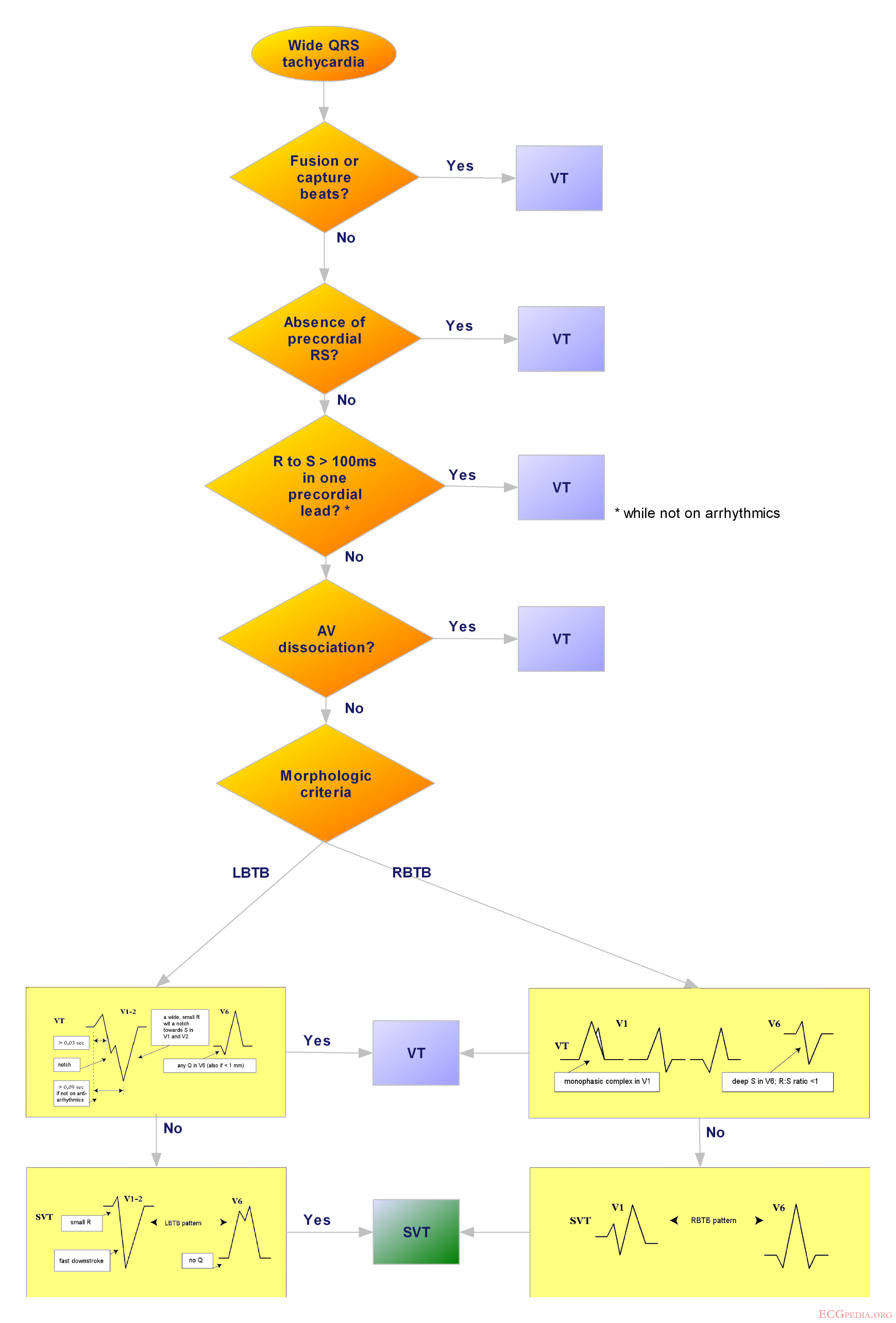
Differential Diagnosis of Wide QRS Complex Tachycardia
- The following favor the diagnosis of VT:
- AV dissociation
- RBBB with QRS > .14, or LBBB with QRS > .16
- QRS axis in RUQ between -90 and +180 degrees
- Positive QRS in all the precordial leads (V1-V6)
- LBBB with a rightward axis
- LBBB with the following QRS morphology
- R wave in V1 or V2 > 0.03 second
- any Q wave in V6
- Onset of the QRS to nadir of the S wave in V1 > 0.06 seconds
- Notching of the S wave in V1 or V2
- Capture beats, fusion beats
- QRS morphology identical to that of premature ventricular beats during sinus rhythm
Clinical Correlation
- Most patients with VT have organic heart disease.
- Post MI VT is associated with a doubling of the risk of death.
- This was an a risk factor independent of poor LV function.
- VT can be seen with reperfusion, but an accelerated idioventricular rhythm is more common.
- Digoxin intoxication is a common cause. Other antiarrhythmics, phenothiazines, TCAs, and pheochromocytoma may also cause this.
- Cardiac catheterization, DC countershock, following repair of congenital lesions, and the hereditary QT prolongation are all associated with VT.