Theophylline
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Theophylline is a anti-asthmatic that is FDA approved for the treatment of is indicated for the treatment of the symptoms and reversible airflow obstruction associated with chronic asthma and other chronic lung diseases, e.g., emphysema and chronic bronchitis.. Common adverse reactions include vomiting, diarrhea, abdominal pain, hematemesis, acid-base disturbances, rhabdomyolysis, supraventricular tachycardia, shock, nervousness, tremors, disorientation and seziures..
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
General Considerations
- The steady-state peak serum theophylline concentration is a function of the dose, the dosing interval, and the rate of theophylline absorption and clearance in the individual patient.
- Because of marked individual differences in the rate of theophylline clearance, the dose required to achieve a peak serum theophylline concentration in the 10-20 mcg/mL range varies fourfold among otherwise similar patients in the absence of factors known to alter theophylline clearance (e.g., 400-1600 mg/day in adults <60 years old and 10-36 mg/kg/day in children 1-9 years old).
- For a given population there is no single theophylline dose that will provide both safe and effective serum concentrations for all patients.
- Administration of the median theophylline dose required to achieve a therapeutic serum theophylline concentration in a given population may result in either sub-therapeutic or potentially toxic serum theophylline concentrations in individual patients.
- For example, at a dose of 900 mg/d in adults <60 years or 22 mg/kg/d in children 1-9 years, the steady state peak serum theophylline concentration will be <10 mcg/mL in about 30% of patients, 10-20 mcg/mL in about 50% and 20-30 mcg/mL in about 20% of patients.
- The dose of theophylline must be individualized on the basis of peak serum theophylline concentration measurements in order to achieve a dose that will provide maximum potential benefit with minimal risk to adverse effects.
- Transient caffeine-like adverse effects and excessive serum concentrations in slow metabolizers can be avoided in most patients by starting with a sufficiently low dose and slowly increasing the dose, if judged to be clinically indicated, in small increments (See Table V).
- Dose increases should only be made if the previous dosage is well tolerated and at intervals of no less than 3 days to allow serum theophylline concentrations to reach the new steady state. Dosage adjustment should be guided by serum theophylline concentration measurement.
- Health care providers should instruct patients and care givers to discontinue any dosage that causes adverse effects, to withhold the medication until these symptoms are gone and to then resume therapy at a lower, previously tolerated dosage.
- If the patient’s symptoms are well controlled, there are no apparent adverse effects, and no intervening factors that might alter dosage requirements , serum theophylline concentrations should be monitored at 6 month intervals for rapidly growing children and at yearly intervals for all others.
- In acutely ill patients, serum theophylline concentrations should be monitored at frequent intervals, e.g., every 24 hours.
- Theophylline distributes poorly into body fat, therefore, mg/kg dose should be calculated on the basis of ideal body weight.
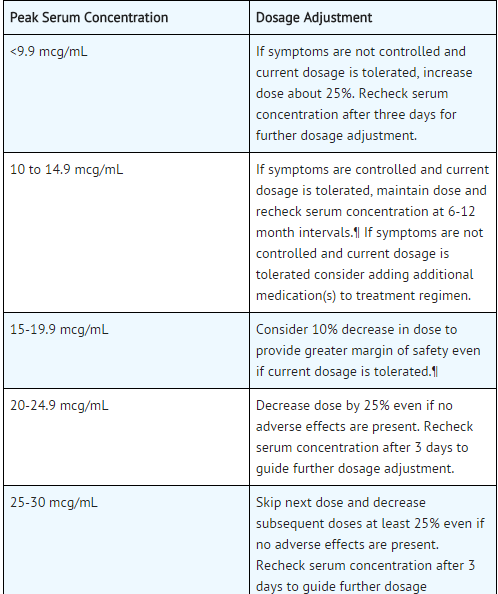
- Table V contains theophylline dosing titration schema recommended for patients in various age groups and clinical circumstances. Table VI contains recommendations for theophylline dosage adjustment based upon serum theophylline concentrations.
- Application of these general dosing recommendations to individual patients must take into account the unique clinical characteristics of each patient.
- In general, these recommendations should serve as the upper limit for dosage adjustments in order to decrease the risk of potentially serious adverse events associated with unexpected large increases in serum theophylline concentration.
Infants <1 year old
Initial Dosage
- Premature Neonates
- < 24 days postnatal age; 1.0 mg/kg every 12 hr
- >24 days postnatal age; 1.5 mg/kg every 12 hr
- Full term infants and infants up to 52 weeks of age:
- Total daily dose (mg) = [(0.2 x age in weeks)+5.0] x (Kg body Wt).
- Up to age 26 weeks; divide dose into 3 equal amounts administered at 8 hour intervals.
- >26 weeks of age; divide dose into 4 equal amounts administered at 6 hour intervals.
- Final Dosage.
- Adjusted to maintain a peak steady state serum theophylline concentration of 5-10 mcg/ml in neonates and 10-15 mcg/mL in older infants (see Table VI). :* Since the time required to reach steady-state is a function of theophylline half-life, up to 5 days may be required to achieve steady state in a premature neonate while only 2-3 days may be required in a 6 month old infant without other risk factors for impaired clearance in the absence of a loading dose.
- If a serum theophylline concentration is obtained before steady state is achieved, the maintenance dose should not be increased, even if the serum theophylline concentration is <10 mcg/mL.
This image is provided by the National Library of Medicine.

Patients With Risk Factors For Impaired Clearance, The Elderly (>60 Years), And Those In Whom It Is Not Feasible To Monitor Serum Theophylline Concentrations
- In children 1-15 years of age, the final theophylline dose should not exceed 16 mg/kg/day up to a maximum of 400 mg/day in the presence of risk factors for reduced theophylline clearance (see WARNINGS) or if it is not feasible to monitor serum theophylline concentrations.
- In adolescents ≥16 years and adults, including the elderly, the final theophylline dose should not exceed 400 mg/day in the presence of risk factors for reduced theophylline clearance (see WARNINGS) or if it is not feasible to monitor serum theophylline concentrations.
Loading Dose for Acute Bronchodilatation
- An inhaled beta-2 selective agonist, alone or in combination with a systemically administered corticosteroid, is the most effective treatment for acute exacerbations of reversible airways obstruction.
- Theophylline is a relatively weak bronchodilator, is less effective than an inhaled beta-2 selective agonist and provides no added benefit in the treatment of acute bronchospasm.
- If an inhaled or parenteral beta agonist is not available, a loading dose of an oral immediate release theophylline can be used as a temporary measure. * A single 5 mg/kg dose of theophylline, in a patient who has not received any theophylline in the previous 24 hours, will produce an average peak serum theophylline concentration of 10 mcg/mL (range 5-15 mcg/mL).
- If dosing with theophylline is to be continued beyond the loading dose, the guidelines in Sections A.1.b., B.3, or C., above, should be utilized and serum theophylline concentration monitored at 24 hour intervals to adjust final dosage.
- Patients with more rapid metabolism, clinically identified by higher than average dose requirements, should receive a smaller dose more frequently to prevent breakthrough symptoms resulting from low trough concentrations before the next dose.
- A reliably absorbed slow-release formulation will decrease fluctuations and permit longer dosing intervals.
This image is provided by the National Library of Medicine. 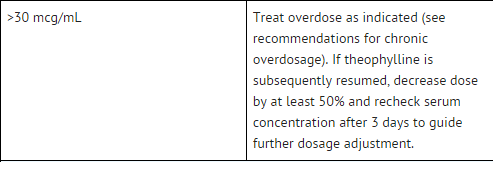
This image is provided by the National Library of Medicine.


Off-Label Use and Dosage (Adult)
Guideline-Supported Use
Condition1
- Developed by:
- Class of Recommendation:
- Strength of Evidence:
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Theophylline in adult patients.
Non–Guideline-Supported Use
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Theophylline in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding FDA-Labeled Use of Theophylline in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
Condition1
- Developed by:
- Class of Recommendation:
- Strength of Evidence:
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Theophylline in pediatric patients.
Non–Guideline-Supported Use
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Theophylline in pediatric patients.
Contraindications
- ELIXOPHYLLIN Elixir is contraindicated in patients with a history of hypersensitivity to theophylline or other components in the product.
Warnings
Concurrent Illness
- Theophylline should be used with extreme caution in patients with the following clinical conditions due to the increased risk of exacerbation of the concurrent condition:
- Active peptic ulcer disease
- Seizure disorders
- Cardiac arrhythmias (not including bradyarrhythmias)
- Conditions That Reduce Theophylline Clearance:
- Age
- Neonates (term and premature)
- Children <1 year
- Elderly (>60 years)
- Concurrent Diseases
- Acute pulmonary edema
- Congestive heart failure
- Cor pulmonale
- Fever; ≥102oF for 24 hours or more; or lesser temperature elevations for longer periods
- Hypothyroidism
- Liver disease; cirrhosis, acute hepatitis
- Reduced renal function in infants <3 months of age
- Sepsis with multi-organ failure
- Shock
- Cessation of Smoking
- Drug Interactions Adding a drug that inhibits theophylline metabolism (e.g., cimetidine, erythromycin, tacrine) or stopping a concurrently administered drug that enhances theophylline metabolism (e.g., carbamazepine, rifampin).
When Signs or Symptoms of Theophylline Toxicity Are Present
- Whenever a patient receiving theophylline develops nausea or vomiting, particularly repetitive vomiting, or other signs or symptoms consistent with theophylline toxicity (even if another cause may be suspected), additional doses of theophylline should be withheld and a serum theophylline concentration measured immediately.
- Patients should be instructed not to continue any dosage that causes adverse effects and to withhold subsequent doses until the symptoms have resolved, at which time the clinician may instruct the patient to resume the drug at a lower dosage
Dosage Increases
- Increases in the dose of theophylline should not be made in response to an acute exacerbation of symptoms of chronic lung disease since theophylline provides little added benefit to inhaled beta2-selective agonists and systemically administered corticosteroids in this circumstance and increases the risk of adverse effects.
- A peak steady state serum theophylline concentration should be measured before increasing the dose in response to persistent chronic symptoms to ascertain whether an increase in dose is safe.
- Before increasing the theophylline dose on the basis of a low serum concentration, the clinician should consider whether the blood sample was obtained at an appropriate time in relationship to the dose and whether the patient has adhered to the prescribed regimen.
- As the rate of theophylline clearance may be dose-dependent (i.e., steady-state serum concentrations may increase disproportionately to the increase in dose), an increase in dose based upon a sub-therapeutic serum concentration measurement should be conservative.
- In general, limiting dose increases to about 25% of the previous total daily dose will reduce the risk of unintended excessive increases in serum theophylline concentration.
Adverse Reactions
Clinical Trials Experience
- Adverse reactions associated with theophylline are generally mild when peak serum theophylline concentrations are <20 mcg/mL and mainly consist of transient caffeine-like adverse effects such as nausea, vomiting, headache, and insomnia.
- When peak serum theophylline concentrations exceed 20 mcg/mL, however, theophylline produces a wide range of adverse reactions including persistent vomiting, cardiac arrhythmias, and intractable seizures which can be lethal. * The transient caffeine-like adverse reactions occur in about 50% of patients when theophylline therapy is initiated at doses higher than recommended initial doses (e.g., >300 mg/day in adults and >12 mg/kg/day in children beyond >1 year of age).
- During the initiation of theophylline therapy, caffeine-like adverse effects may transiently alter patient behavior, especially in school age children, but this response rarely persists.
- Initiation of theophylline therapy at a low dose with subsequent slow titration to a predetermined age-related maximum dose will significantly reduce the frequency of these transient adverse effects (see DOSAGE AND ADMINISTRATION , TABLE V).
- In a small percentage of patients (<3% of children and <10% of adults) the caffeine-like adverse effects persist during maintenance therapy, even at peak serum theophylline concentrations within the therapeutic range (i.e., 10-20 mcg/mL).
- Dosage reduction may alleviate the caffeine-like adverse effects in these patients, however, persistent adverse effects should result in a reevaluation of the need for continued theophylline therapy and the potential therapeutic benefit of alternative treatment.
- Other adverse reactions that have been reported at serum theophylline concentrations <20 mcg/mL include diarrhea, irritability, restlessness, fine skeletal muscle tremors, and transient diuresis.
- In patients with hypoxia secondary to COPD, multifocal atrial tachycardia and flutter have been reported at serum theophylline concentrations ≥15 mcg/mL.
- There have been a few isolated reports of seizures at serum theophylline concentrations <20 mcg/mL in patients with an underlying neurological disease or in elderly patients.
- The occurrence of seizures in elderly patients with serum theophylline concentrations <20 mcg/mL may be secondary to decreased protein binding resulting in a larger proportion of the total serum theophylline concentration in the pharmacologically active unbound form.
- The clinical characteristics of the seizures reported in patients with serum theophylline concentrations <20 mcg/mL have generally been milder than seizures associated with excessive serum theophylline concentrations resulting from an overdose (i.e., they have generally been transient, often stopped without anticonvulsant therapy, and did not result in neurological residua).
This image is provided by the National Library of Medicine. 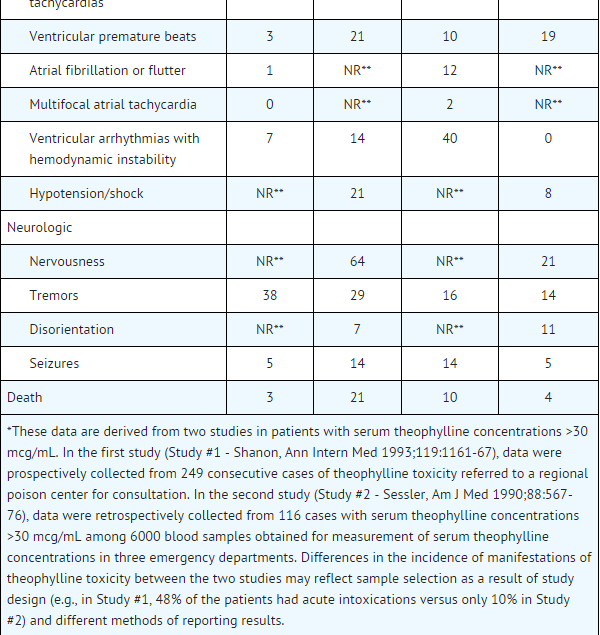
This image is provided by the National Library of Medicine.


Cardiovascular
Digestive
Endocrine
Hematologic and Lymphatic
Metabolic and Nutritional
Musculoskeletal
Neurologic
Respiratory
Skin and Hypersensitivy Reactions
Special Senses
Urogenital
Miscellaneous
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Theophylline in the drug label.
Body as a Whole
Cardiovascular
Digestive
Endocrine
Hematologic and Lymphatic
Metabolic and Nutritional
Musculoskeletal
Neurologic
Respiratory
Skin and Hypersensitivy Reactions
Special Senses
Urogenital
Miscellaneous
Drug Interactions
- Drug
- Description
Use in Specific Populations
Pregnancy
- Pregnancy Category
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Theophylline in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Theophylline during labor and delivery.
Nursing Mothers
There is no FDA guidance on the use of Theophylline with respect to nursing mothers.
Pediatric Use
There is no FDA guidance on the use of Theophylline with respect to pediatric patients.
Geriatic Use
There is no FDA guidance on the use of Theophylline with respect to geriatric patients.
Gender
There is no FDA guidance on the use of Theophylline with respect to specific gender populations.
Race
There is no FDA guidance on the use of Theophylline with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Theophylline in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Theophylline in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Theophylline in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Theophylline in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
Monitoring
There is limited information regarding Monitoring of Theophylline in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Theophylline in the drug label.
Overdosage
General
- The chronicity and pattern of theophylline overdosage significantly influences clinical manifestations of toxicity, management and outcome.
- There are two common presentations: (1) acute overdose, i.e., ingestion of a single large excessive dose (>10 mg/kg) as occurs in the context of an attempted suicide or isolated medication error, and (2) chronic overdosage, i.e., ingestion of repeated doses that are excessive for the patient’s rate of theophylline clearance. The most common causes of chronic theophylline overdosage include patient or care giver error in dosing, clinician prescribing of an excessive dose or a normal dose in the presence of factors known to decrease the rate of theophylline clearance, and increasing the dose in response to an exacerbation of symptoms without first measuring the serum theophylline concentration to determine whether a dose increase is safe.
- Severe toxicity from theophylline overdose is a relatively rare event. In one health maintenance organization, the frequency of hospital admissions for chronic overdosage of theophylline was about 1 per 1000 person-years exposure.
- In another study, among 6000 blood samples obtained for measurement of serum theophylline concentration, for any reason, from patients treated in an emergency department, 7% were in the 20-30 mcg/mL range and 3% were >30 mcg/mL.
- Approximately two-thirds of the patients with serum theophylline concentrations in the 20-30 mcg/mL range had one or more manifestations of toxicity while >90% of patients with serum theophylline concentrations >30mcg/mL were clinically intoxicated.
- Similarly, in other reports, serious toxicity from theophylline is seen principally at serum concentrations >30 mcg/mL.
- Several studies have described the clinical manifestations of theophylline overdose and attempted to determine the factors that predict life-threatening toxicity.
- In general, patients who experience an acute overdose are less likely to experience seizures than patients who have experienced a chronic overdosage, unless the peak serum theophylline concentration is >100 mcg/mL.
- After a chronic overdosage, generalized seizures, life-threatening cardiac arrhythmias, and death may occur at serum theophylline concentrations >30 mcg/mL.
- The severity of toxicity after chronic overdosage is more strongly correlated with the patient’s age than the peak serum theophylline concentration; patients >60 years are at the greatest risk for severe toxicity and mortality after a chronic overdosage.
- Pre-existing or concurrent disease may also significantly increase the susceptibility of a patient to a particular toxic manifestation, e.g., patients with neurologic disorders have an increased risk of seizures and patients with cardiac disease have an increased risk of cardiac arrhythmias for a given serum theophylline concentration compared to patients without the underlying disease.
- The frequency of various reported manifestations of theophylline overdose according to the mode of overdose are listed in Table IV.
- Other manifestations of theophylline toxicity include increases in serum calcium, creatine kinase, myoglobin and leukocyte count, decreases in serum phosphate and magnesium, acute myocardial infarction, and urinary retention in men with obstructive uropathy.
- Seizures associated with serum theophylline concentrations >30 mcg/mL are often resistant to anticonvulsant therapy and may result in irreversible brain injury if not rapidly controlled.
- Death from theophylline toxicity is most often secondary to cardiorespiratory arrest and/or hypoxic encephalopathy following prolonged generalized seizures or intractable cardiac arrhythmias causing hemodynamic compromise.
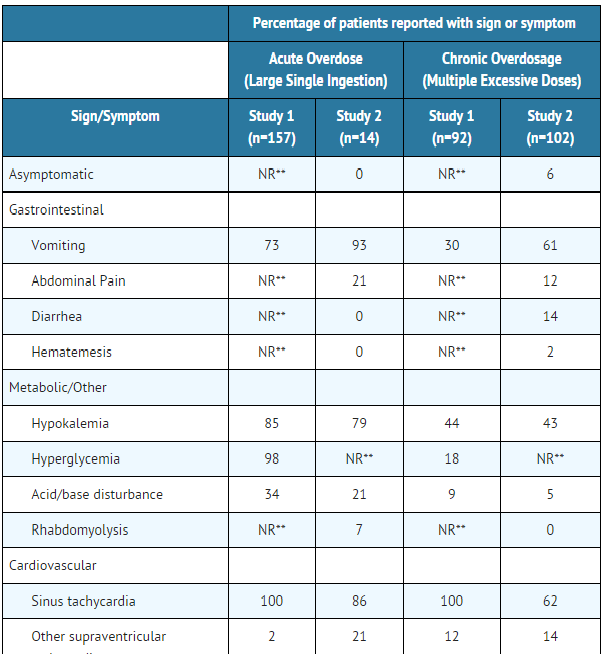
Overdose Management
- General Recommendations for Patients with Symptoms of Theophylline Overdose or Serum Theophylline Concentrations >30 mcg/mL (Note: Serum theophylline concentrations may continue to increase after presentation of the patient for medical care.)
- While simultaneously instituting treatment, contact a regional poison center to obtain updated information and advice on individualizing the recommendations that follow.
- Institute supportive care, including establishment of intravenous access, maintenance of the airway, and electrocardiographic monitoring.
- Treatment of seizures Because of the high morbidity and mortality associated with theophylline-induced seizures, treatment should be rapid and aggressive.
- Anticonvulsant therapy should be initiated with an intravenous benzodiazepine, e.g., diazepam, in increments of 0.1-0.2 mg/kg every 1-3 minutes until seizures are terminated. Repetitive seizures should be treated with a loading dose of phenobarbital (20 mg/kg infused over 30- 60 minutes). * Case reports of theophylline overdose in humans and animal studies suggest that phenytoin is ineffective in terminating theophylline-induced seizures.
- The doses of benzodiazepines and phenobarbital required to terminate theophylline-induced seizures are close to the doses that may cause severe respiratory depression or respiratory arrest; the clinician should therefore be prepared to provide assisted ventilation.
- Elderly patients and patients with COPD may be more susceptible to the respiratory depressant effects of anticonvulsants.
- Barbiturate-induced coma or administration of general anesthesia may be required to terminate repetitive seizures or status epilepticus. General anesthesia should be used with caution in patients with theophylline overdose because fluorinated volatile anesthetics may sensitize the myocardium to endogenous catecholamines released by theophylline.
- Enflurane appears to less likely to be associated with this effect than halothane and may, therefore, be safer.
- Neuromuscular blocking agents alone should not be used to terminate seizures since they abolish the musculoskeletal manifestations without terminating seizure activity in the brain.
- Anticipate Need for Anticonvulsants In patients with theophylline overdose who are at high risk for theophylline induced seizures, e.g., patients with acute overdoses and serum theophylline concentrations >100 mcg/mL chronic overdosage in patients >60 years of age with serum theophylline concentrations >30 mcg/mL, the need for anticonvulsant therapy should be anticipated.
- A benzodiazepine such as diazepam should be drawn into a syringe and kept at the patient’s bedside and medical personnel qualified to treat seizures should be immediately available.
- In selected patients at high risk for theophylline-induced seizures, consideration should be given to the administration of prophylactic anticonvulsant therapy.
- Situations where prophylactic anticonvulsant therapy should be considered in high risk patients include anticipated delays in instituting methods for extracorporeal removal of theophylline (e.g., transfer of a high risk patient from one health care facility to another for extracorporeal removal) and clinical circumstances that significantly interfere with efforts to enhance theophylline clearance (e.g., a neonate where dialysis may not be technically feasible or a patient with vomiting unresponsive to antiemetics who is unable to tolerate multiple-dose oral activated charcoal).
- In animal studies, prophylactic administration of phenobarbital, but not phenytoin, has been shown to delay the onset of theophylline induced generalized seizures and to increase the dose of theophylline required to induce seizures (i.e., markedly increases the LD50).
- Although there are no controlled studies in humans, a loading dose of intravenous phenobarbital (20 mg/kg infused over 60 minutes) may delay or prevent life-threatening seizures in high risk patients while efforts to enhance theophylline clearance are continued.
- Phenobarbital may cause respiratory depression, particularly in elderly patients and patients with COPD.
- Treatment of cardiac arrhythmias Sinus tachycardia and simple ventricular premature beats are not harbingers of life-threatening arrhythmias, they do not require treatment in the absence of hemodynamic compromise, and they resolve with declining serum theophylline concentrations.
- Other arrhythmias, especially those associated with hemodynamic compromise, should be treated with antiarrhythmic therapy appropriate for the type of arrhythmia.
- Gastrointestinal decontamination Oral activated charcoal (0.5 g/kg up to 20 g and repeat at least once 1-2 hours after the first dose) is extremely effective in blocking the absorption of theophylline throughout the gastrointestinal tract, even when administered several hours after ingestion. * If the patient is vomiting, the charcoal should be administered through a nasogastric tube or after administration of an antiemetic. Phenothiazine antiemetics such as prochlorperazine or perphenazine should be avoided since they can lower the seizure threshold and frequently cause dystonic reactions. * A single dose of sorbitol may be used to promote stooling to facilitate removal of theophylline bound to charcoal from the gastrointestinal tract.
- Sorbitol, however, should be dosed with caution since it is a potent purgative which can cause profound fluid and electrolyte abnormalities, particularly after multiple doses.
- Commercially available fixed combinations of liquid charcoal and sorbitol should be avoided in young children and after the first dose in adolescents and adults since they do not allow for individualization of charcoal and sorbitol dosing.
- Ipecac syrup should be avoided in theophylline overdoses. Although ipecac induces emesis, it does not reduce the absorption of theophylline unless administered within 5 minutes of ingestion and even then is less effective than oral activated charcoal.
- Moreover, ipecac induced emesis may persist for several hours after a single dose and significantly decrease the retention and the effectiveness of oral activated charcoal.
- Serum Theophylline Concentration Monitoring The serum theophylline concentration should be measured immediately upon presentation, 2-4 hours later, and then at sufficient intervals, e.g., every 4 hours, to guide treatment decisions and to assess the effectiveness of therapy.
- Serum theophylline concentrations may continue to increase after presentation of the patient for medical care as a result of continued absorption of theophylline from the gastrointestinal tract.
- Serial monitoring of serum theophylline serum concentrations should be continued until it is clear that the concentration is no longer rising and has returned to non-toxic levels.
- General Monitoring Procedures Electrocardiographic monitoring should be initiated on presentation and continued until the serum theophylline level has returned to a non-toxic level.
- Serum electrolytes and glucose should be measured on presentation and at appropriate intervals indicated by clinical circumstances. Fluid and electrolyte abnormalities should be promptly corrected. Monitoring and treatment should be continued until the serum concentration decreases below 20 mcg/mL.
- Enhance clearance of theophylline Multiple-dose oral activated charcoal (e.g., 0.5 mg/kg up to 20 g, every two hours) increases the clearance of theophylline at least twofold by adsorption of theophylline secreted into gastrointestinal fluids.
- Charcoal must be retained in, and pass through, the gastrointestinal tract to be effective; emesis should therefore be controlled by administration of appropriate antiemetics.
- Alternatively, the charcoal can be administered continuously through a nasogastric tube in conjunction with appropriate antiemetics.
- A single dose of sorbitol may be administered with the activated charcoal to promote stooling to facilitate clearance of the adsorbed theophylline from the gastrointestinal tract.
- Sorbitol alone does not enhance clearance of theophylline and should be dosed with caution to prevent excessive stooling which can result in severe fluid and electrolyte imbalances.
- Commercially available fixed combinations of liquid charcoal and sorbitol should be avoided in young children and after the first dose in adolescents and adults since they do not allow for individualization of charcoal and sorbitol dosing.
- In patients with intractable vomiting, extracorporeal methods of theophylline removal should be instituted.
Specific Recommendations
Acute Overdose
- Serum Concentration >20<30 mcg/mL
- Administer a single dose of oral activated charcoal.
- Monitor the patient and obtain a serum theophylline concentration in 2-4 hours to insure that the concentration is not increasing.
- Serum Concentration >30<100 mcg/mL
- Administer multiple dose oral activated charcoal and measures to control emesis.
- Monitor the patient and obtain serial theophylline concentrations every 2-4 hours to gauge the effectiveness of therapy and to guide further treatment decisions.
- Institute extracorporeal removal if emesis, seizures, or cardiac arrhythmias cannot be adequately controlled.
- Serum Concentration >100 mcg/mL
- Consider prophylactic anticonvulsant therapy.
- Administer multiple-dose oral activated charcoal and measures to control emesis.
- Consider extracorporeal removal, even if the patient has not experienced a seizure (see OVERDOSAGE, EXTRACORPOREAL REMOVAL).
- Monitor the patient and obtain serial theophylline concentrations every 2-4 hours to gauge the effectiveness of therapy and to guide further treatment decisions.
Chronic Overdosage
- Serum Concentration >20<30 mcg/mL (with manifestations of theophylline toxicity)
- Administer a single dose of oral activated charcoal.
- Monitor the patient and obtain a serum theophylline concentration in 2-4 hours to insure that the concentration is not increasing.
- Serum Concentration >30 mcg/mL in patients <60 years of age
- Administer multiple-dose oral activated charcoal and measures to control emesis.
- Monitor the patient and obtain serial theophylline concentrations every 2-4 hours to gauge the effectiveness of therapy and to guide further treatment decisions.
- Institute extracorporeal removal if emesis, seizures, or cardiac arrhythmias cannot be adequately controlled.
- Serum Concentration >30 mcg/mL in patients ≥60 years of age.
- Consider prophylactic anticonvulsant therapy.
- Administer multiple-dose oral activated charcoal and measures to control emesis.
- Consider extracorporeal removal even if the patient has not experienced a seizure (see OVERDOSAGE, EXTRACORPOREAL REMOVAL).
- Monitor the patient and obtain serial theophylline concentrations every 2-4 hours to gauge the effectiveness of therapy and to guide further treatment decisions.
=Extracorporeal Removal=
- Increasing the rate of theophylline clearance by extracorporeal methods may rapidly decrease serum concentrations, but the risks of the procedure must be weighed against the potential benefit. Charcoal hemoperfusion is the most effective method of extracorporeal removal, increasing theophylline clearance up to six fold, but serious complications, including hypotension, hypocalcemia, platelet consumption and bleeding diatheses may occur.
- Hemodialysis is about as efficient as multiple-dose oral activated charcoal and has a lower risk of serious complications than charcoal hemoperfusion.
- Hemodialysis should be considered as an alternative when charcoal hemoperfusion is not feasible and multiple-dose oral charcoal is ineffective because of intractable emesis.
- Serum theophylline concentrations may rebound 5-10 mcg/mL after discontinuation of charcoal hemoperfusion or hemodialysis due to redistribution of theophylline from the tissue compartment. Peritoneal dialysis is ineffective for theophylline removal; exchange transfusions in neonates have been minimally effective
Pharmacology
There is limited information regarding Theophylline Pharmacology in the drug label.
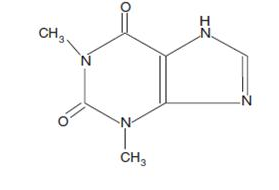
Mechanism of Action
Structure
This image is provided by the National Library of Medicine.
Pharmacodynamics
There is limited information regarding Pharmacodynamics of Theophylline in the drug label.
Pharmacokinetics
There is limited information regarding Pharmacokinetics of Theophylline in the drug label.
Nonclinical Toxicology
There is limited information regarding Nonclinical Toxicology of Theophylline in the drug label.
Clinical Studies
There is limited information regarding Clinical Studies of Theophylline in the drug label.
How Supplied
Storage
There is limited information regarding Theophylline Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Theophylline |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Theophylline |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
There is limited information regarding Patient Counseling Information of Theophylline in the drug label.
Precautions with Alcohol
- Alcohol-Theophylline interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- ®[1]
Look-Alike Drug Names
- A® — B®[2]
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Empty citation (help)
- ↑ "http://www.ismp.org". External link in
|title=(help)
{{#subobject:
|Page Name=Theophylline
|Pill Name=No image.jpg
|Drug Name=
|Pill Ingred=|+sep=;
|Pill Imprint=
|Pill Dosage={{{dosageValue}}} {{{dosageUnit}}}
|Pill Color=|+sep=;
|Pill Shape=
|Pill Size (mm)=
|Pill Scoring=
|Pill Image=
|Drug Author=
|NDC=
}}
{{#subobject:
|Label Page=Theophylline |Label Name=Theophylline11.png
}}
{{#subobject:
|Label Page=Theophylline |Label Name=Theophylline11.png
}}