Zelnorm® (tegaserod maleate) is indicated for the short-term treatment of women with irritable bowel syndrome (IBS) whose primary bowel symptom is constipation.
* Tegaserod maleate is indicated for the short-term treatment of women with [[irritable bowel syndrome]] (IBS) whose primary [[bowel]] symptom is [[constipation]].
* The safety and effectiveness of Zelnorm in men with IBS with [[constipation]] have not been established.
The safety and effectiveness of Zelnorm in men with IBS with constipation have not been established.
=====Chronic Idiopathic Constipation=====
* Tegaserod maleate is indicated for the treatment of patients less than 65 years of age with chronic idiopathic [[constipation]]. The effectiveness of Zelnorm in patients 65 years or older with chronic idiopathic [[constipation]] has not been established.
Chronic Idiopathic Constipation
* The efficacy of tegaserod maleate for the treatment of IBS with constipation or chronic idiopathic [[constipation]] has not been studied beyond 12 weeks.
Zelnorm® (tegaserod maleate) is indicated for the treatment of patients less than 65 years of age with chronic idiopathic constipation. The effectiveness of Zelnorm in patients 65 years or older with chronic idiopathic constipation has not been established (see Geriatric Use).
* IBS with Constipation: The recommended dosage of Tegaserod maleate is 6 mg taken twice daily orally before meals for 4-6 weeks. For those women who respond to therapy at 4-6 weeks, an additional 4-6 week course can be considered.
* Chronic Idiopathic [[Constipation]]
The efficacy of Zelnorm for the treatment of IBS with constipation or chronic idiopathic constipation has not been studied beyond 12 weeks.
:* The recommended dosage of tegaserod maleate is 6 mg taken twice daily orally before meals. :* Physicians and patients should periodically assess the need for continued therapy.
IBS with Constipation: The recommended dosage of Zelnorm® (tegaserod maleate) is 6 mg taken twice daily orally before meals for 4-6 weeks. For those women who respond to therapy at 4-6 weeks, an additional 4-6 week course can be considered.
|offLabelAdultGuideSupport=There is limited information regarding <i>Off-Label Guideline-Supported Use</i> of {{PAGENAME}} in adult patients.
Chronic Idiopathic Constipation: The recommended dosage of Zelnorm is 6 mg taken twice daily orally before meals. Physicians and patients should periodically assess the need for continued therapy.
|offLabelAdultGuideSupport=
There is limited information regarding <i>Off-Label Guideline-Supported Use</i> of {{PAGENAME}} in adult patients.
<!--Non–Guideline-Supported Use (Adult)-->
<!--Non–Guideline-Supported Use (Adult)-->
|offLabelAdultNoGuideSupport=
|offLabelAdultNoGuideSupport=There is limited information regarding <i>Off-Label Non–Guideline-Supported Use</i> of {{PAGENAME}} in adult patients.
There is limited information regarding <i>Off-Label Non–Guideline-Supported Use</i> of {{PAGENAME}} in adult patients.
<!--Pediatric Indications and Dosage-->
<!--Pediatric Indications and Dosage-->
<!--FDA-Labeled Indications and Dosage (Pediatric)-->
<!--FDA-Labeled Indications and Dosage (Pediatric)-->
|fdaLIADPed=
|fdaLIADPed=There is limited information regarding <i>FDA-Labeled Use</i> of {{PAGENAME}} in pediatric patients.
There is limited information regarding <i>FDA-Labeled Use</i> of {{PAGENAME}} in pediatric patients.
<!--Off-Label Use and Dosage (Pediatric)-->
<!--Off-Label Use and Dosage (Pediatric)-->
<!--Guideline-Supported Use (Pediatric)-->
<!--Guideline-Supported Use (Pediatric)-->
|offLabelPedGuideSupport=
|offLabelPedGuideSupport=There is limited information regarding <i>Off-Label Guideline-Supported Use</i> of {{PAGENAME}} in pediatric patients.
There is limited information regarding <i>Off-Label Guideline-Supported Use</i> of {{PAGENAME}} in pediatric patients.
<!--Non–Guideline-Supported Use (Pediatric)-->
<!--Non–Guideline-Supported Use (Pediatric)-->
|offLabelPedNoGuideSupport=
|offLabelPedNoGuideSupport=There is limited information regarding <i>Off-Label Non–Guideline-Supported Use</i> of {{PAGENAME}} in pediatric patients.
There is limited information regarding <i>Off-Label Non–Guideline-Supported Use</i> of {{PAGENAME}} in pediatric patients.
<!--Contraindications-->
<!--Contraindications-->
|contraindications=* Zelnorm® (tegaserod maleate) is contraindicated in those patients with:
|contraindications=* Tegaserod maleate is contraindicated in those patients with:
:* Severe renal impairment.
severe renal impairment
:* Moderate or severe hepatic impairment.
moderate or severe hepatic impairment
:* A history of bowel obstruction, symptomatic [[gallbladder]] disease, suspected [[sphincter of Oddi]] dysfunction, or [[abdominal adhesions]].
a history of bowel obstruction, symptomatic gallbladder disease, suspected sphincter of Oddi dysfunction, or abdominal adhesions
:* A known [[hypersensitivity]] to the drug or any of its excipients.
a known hypersensitivity to the drug or any of its excipients
|warnings=* Serious consequences of [[diarrhea]], including [[hypovolemia]], [[hypotension]], and [[syncope]] have been reported in the clinical studies and during marketed use of Tegaserod maleate In some cases, these complications have required hospitalization for rehydration. Tegaserod maleate should be discontinued immediately in patients who develop severe [[diarrhea]], [[hypotension]] or [[syncope]]. tegaserod maleate should not be initiated in patients who are currently experiencing or frequently experience [[diarrhea]].
|warnings=* Serious consequences of diarrhea, including hypovolemia, hypotension, and syncope have been reported in the clinical studies and during marketed use of Zelnorm® (tegaserod maleate) In some cases, these complications have required hospitalization for rehydration. Zelnorm should be discontinued immediately in patients who develop severe diarrhea, hypotension or syncope. Zelnorm should not be initiated in patients who are currently experiencing or frequently experience diarrhea
|clinicalTrials======IBS with Constipation=====
|clinicalTrials=IBS with Constipation
* In Phase 3 clinical trials 2,632 female and male patients received Tegaserod maleate 6 mg b.i.d. or [[placebo]]. The frequency and type of adverse events for females and males were similar. The following adverse experiences were reported in 1% or more of patients who received tegaserod maleate and occurred more frequently on tegaserod maleate than placebo:
In Phase 3 clinical trials 2,632 female and male patients received Zelnorm® (tegaserod maleate) 6 mg b.i.d. or placebo. The frequency and type of adverse events for females and males were similar. The following adverse experiences were reported in 1% or more of patients who received Zelnorm and occurred more frequently on Zelnorm than placebo:
: [[File:Terg 05 Adverse effc.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
=====Chronic Idiopathic Constipation=====
Chronic Idiopathic Constipation
* In Phase 3 clinical trials 2,603 male and female patients received tegaserod maleate 6 mg b.i.d., 2 mg b.i.d. or placebo. The following adverse experiences were reported in 1% or more of patients who received tegaserod maleate and occurred more frequently than in patients who received placebo.
In Phase 3 clinical trials 2,603 male and female patients received Zelnorm 6 mg b.i.d., 2 mg b.i.d. or placebo. The following adverse experiences were reported in 1% or more of patients who received Zelnorm and occurred more frequently than in patients who received placebo.
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
Zelnorm was not associated with changes in ECG intervals.
* Tegaserod maleate was not associated with changes in ECG intervals.
* Tegaserod maleate-Induced [[Diarrhea]].
Zelnorm-Induced Diarrhea
=====IBS with Constipation=====
IBS with Constipation
* In the Phase 3 clinical studies, 8.8% of patients receiving tegaserod maleate reported diarrhea as an adverse experience compared to 3.8% of patients receiving [[placebo]]. The majority of the tegaserod maleate patients reporting diarrhea had a single episode. In most cases, diarrhea occurred within the first week of treatment. Typically, [[diarrhea]] resolved with continued therapy. Overall, the discontinuation rate from the studies due to diarrhea was 1.6% among the tegaserod maleate-treated patients. In clinical studies, a small number of patients (0.04%) experienced clinically significant [[diarrhea]] including hospitalization, [[hypovolemia]], [[hypotension]] and need for intravenous fluids. [[Diarrhea]] can be the pharmacologic response to tegaserod maleate.
=====Chronic Idiopathic Constipation=====
In the Phase 3 clinical studies, 8.8% of patients receiving Zelnorm reported diarrhea as an adverse experience compared to 3.8% of patients receiving placebo. The majority of the Zelnorm patients reporting diarrhea had a single episode. In most cases, diarrhea occurred within the first week of treatment. Typically, diarrhea resolved with continued therapy. Overall, the discontinuation rate from the studies due to diarrhea was 1.6% among the Zelnorm-treated patients. In clinical studies, a small number of patients (0.04%) experienced clinically significant diarrhea including hospitalization, hypovolemia, hypotension and need for intravenous fluids. Diarrhea can be the pharmacologic response to Zelnorm.
* In the two Phase 3 studies, 6.6% of patients treated with tegaserod maleate 6 mg b.i.d. and 4.2% of patients treated with tegaserod maleate 2 mg b.i.d. reported [[diarrhea]] as an adverse event, versus 3.0% of patients receiving placebo.
* The diarrhea episodes experienced by patients treated with tegaserod occurred early after initiation of treatment (median of 5.5 days), were of short duration (median of 2.5 days), and occurred only once in the majority of patient.
Chronic Idiopathic Constipation
* Typically, [[diarrhea]] resolved with continued therapy; only 0.9% of patients treated with tegaserod maleate 6 mg b.i.d. discontinued the study due to [[diarrhea]] (compared to 0.3% in the tegaserod maleate 2 mg b.i.d. group and 0.2% in the placebo group).
=====Abdominal Surgeries, Including Cholecystectomy=====
In the two Phase 3 studies, 6.6% of patients treated with Zelnorm 6 mg b.i.d. and 4.2% of patients treated with Zelnorm 2 mg b.i.d. reported diarrhea as an adverse event, versus 3.0% of patients receiving placebo.
* An increase in abdominal surgeries was observed on tegaserod maleate (9/2,965; 0.3%) vs. placebo (3/1,740; 0.2%) in the Phase 3 IBS clinical studies. The increase was primarily due to a numerical imbalance in [[cholecystectomies]] reported in patients treated with tegaserod maleate (5/2,965; 0.17%) vs. placebo (1/1,740; 0.06%). In [[chronic idiopathic constipation]] clinical trials there was no increase in the frequency of abdominal and pelvic surgeries in active vs. placebo groups: 9/1,752; 0.5% on tegaserod maleate versus 8/861; 0.9% on placebo. A causal relationship between abdominal surgeries and tegaserod maleate has not been established.
=====Other Adverse Events=====
The diarrhea episodes experienced by patients treated with tegaserod occurred early after initiation of treatment (median of 5.5 days), were of short duration (median of 2.5 days), and occurred only once in the majority of patients.
* The following list of adverse events includes those from Phase 3 clinical studies (6 mg b.i.d. or 2 mg b.i.d.) which were reported more frequently (>0.2%) in patients on tegaserod maleate than placebo; or which were considered by the investigator to be possibly related to tegaserod maleate and reported more frequently (>0.1%) on tegaserod maleate than placebo; or which lead to discontinuation more frequently (≥0.1% and in more than 1 patient) on tegaserod maleate than placebo. The list also contains those serious adverse events from all clinical trials in patients treated with either 6 mg b.i.d. or 2 mg b.i.d. tegaserod maleate which were either considered by the investigator as possibly drug related, or occurred in at least 2 more patients on tegaserod maleate than on placebo. Although the events reported occurred during treatment with tegaserod maleate, they were not necessarily caused by it.
* Cardiac Disorders.
Typically, diarrhea resolved with continued therapy; only 0.9% of patients treated with Zelnorm 6 mg b.i.d. discontinued the study due to diarrhea (compared to 0.3% in the Zelnorm 2 mg b.i.d. group and 0.2% in the placebo group).
An increase in abdominal surgeries was observed on Zelnorm (9/2,965; 0.3%) vs. placebo (3/1,740; 0.2%) in the Phase 3 IBS clinical studies. The increase was primarily due to a numerical imbalance in cholecystectomies reported in patients treated with Zelnorm (5/2,965; 0.17%) vs. placebo (1/1,740; 0.06%). In chronic idiopathic constipation clinical trials there was no increase in the frequency of abdominal and pelvic surgeries in active vs. placebo groups: 9/1,752; 0.5% on Zelnorm versus 8/861; 0.9% on placebo. A causal relationship between abdominal surgeries and Zelnorm has not been established.
* General Disorders and Administration Site Conditions.
The following list of adverse events includes those from Phase 3 clinical studies (6 mg b.i.d. or 2 mg b.i.d.) which were reported more frequently (>0.2%) in patients on Zelnorm than placebo; or which were considered by the investigator to be possibly related to Zelnorm and reported more frequently (>0.1%) on Zelnorm than placebo; or which lead to discontinuation more frequently (≥0.1% and in more than 1 patient) on Zelnorm than placebo. The list also contains those serious adverse events from all clinical trials in patients treated with either 6 mg b.i.d. or 2 mg b.i.d. Zelnorm which were either considered by the investigator as possibly drug related, or occurred in at least 2 more patients on Zelnorm than on placebo. Although the events reported occurred during treatment with Zelnorm, they were not necessarily caused by it.
Metabolism and Nutrition Disorders: Increased appetite
:* [[holecystectomy]].
* Vascular Disorders.
Neoplasms Benign, Malignant and Unspecified (including cysts and polyps): Breast carcinoma
:* [[Flushing]], [[hypotension]].
|postmarketing=* [[ischemic colitis]], [[mesenteric ischemia]], [[gangrenous bowel]], rectal bleeding,[[syncope]], [[hypotension]], [[hypovolemia]], [[electrolyte disorders]], suspected [[sphincter of Oddi]] spasm, [[bile duct stone]], [[cholecystitis]] with elevated transaminases, and [[ypersensitivity]] reaction including [[rash]], [[urticaria]], [[pruritus]] and serious allergic Type I reactions. Because these cases are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. No causal relationship between these events and tegaserod maleate use has been established.
* Post-marketing reports of [[diarrhea]], which can be a pharmacologic response to tegaserod maleate, have also been received.
Respiratory, Thoracic and Mediastinal Disorders: Dyspnea, pharyngolaryngeal pain
Reproductive System and Breast Disorders: Miscarriage, menorrhagia
Surgical and Medical Procedures: Cholecystectomy
Vascular Disorders: Flushing, hypotension
|postmarketing=Voluntary reports of adverse events occurring with the use of Zelnorm include the following: ischemic colitis (see PRECAUTIONS), mesenteric ischemia, gangrenous bowel, rectal bleeding, syncope, hypotension, hypovolemia, electrolyte disorders, suspected sphincter of Oddi spasm, bile duct stone, cholecystitis with elevated transaminases, and hypersensitivity reaction including rash, urticaria, pruritus and serious allergic Type I reactions. Because these cases are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. No causal relationship between these events and Zelnorm use has been established.
Post-marketing reports of diarrhea, which can be a pharmacologic response to Zelnorm, have also been received.
|FDAPregCat=B
|FDAPregCat=B
|useInPregnancyFDA=* Reproduction studies have been performed in rats at oral doses up to 100 mg/kg/day (approximately 15 times the human exposure at 6 mg b.i.d. based on plasma AUC0-24 hr) and rabbits at oral doses up to 120 mg/kg/day (approximately 51 times the human exposure at 6 mg b.i.d. based on plasma AUC0-24 hr) and have revealed no evidence of impaired fertility or harm to the fetus due to tegaserod. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
|useInPregnancyFDA=* Reproduction studies have been performed in rats at oral doses up to 100 mg/kg/day (approximately 15 times the human exposure at 6 mg b.i.d. based on plasma AUC0-24 hr) and rabbits at oral doses up to 120 mg/kg/day (approximately 51 times the human exposure at 6 mg b.i.d. based on plasma AUC0-24 hr) and have revealed no evidence of impaired fertility or harm to the fetus due to tegaserod. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Line 131:
Line 106:
|useInNursing=* Tegaserod and its metabolites are excreted in the milk of lactating rats with a high milk to plasma ratio. It is not known whether tegaserod is excreted in human milk. Many drugs, which are excreted in human milk, have potential for serious adverse reactions in nursing infants. Based on the potential for tumorigenicity shown for tegaserod in the mouse carcinogenicity study, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
|useInNursing=* Tegaserod and its metabolites are excreted in the milk of lactating rats with a high milk to plasma ratio. It is not known whether tegaserod is excreted in human milk. Many drugs, which are excreted in human milk, have potential for serious adverse reactions in nursing infants. Based on the potential for tumorigenicity shown for tegaserod in the mouse carcinogenicity study, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
|useInPed=There is no FDA guidance on the use of {{PAGENAME}} with respect to pediatric patients.
|useInPed=There is no FDA guidance on the use of {{PAGENAME}} with respect to pediatric patients.
|useInGeri=IBS with Constipation
|useInGeri======IBS with Constipation=====
* Of 4,035 patients in Phase 3 clinical studies of tegaserod maleate, 290 were at least 65 years of age, while 52 were at least 75 years old. No overall differences in safety were observed between these patients and younger patients with regard to adverse events.
Of 4,035 patients in Phase 3 clinical studies of Zelnorm, 290 were at least 65 years of age, while 52 were at least 75 years old. No overall differences in safety were observed between these patients and younger patients with regard to adverse events.
* No dose adjustment is necessary when administering tegaserod maleate to patients with IBS with constipation over 65 years old.
=====Chronic Idiopathic Constipation=====
No dose adjustment is necessary when administering Zelnorm to patients with IBS with constipation over 65 years old. (See CLINICAL PHARMACOLOGY.)
* Of 2,612 patients in Phase 3 clinical studies of tegaserod maleate, 331 were at least 65 years of age. Efficacy in patients 65 years of age or greater showed no significant difference between drug and placebo responses. Patients 65 years of age or greater who received tegaserod maleate experienced a higher incidence of diarrhea and discontinuations due to diarrhea than patients younger than 65.
Chronic Idiopathic Constipation
Of 2,612 patients in Phase 3 clinical studies of Zelnorm, 331 were at least 65 years of age. Efficacy in patients 65 years of age or greater showed no significant difference between drug and placebo responses. Patients 65 years of age or greater who received Zelnorm experienced a higher incidence of diarrhea and discontinuations due to diarrhea than patients younger than 65.
|useInGender=There is no FDA guidance on the use of {{PAGENAME}} with respect to specific gender populations.
|useInGender=There is no FDA guidance on the use of {{PAGENAME}} with respect to specific gender populations.
|useInRace=There is no FDA guidance on the use of {{PAGENAME}} with respect to specific racial populations.
|useInRace=There is no FDA guidance on the use of {{PAGENAME}} with respect to specific racial populations.
Line 148:
Line 119:
<!--Administration and Monitoring-->
<!--Administration and Monitoring-->
|administration=* Oral
|administration=* [[Oral]].
|monitoring=There is limited information regarding <i>Monitoring</i> of {{PAGENAME}} in the drug label.
|monitoring=There is limited information regarding <i>Monitoring</i> of {{PAGENAME}} in the drug label.
Line 157:
Line 126:
<!--Overdosage-->
<!--Overdosage-->
|overdose=* There have been no reports of human overdosage with Zelnorm® (tegaserod maleate). Single oral doses of 120 mg of tegaserod were administered to 3 healthy volunteers in 1 study. All 3 subjects developed diarrhea and headache. Two of these subjects also reported intermittent abdominal pain, and 1 developed orthostatic hypotension. In 28 healthy subjects exposed to doses of tegaserod of 90 to 180 mg/d for several days, adverse events were diarrhea (100%), headache (57%), abdominal pain (18%), flatulence (18%), nausea (7%) and vomiting (7%).
|overdose=* There have been no reports of human overdosage with tegaserod maleate. Single oral doses of 120 mg of tegaserod were administered to 3 healthy volunteers in 1 study. All 3 subjects developed diarrhea and headache. Two of these subjects also reported intermittent abdominal pain, and 1 developed orthostatic hypotension. In 28 healthy subjects exposed to doses of tegaserod of 90 to 180 mg/d for several days, adverse events were diarrhea (100%), headache (57%), abdominal pain (18%), flatulence (18%), nausea (7%) and vomiting (7%).
* Based on the large distribution volume and high protein binding of tegaserod it is unlikely that tegaserod could be removed by dialysis. In cases of overdosage treat symptomatically and institute supportive measures as appropriate.
Based on the large distribution volume and high protein binding of tegaserod it is unlikely that tegaserod could be removed by dialysis. In cases of overdosage treat symptomatically and institute supportive measures as appropriate.
|drugBox=: [[File:Tegaserod - Wikipedia, the free encyclopedia.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
|drugBox=<!--Mechanism of Action-->
|mechAction=* [[Irritable bowel syndrome]] with [[constipation]] and [[chronic idiopathic constipation]] are both lower gastrointestinal dysmotility disorders. Clinical investigations have shown that both motor and sensory functions of the gut appear to be altered in patients suffering from [[irritable bowel syndrome]] (IBS), while in patients with [[chronic idiopathic constipation]], reduced intestinal motility is the predominant cause of the condition. Both the enteric nervous system, which acts to integrate and process information in the gut, and 5-hydroxytryptamine (5-HT, serotonin) are thought to represent key elements in the etiology of both IBS and idiopathic constipation. Approximately 95% of serotonin is found throughout the gastrointestinal tract, primarily stored in enterochromaffin cells but also in enteric nerves acting as a [[neurotransmitter]]. [[Serotonin]] has been shown to be involved in regulating motility, visceral sensitivity and intestinal secretion. Investigations suggest an important role of serotonin Type-4 (5-HT4) receptors in the maintenance of gastrointestinal functions in humans. 5-HT4 receptor mRNA has been found throughout the human gastrointestinal tract.
|mechAction=* Irritable bowel syndrome with constipation and chronic idiopathic constipation are both lower gastrointestinal dysmotility disorders. Clinical investigations have shown that both motor and sensory functions of the gut appear to be altered in patients suffering from irritable bowel syndrome (IBS), while in patients with chronic idiopathic constipation, reduced intestinal motility is the predominant cause of the condition. Both the enteric nervous system, which acts to integrate and process information in the gut, and 5-hydroxytryptamine (5-HT, serotonin) are thought to represent key elements in the etiology of both IBS and idiopathic constipation. Approximately 95% of serotonin is found throughout the gastrointestinal tract, primarily stored in enterochromaffin cells but also in enteric nerves acting as a neurotransmitter. Serotonin has been shown to be involved in regulating motility, visceral sensitivity and intestinal secretion. Investigations suggest an important role of serotonin Type-4 (5-HT4) receptors in the maintenance of gastrointestinal functions in humans. 5-HT4 receptor mRNA has been found throughout the human gastrointestinal tract.
* Tegaserod is a 5-HT4 receptor partial agonist that binds with high affinity at human 5-HT4 receptors, whereas it has no appreciable affinity for 5-HT3 or [[dopamine]] receptors. It has moderate affinity for 5-HT1 receptors. Tegaserod, by acting as an agonist at neuronal 5-HT4 receptors, triggers the release of further neurotransmitters such as [[calcitonin]] gene-related peptide from sensory neurons.
* The activation of 5-HT4 receptors in the gastrointestinal tract stimulates the peristaltic reflex and intestinal secretion, as well as inhibits visceral sensitivity. In vivo studies showed that tegaserod enhanced basal motor activity and normalized impaired motility throughout the gastrointestinal tract. In addition, studies demonstrated that tegaserod moderated visceral sensitivity during colorectal distension in animals.
Tegaserod is a 5-HT4 receptor partial agonist that binds with high affinity at human 5-HT4 receptors, whereas it has no appreciable affinity for 5-HT3 or dopamine receptors. It has moderate affinity for 5-HT1 receptors. Tegaserod, by acting as an agonist at neuronal 5-HT4 receptors, triggers the release of further neurotransmitters such as calcitonin gene-related peptide from sensory neurons. The activation of 5-HT4 receptors in the gastrointestinal tract stimulates the peristaltic reflex and intestinal secretion, as well as inhibits visceral sensitivity. In vivo studies showed that tegaserod enhanced basal motor activity and normalized impaired motility throughout the gastrointestinal tract. In addition, studies demonstrated that tegaserod moderated visceral sensitivity during colorectal distension in animals.
|structure=* Tegaserod maleate tablets contain tegaserod as the hydrogen maleate salt. As the maleate salt, tegaserod is chemically designated as 3-(5-methoxy-1H-indol-3-ylmethylene)-N-pentylcarbazimidamide hydrogen maleate. Its empirical formula is C16H23N5O•C4H4O4. The molecular weight is 417.47 and the structural formula is
|structure=*
: [[File:Terg 01 Structure.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
* Tegaserod as the maleate salt is a white to off-white crystalline powder and is slightly soluble in ethanol and very slightly soluble in water. Each 1.385 mg of tegaserod as the maleate is equivalent to 1 mg of tegaserod. Tegaserod maleate is available for oral use in the following tablet formulations:
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
:* 2-mg and 6-mg tablets (blister packs) containing 2 mg and 6 mg tegaserod, respectively and the following inactive ingredients: crospovidone, glyceryl monostearate, hypromellose, lactose monohydrate, poloxamer 188, and polyethylene glycol 4000
:* 6-mg tablets (bottles) containing 6 mg tegaserod and the following inactive ingredients: crospovidone, glyceryl behenate, hypromellose, lactose monohydrate, and colloidal silicon dioxide.
<!--Pharmacodynamics-->
<!--Pharmacodynamics-->
Line 172:
Line 142:
<!--Pharmacokinetics-->
<!--Pharmacokinetics-->
|PK=Absorption
|PK======Absorption=====
* Peak plasma concentrations are reached approximately 1 hour after oral dosing. The absolute bioavailability of tegaserod when administered to fasting subjects is approximately 10%. The pharmacokinetics are dose proportional over the 2 mg to 12 mg range given twice daily for 5 days. There was no clinically relevant accumulation of tegaserod in plasma when a 6 mg b.i.d. dose was given for 5 days.
Peak plasma concentrations are reached approximately 1 hour after oral dosing. The absolute bioavailability of tegaserod when administered to fasting subjects is approximately 10%. The pharmacokinetics are dose proportional over the 2 mg to 12 mg range given twice daily for 5 days. There was no clinically relevant accumulation of tegaserod in plasma when a 6 mg b.i.d. dose was given for 5 days. (See DOSAGE AND ADMINISTRATION.)
=====Food Effects=====
* When the drug is administered with food, the bioavailability of tegaserod is reduced by 40%-65% and Cmax by approximately 20%-40%. Similar reductions in plasma concentration occur when tegaserod is administered to subjects within 30 minutes prior to a meal, or 2.5 hours after a meal. Tmax of tegaserod is prolonged from approximately 1 hour to 2 hours when taken following a meal, but decreased to 0.7 hours when taken 30 minutes prior to a meal.
Food Effects
=====Distribution=====
* Tegaserod is approximately 98% bound to plasma proteins, predominantly alpha-1-acid glycoprotein. Tegaserod exhibits pronounced distribution into tissues following intravenous dosing with a volume of distribution at steady-state of 368 ± 223 L.
When the drug is administered with food, the bioavailability of tegaserod is reduced by 40%-65% and Cmax by approximately 20%-40%. Similar reductions in plasma concentration occur when tegaserod is administered to subjects within 30 minutes prior to a meal, or 2.5 hours after a meal. Tmax of tegaserod is prolonged from approximately 1 hour to 2 hours when taken following a meal, but decreased to 0.7 hours when taken 30 minutes prior to a meal.
=====Metabolism=====
* Tegaserod is metabolized mainly via two pathways. The first is a presystemic acid catalyzed hydrolysis in the stomach followed by oxidation and conjugation which produces the main metabolite of tegaserod, 5-methoxyindole-3-carboxylic acid glucuronide. The main metabolite has negligible affinity for 5-HT4 receptors in vitro. In humans, systemic exposure to tegaserod was not altered at neutral gastric pH values. The second metabolic pathway of tegaserod is direct glucuronidation which leads to generation of three isomeric N-glucuronides.
Distribution
=====Elimination=====
* The plasma clearance of tegaserod is 77 ± 15 L/h with an estimated terminal half-life (T1/2) of 11 ± 5 hours following intravenous dosing. Approximately two-thirds of the orally administered dose of tegaserod is excreted unchanged in the feces, with the remaining one-third excreted in the urine, primarily as the main metabolite.
Tegaserod is approximately 98% bound to plasma proteins, predominantly alpha-1-acid glycoprotein. Tegaserod exhibits pronounced distribution into tissues following intravenous dosing with a volume of distribution at steady-state of 368 ± 223 L.
=====Sub Populations=====
* Patients
Metabolism
:* The pharmacokinetics of tegaserod in IBS patients are comparable to those in healthy subjects. The pharmacokinetics of tegaserod in patients with chronic idiopathic constipation have not been studied.
:* Reduced Renal Function: No change in the pharmacokinetics of tegaserod was observed in subjects with severe renal impairment requiring hemodialysis (creatinine clearance <15 mL/min/1.73 m2). Cmax and AUC of the main pharmacologically inactive metabolite of tegaserod, 5-methoxy-indole-3-carboxylic acid glucuronide, increased 2- and 10-fold respectively, in subjects with severe renal impairment compared to healthy controls. No dosage adjustment is required in patients with mild-to-moderate renal impairment. Tegaserod is not recommended in patients with severe renal impairment.
Tegaserod is metabolized mainly via two pathways. The first is a presystemic acid catalyzed hydrolysis in the stomach followed by oxidation and conjugation which produces the main metabolite of tegaserod, 5-methoxyindole-3-carboxylic acid glucuronide. The main metabolite has negligible affinity for 5-HT4 receptors in vitro. In humans, systemic exposure to tegaserod was not altered at neutral gastric pH values. The second metabolic pathway of tegaserod is direct glucuronidation which leads to generation of three isomeric N-glucuronides.
* Reduced Hepatic Function
:* In subjects with mild hepatic impairment, mean AUC was 31% higher and Cmax 16% higher compared to subjects with normal hepatic function. No dosage adjustment is required in patients with mild impairment, however, caution is recommended when using tegaserod in this patient population. Tegaserod has not adequately been studied in patients with moderate and severe hepatic impairment, and is therefore not recommended in these patients.
Elimination
* Gender
:* Gender has no effect on the pharmacokinetics of tegaserod.
The plasma clearance of tegaserod is 77 ± 15 L/h with an estimated terminal half-life (T1/2) of 11 ± 5 hours following intravenous dosing. Approximately two-thirds of the orally administered dose of tegaserod is excreted unchanged in the feces, with the remaining one-third excreted in the urine, primarily as the main metabolite.
* Race
:* Data were inadequate to assess the effect of race on the pharmacokinetics of tegaserod.
Sub Populations
* Age
:* In a clinical pharmacology study conducted to assess the pharmacokinetics of tegaserod administered to healthy young (18-40 years) and healthy elderly (65-85 years) subjects, peak plasma concentration and exposure were 22% and 40% greater, respectively, in elderly females than young females but still within the variability seen in tegaserod pharmacokinetics in healthy subjects. Based on an analysis across several pharmacokinetic studies in healthy subjects, there is no age effect on the pharmacokinetics of tegaserod when allowing for body weight as a covariate. Therefore, dose adjustment in elderly patients who have IBS with constipation is not necessary.
Patients: The pharmacokinetics of tegaserod in IBS patients are comparable to those in healthy subjects. The pharmacokinetics of tegaserod in patients with chronic idiopathic constipation have not been studied.
Reduced Renal Function: No change in the pharmacokinetics of tegaserod was observed in subjects with severe renal impairment requiring hemodialysis (creatinine clearance <15 mL/min/1.73 m2). Cmax and AUC of the main pharmacologically inactive metabolite of tegaserod, 5-methoxy-indole-3-carboxylic acid glucuronide, increased 2- and 10-fold respectively, in subjects with severe renal impairment compared to healthy controls. No dosage adjustment is required in patients with mild-to-moderate renal impairment. Tegaserod is not recommended in patients with severe renal impairment.
Reduced Hepatic Function: In subjects with mild hepatic impairment, mean AUC was 31% higher and Cmax 16% higher compared to subjects with normal hepatic function. No dosage adjustment is required in patients with mild impairment, however, caution is recommended when using tegaserod in this patient population. Tegaserod has not adequately been studied in patients with moderate and severe hepatic impairment, and is therefore not recommended in these patients.
Gender: Gender has no effect on the pharmacokinetics of tegaserod.
Race: Data were inadequate to assess the effect of race on the pharmacokinetics of tegaserod.
Age: In a clinical pharmacology study conducted to assess the pharmacokinetics of tegaserod administered to healthy young (18-40 years) and healthy elderly (65-85 years) subjects, peak plasma concentration and exposure were 22% and 40% greater, respectively, in elderly females than young females but still within the variability seen in tegaserod pharmacokinetics in healthy subjects. Based on an analysis across several pharmacokinetic studies in healthy subjects, there is no age effect on the pharmacokinetics of tegaserod when allowing for body weight as a covariate. Therefore, dose adjustment in elderly patients who have IBS with constipation is not necessary.
|nonClinToxic=There is limited information regarding <i>Nonclinical Toxicology</i> of {{PAGENAME}} in the drug label.
|nonClinToxic=There is limited information regarding <i>Nonclinical Toxicology</i> of {{PAGENAME}} in the drug label.
<!--Clinical Studies-->
<!--Clinical Studies-->
|clinicalStudies=IBS with Constipation
|clinicalStudies======IBS with Constipation=====
RESULTS IN WOMEN: In three multicenter, double-blind, placebo-controlled studies, 2,470 women (mean age 43 years [range 17-89 years]; 86% Caucasian, 10% African American) with at least a 3-month history of IBS symptoms prior to the study baseline period that included abdominal pain, bloating and constipation received either Zelnorm® (tegaserod maleate) 6 mg b.i.d. or placebo. In all patients, constipation was characterized by at least two of the following three symptoms each occurring ≥25% of the time over a 3-month period:< 3 bowel movements/week, hard or lumpy stools, or straining with a bowel movement. The study design consisted of a 4-week placebo-free baseline period followed by a 12-week double-blind treatment period. Study 1 and 2 evaluated a fixed dose regimen of tegaserod 6 mg b.i.d. while Study 3 utilized a dose-titration design.
* RESULTS IN WOMEN: In three multicenter, double-blind, placebo-controlled studies, 2,470 women (mean age 43 years [range 17-89 years]; 86% Caucasian, 10% African American) with at least a 3-month history of IBS symptoms prior to the study baseline period that included abdominal pain, bloating and constipation received either tegaserod maleate® (tegaserod maleate) 6 mg b.i.d. or placebo. In all patients, constipation was characterized by at least two of the following three symptoms each occurring ≥25% of the time over a 3-month period:< 3 bowel movements/week, hard or lumpy stools, or straining with a bowel movement. The study design consisted of a 4-week placebo-free baseline period followed by a 12-week double-blind treatment period. Study 1 and 2 evaluated a fixed dose regimen of tegaserod 6 mg b.i.d. while Study 3 utilized a dose-titration design.
* Each week of the 4-week placebo-free baseline period and the 12-week double-blind treatment period, patients were asked the question, “Please consider how you felt this past week in regard to your IBS, in particular your overall well-being, and symptoms of abdominal discomfort, pain and altered bowel habit. Compared to the way you usually felt before entering the study, how would you rate your relief of symptoms during the past week?” The response variable consisted of the following 5 categories: completely relieved, considerably relieved, somewhat relieved, unchanged, or worse. Patients were classified as responders within a month if they were considerably or completely relieved for at least two of the four weeks, or if they were at least somewhat relieved for each of the four weeks.
Each week of the 4-week placebo-free baseline period and the 12-week double-blind treatment period, patients were asked the question, “Please consider how you felt this past week in regard to your IBS, in particular your overall well-being, and symptoms of abdominal discomfort, pain and altered bowel habit. Compared to the way you usually felt before entering the study, how would you rate your relief of symptoms during the past week?” The response variable consisted of the following 5 categories: completely relieved, considerably relieved, somewhat relieved, unchanged, or worse. Patients were classified as responders within a month if they were considerably or completely relieved for at least two of the four weeks, or if they were at least somewhat relieved for each of the four weeks.
* Calculated response rates during month 1 and during month 3 as described above are shown in the table below. The differences in response rates vs. placebo were greater at month 1 than month 3.
: [[File:Tergg 03 Clinical studies.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
Calculated response rates during month 1 and during month 3 as described above are shown in the table below. The differences in response rates vs. placebo were greater at month 1 than month 3.
* Response: ≥ 2 of 4 weeks complete or considerable relief or 4 of 4 weeks with at least somewhat relief.
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
* The same efficacy variable (i.e., complete relief, considerable relief, somewhat relief, unchanged, worse) was analyzed on a weekly basis. The proportion of female patients with complete, considerable or somewhat relief at weeks 1, 4, 6, 8 and 12 are shown in the figure below.
Response: ≥ 2 of 4 weeks complete or considerable relief or 4 of 4 weeks with at least somewhat relief.
: [[File:Terg 03 Cinical studies 02.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
* In addition, individual symptoms of abdominal pain/discomfort and bloating were assessed daily using a 6 or 7 point intensity scale. A positive response was defined as at least a 1 point reduction in the scale. During the first four weeks in the fixed dose studies, 8 to 11% more Zelnorm-treated patients than placebo patients were responders for abdominal pain/discomfort. Similarly, 9 to 12% more tegaserod maleate-treated patients were responders for bloating. Corresponding differences at month 3 were 1 to 10% for abdominal pain/discomfort and 4 to 11% for bloating. Patients on tegaserod maleate also experienced an increase in median number of stools from 3.8/week at baseline to 6.3/week at month 1 and 6.0/week at month 3, while placebo patients increased from 4.0/week to 5.1/week at month 1 and 5.5/week at month 3.
The same efficacy variable (i.e., complete relief, considerable relief, somewhat relief, unchanged, worse) was analyzed on a weekly basis. The proportion of female patients with complete, considerable or somewhat relief at weeks 1, 4, 6, 8 and 12 are shown in the figure below.
* RESULTS IN MEN: In two randomized, placebo-controlled, double-blind studies enrolling 288 males, there were no significant differences between placebo and tegaserod maleate response rates in subgroup analyses by gender.
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
=====Chronic Idiopathic Constipation=====
In addition, individual symptoms of abdominal pain/discomfort and bloating were assessed daily using a 6 or 7 point intensity scale. A positive response was defined as at least a 1 point reduction in the scale. During the first four weeks in the fixed dose studies, 8 to 11% more Zelnorm-treated patients than placebo patients were responders for abdominal pain/discomfort. Similarly, 9 to 12% more Zelnorm-treated patients were responders for bloating. Corresponding differences at month 3 were 1 to 10% for abdominal pain/discomfort and 4 to 11% for bloating. Patients on Zelnorm also experienced an increase in median number of stools from 3.8/week at baseline to 6.3/week at month 1 and 6.0/week at month 3, while placebo patients increased from 4.0/week to 5.1/week at month 1 and 5.5/week at month 3.
* In two multicenter, double-blind, placebo-controlled studies, 2,612 patients with chronic constipation were randomized to receive either tegaserod maleate 6 mg b.i.d., 2 mg b.i.d., or placebo.
* RESULTS IN PATIENTS UNDER AGE 65: A total of 2,281 patients were less than 65 years of age. Patients (91% female, mean age 43 [range 18-64], 90% Caucasian, 4.3% African American) had constipation defined as less than 3 complete spontaneous bowel movements [CSBM] per week and at least one of the following symptoms for at least 25% of defecations: straining, hard/very hard stools, incomplete evacuation. A bowel movement was evaluated by the patient as complete if it resulted in a feeling of complete emptying of their bowel. A bowel movement was considered to be spontaneous [SBM] if no laxatives were taken in the preceding 24 hours. The study population consisted of patients with a 6 month or longer history of constipation symptoms (median 12 years). Patients with constipation known to be due to other known colon diseases, pelvic floor dysfunction, metabolic or neurological disturbances, or concomitant medications were excluded.
RESULTS IN MEN: In two randomized, placebo-controlled, double-blind studies enrolling 288 males, there were no significant differences between placebo and Zelnorm response rates in subgroup analyses by gender.
* After a 2-week baseline, patients were randomized to a 12-week double-blind treatment with tegaserod maleate 6 mg b.i.d., tegaserod maleate 2 mg b.i.d., or placebo. This treatment period was followed, in Study 1, by an extension period where patients received either 6 mg b.i.d. or 2 mg b.i.d. for an additional 13 months. The drop out rate for lack of efficacy for the additional 13-month period was 19% for 6 mg b.i.d. and 22% for 2 mg b.i.d.. In Study 2, the 12-week treatment period was followed by a 4-week drug-free withdrawal period.
* Patients were classified as responders (primary efficacy variable) if they achieved an average increase of at least one CSBM per week during the first four weeks of treatment compared to baseline, and had at least 7 days of exposure in the study.
Chronic Idiopathic Constipation
* The response rate for the primary efficacy variable in patients under 65 years of age was higher in the tegaserod maleate 6 mg b.i.d. group compared to the placebo group for each of the 2 trials (p <0.0001, Table 2). This difference was statistically significant for CSBM changes averaged over the first 4 weeks of treatment and the full 12 weeks of treatment. The results with tegaserod maleate 2 mg b.i.d. showed significant changes during the first 4 weeks, however, no statistically significant changes were observed over 12 weeks in one study.
In two multicenter, double-blind, placebo-controlled studies, 2,612 patients with chronic constipation were randomized to receive either Zelnorm® (tegaserod maleate) 6 mg b.i.d., 2 mg b.i.d., or placebo.
=====Infrequent defecation=====
* At baseline, the median number of CSBM’s per week was zero and the mean number of CSBM’s per week was 0.5. Regardless of baseline, tegaserod maleate significantly increased the number of complete spontaneous bowel movements compared to placebo at each week (p<0.05).
RESULTS IN PATIENTS UNDER AGE 65: A total of 2,281 patients were less than 65 years of age. Patients (91% female, mean age 43 [range 18-64], 90% Caucasian, 4.3% African American) had constipation defined as less than 3 complete spontaneous bowel movements [CSBM] per week and at least one of the following symptoms for at least 25% of defecations: straining, hard/very hard stools, incomplete evacuation. A bowel movement was evaluated by the patient as complete if it resulted in a feeling of complete emptying of their bowel. A bowel movement was considered to be spontaneous [SBM] if no laxatives were taken in the preceding 24 hours. The study population consisted of patients with a 6 month or longer history of constipation symptoms (median 12 years). Patients with constipation known to be due to other known colon diseases, pelvic floor dysfunction, metabolic or neurological disturbances, or concomitant medications were excluded.
* Tegaserod maleate also significantly increased the number of SBM’s compared to placebo at each week (p<0.05).
=====Constipation symptoms=====
After a 2-week baseline, patients were randomized to a 12-week double-blind treatment with Zelnorm 6 mg b.i.d., Zelnorm 2 mg b.i.d., or placebo. This treatment period was followed, in Study 1, by an extension period where patients received either 6 mg b.i.d. or 2 mg b.i.d. for an additional 13 months. The drop out rate for lack of efficacy for the additional 13-month period was 19% for 6 mg b.i.d. and 22% for 2 mg b.i.d.. In Study 2, the 12-week treatment period was followed by a 4-week drug-free withdrawal period.
* Patients treated with tegaserod maleate experienced a statistically significant reduction in the individual symptoms of straining, abdominal distension/bloating, and abdominal discomfort/pain, and a statistically significant improvement in stool consistency and frequency compared to placebo when averaged over the 12 weeks (p<0.05). In addition, a global constipation relief score, computed as an average of 4 scores measuring abdominal discomfort/pain, abdominal distension/bloating, bothersomeness of constipation and satisfaction with bowel habits, showed statistically significant improvement for tegaserod maleate compared to placebo when averaged over the 12 weeks (p<0.05).
* RESULTS IN PATIENTS AGE 65 AND OVER: Subgroup analyses of patients 65 and older (n=331) showed no significant treatment effects for tegaserod maleate over placebo.
Patients were classified as responders (primary efficacy variable) if they achieved an average increase of at least one CSBM per week during the first four weeks of treatment compared to baseline, and had at least 7 days of exposure in the study.
|howSupplied=* tegaserod maleate® (tegaserod maleate) is available as whitish to slightly yellowish, marbled, circular flat tablets with a bevelled edge containing 2 mg or 6 mg tegaserod as follows:
* 2-mg Tablet - white round engraved with “NVR” and “DL”
The response rate for the primary efficacy variable in patients under 65 years of age was higher in the Zelnorm 6 mg b.i.d. group compared to the placebo group for each of the 2 trials (p <0.0001, Table 2). This difference was statistically significant for CSBM changes averaged over the first 4 weeks of treatment and the full 12 weeks of treatment. The results with Zelnorm 2 mg b.i.d. showed significant changes during the first 4 weeks, however, no statistically significant changes were observed over 12 weeks in one study.
* Unit Dose (blister pack)
:* Box of 60 (strips of 10)…………………………………………….NDC 0078-0355-80
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
:* 6-mg Tablet - white round engraved with “NVR” and “EH”
Infrequent defecation
* Unit Dose (blister pack)
:* Box of 60 (strips of 10) ……………………………………………NDC 0078-0356-80
At baseline, the median number of CSBM’s per week was zero and the mean number of CSBM’s per week was 0.5. Regardless of baseline, Zelnorm significantly increased the number of complete spontaneous bowel movements compared to placebo at each week (p<0.05).
:* Bottle of 60………………………………………………………………...NDC 0078-0426-20
: [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]]
Zelnorm also significantly increased the number of SBM’s compared to placebo at each week (p<0.05).
Constipation symptoms
Patients treated with Zelnorm experienced a statistically significant reduction in the individual symptoms of straining, abdominal distension/bloating, and abdominal discomfort/pain, and a statistically significant improvement in stool consistency and frequency compared to placebo when averaged over the 12 weeks (p<0.05). In addition, a global constipation relief score, computed as an average of 4 scores measuring abdominal discomfort/pain, abdominal distension/bloating, bothersomeness of constipation and satisfaction with bowel habits, showed statistically significant improvement for Zelnorm compared to placebo when averaged over the 12 weeks (p<0.05).
RESULTS IN PATIENTS AGE 65 AND OVER: Subgroup analyses of patients 65 and older (n=331) showed no significant treatment effects for Zelnorm over placebo.
|howSupplied=* Zelnorm® (tegaserod maleate) is available as whitish to slightly yellowish, marbled, circular flat tablets with a bevelled edge containing 2 mg or 6 mg tegaserod as follows:
2-mg Tablet - white round engraved with “NVR” and “DL”
Unit Dose (blister pack)
Box of 60 (strips of 10)…………………………………………….NDC 0078-0355-80
6-mg Tablet - white round engraved with “NVR” and “EH”
Unit Dose (blister pack)
Box of 60 (strips of 10) ……………………………………………NDC 0078-0356-80
Bottle of 60………………………………………………………………...NDC 0078-0426-20
|storage=* Store at 25°C (77°F); excursions permitted to 15-30°C (59-86°F).
|storage=* Store at 25°C (77°F); excursions permitted to 15-30°C (59-86°F).
|packLabel=<!--Patient Counseling Information-->
|packLabel=[[File:Terg 06.png|thumb|none|400px|This image is provided by the National Library of Medicine.]]
|alcohol=* Alcohol-{{PAGENAME}} interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
|alcohol=* Alcohol-{{PAGENAME}} interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
<!--Brand Names-->
<!--Brand Names-->
|brandNames=* ZELNORM ®<ref>{{Cite web | title =ZELNORM- tegaserod maleate tablet | url =http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=a274e3ea-bf67-4f81-aaa0-10475b20cd69 }}</ref>
|brandNames=* Zelnorm®<ref>{{Cite web | title =ZELNORM- tegaserod maleate tablet | url =http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=a274e3ea-bf67-4f81-aaa0-10475b20cd69 }}</ref>
<!--Look-Alike Drug Names-->
<!--Look-Alike Drug Names-->
|lookAlike=* A® — B®<ref name="www.ismp.org">{{Cite web | last = | first = | title = http://www.ismp.org | url = http://www.ismp.org | publisher = | date = }}</ref>
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
The safety and effectiveness of Zelnorm in men with IBS with constipation have not been established.
Chronic Idiopathic Constipation
Tegaserod maleate is indicated for the treatment of patients less than 65 years of age with chronic idiopathic constipation. The effectiveness of Zelnorm in patients 65 years or older with chronic idiopathic constipation has not been established.
The efficacy of tegaserod maleate for the treatment of IBS with constipation or chronic idiopathic constipation has not been studied beyond 12 weeks.
IBS with Constipation: The recommended dosage of Tegaserod maleate is 6 mg taken twice daily orally before meals for 4-6 weeks. For those women who respond to therapy at 4-6 weeks, an additional 4-6 week course can be considered.
The recommended dosage of tegaserod maleate is 6 mg taken twice daily orally before meals. :* Physicians and patients should periodically assess the need for continued therapy.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Tegaserod in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Tegaserod in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Tegaserod in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Tegaserod in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Tegaserod in pediatric patients.
Contraindications
Tegaserod maleate is contraindicated in those patients with:
Serious consequences of diarrhea, including hypovolemia, hypotension, and syncope have been reported in the clinical studies and during marketed use of Tegaserod maleate In some cases, these complications have required hospitalization for rehydration. Tegaserod maleate should be discontinued immediately in patients who develop severe diarrhea, hypotension or syncope. tegaserod maleate should not be initiated in patients who are currently experiencing or frequently experience diarrhea.
Adverse Reactions
Clinical Trials Experience
IBS with Constipation
In Phase 3 clinical trials 2,632 female and male patients received Tegaserod maleate 6 mg b.i.d. or placebo. The frequency and type of adverse events for females and males were similar. The following adverse experiences were reported in 1% or more of patients who received tegaserod maleate and occurred more frequently on tegaserod maleate than placebo:
This image is provided by the National Library of Medicine.
Chronic Idiopathic Constipation
In Phase 3 clinical trials 2,603 male and female patients received tegaserod maleate 6 mg b.i.d., 2 mg b.i.d. or placebo. The following adverse experiences were reported in 1% or more of patients who received tegaserod maleate and occurred more frequently than in patients who received placebo.
In the Phase 3 clinical studies, 8.8% of patients receiving tegaserod maleate reported diarrhea as an adverse experience compared to 3.8% of patients receiving placebo. The majority of the tegaserod maleate patients reporting diarrhea had a single episode. In most cases, diarrhea occurred within the first week of treatment. Typically, diarrhea resolved with continued therapy. Overall, the discontinuation rate from the studies due to diarrhea was 1.6% among the tegaserod maleate-treated patients. In clinical studies, a small number of patients (0.04%) experienced clinically significant diarrhea including hospitalization, hypovolemia, hypotension and need for intravenous fluids. Diarrhea can be the pharmacologic response to tegaserod maleate.
Chronic Idiopathic Constipation
In the two Phase 3 studies, 6.6% of patients treated with tegaserod maleate 6 mg b.i.d. and 4.2% of patients treated with tegaserod maleate 2 mg b.i.d. reported diarrhea as an adverse event, versus 3.0% of patients receiving placebo.
The diarrhea episodes experienced by patients treated with tegaserod occurred early after initiation of treatment (median of 5.5 days), were of short duration (median of 2.5 days), and occurred only once in the majority of patient.
Typically, diarrhea resolved with continued therapy; only 0.9% of patients treated with tegaserod maleate 6 mg b.i.d. discontinued the study due to diarrhea (compared to 0.3% in the tegaserod maleate 2 mg b.i.d. group and 0.2% in the placebo group).
Abdominal Surgeries, Including Cholecystectomy
An increase in abdominal surgeries was observed on tegaserod maleate (9/2,965; 0.3%) vs. placebo (3/1,740; 0.2%) in the Phase 3 IBS clinical studies. The increase was primarily due to a numerical imbalance in cholecystectomies reported in patients treated with tegaserod maleate (5/2,965; 0.17%) vs. placebo (1/1,740; 0.06%). In chronic idiopathic constipation clinical trials there was no increase in the frequency of abdominal and pelvic surgeries in active vs. placebo groups: 9/1,752; 0.5% on tegaserod maleate versus 8/861; 0.9% on placebo. A causal relationship between abdominal surgeries and tegaserod maleate has not been established.
Other Adverse Events
The following list of adverse events includes those from Phase 3 clinical studies (6 mg b.i.d. or 2 mg b.i.d.) which were reported more frequently (>0.2%) in patients on tegaserod maleate than placebo; or which were considered by the investigator to be possibly related to tegaserod maleate and reported more frequently (>0.1%) on tegaserod maleate than placebo; or which lead to discontinuation more frequently (≥0.1% and in more than 1 patient) on tegaserod maleate than placebo. The list also contains those serious adverse events from all clinical trials in patients treated with either 6 mg b.i.d. or 2 mg b.i.d. tegaserod maleate which were either considered by the investigator as possibly drug related, or occurred in at least 2 more patients on tegaserod maleate than on placebo. Although the events reported occurred during treatment with tegaserod maleate, they were not necessarily caused by it.
Reproduction studies have been performed in rats at oral doses up to 100 mg/kg/day (approximately 15 times the human exposure at 6 mg b.i.d. based on plasma AUC0-24 hr) and rabbits at oral doses up to 120 mg/kg/day (approximately 51 times the human exposure at 6 mg b.i.d. based on plasma AUC0-24 hr) and have revealed no evidence of impaired fertility or harm to the fetus due to tegaserod. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Tegaserod in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Tegaserod during labor and delivery.
Nursing Mothers
Tegaserod and its metabolites are excreted in the milk of lactating rats with a high milk to plasma ratio. It is not known whether tegaserod is excreted in human milk. Many drugs, which are excreted in human milk, have potential for serious adverse reactions in nursing infants. Based on the potential for tumorigenicity shown for tegaserod in the mouse carcinogenicity study, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
There is no FDA guidance on the use of Tegaserod with respect to pediatric patients.
Geriatic Use
IBS with Constipation
Of 4,035 patients in Phase 3 clinical studies of tegaserod maleate, 290 were at least 65 years of age, while 52 were at least 75 years old. No overall differences in safety were observed between these patients and younger patients with regard to adverse events.
No dose adjustment is necessary when administering tegaserod maleate to patients with IBS with constipation over 65 years old.
Chronic Idiopathic Constipation
Of 2,612 patients in Phase 3 clinical studies of tegaserod maleate, 331 were at least 65 years of age. Efficacy in patients 65 years of age or greater showed no significant difference between drug and placebo responses. Patients 65 years of age or greater who received tegaserod maleate experienced a higher incidence of diarrhea and discontinuations due to diarrhea than patients younger than 65.
Gender
There is no FDA guidance on the use of Tegaserod with respect to specific gender populations.
Race
There is no FDA guidance on the use of Tegaserod with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Tegaserod in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Tegaserod in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Tegaserod in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Tegaserod in patients who are immunocompromised.
There is limited information regarding Monitoring of Tegaserod in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Tegaserod in the drug label.
Overdosage
There have been no reports of human overdosage with tegaserod maleate. Single oral doses of 120 mg of tegaserod were administered to 3 healthy volunteers in 1 study. All 3 subjects developed diarrhea and headache. Two of these subjects also reported intermittent abdominal pain, and 1 developed orthostatic hypotension. In 28 healthy subjects exposed to doses of tegaserod of 90 to 180 mg/d for several days, adverse events were diarrhea (100%), headache (57%), abdominal pain (18%), flatulence (18%), nausea (7%) and vomiting (7%).
Based on the large distribution volume and high protein binding of tegaserod it is unlikely that tegaserod could be removed by dialysis. In cases of overdosage treat symptomatically and institute supportive measures as appropriate.
Pharmacology
This image is provided by the National Library of Medicine.
Mechanism of Action
Irritable bowel syndrome with constipation and chronic idiopathic constipation are both lower gastrointestinal dysmotility disorders. Clinical investigations have shown that both motor and sensory functions of the gut appear to be altered in patients suffering from irritable bowel syndrome (IBS), while in patients with chronic idiopathic constipation, reduced intestinal motility is the predominant cause of the condition. Both the enteric nervous system, which acts to integrate and process information in the gut, and 5-hydroxytryptamine (5-HT, serotonin) are thought to represent key elements in the etiology of both IBS and idiopathic constipation. Approximately 95% of serotonin is found throughout the gastrointestinal tract, primarily stored in enterochromaffin cells but also in enteric nerves acting as a neurotransmitter. Serotonin has been shown to be involved in regulating motility, visceral sensitivity and intestinal secretion. Investigations suggest an important role of serotonin Type-4 (5-HT4) receptors in the maintenance of gastrointestinal functions in humans. 5-HT4 receptor mRNA has been found throughout the human gastrointestinal tract.
Tegaserod is a 5-HT4 receptor partial agonist that binds with high affinity at human 5-HT4 receptors, whereas it has no appreciable affinity for 5-HT3 or dopamine receptors. It has moderate affinity for 5-HT1 receptors. Tegaserod, by acting as an agonist at neuronal 5-HT4 receptors, triggers the release of further neurotransmitters such as calcitonin gene-related peptide from sensory neurons.
The activation of 5-HT4 receptors in the gastrointestinal tract stimulates the peristaltic reflex and intestinal secretion, as well as inhibits visceral sensitivity. In vivo studies showed that tegaserod enhanced basal motor activity and normalized impaired motility throughout the gastrointestinal tract. In addition, studies demonstrated that tegaserod moderated visceral sensitivity during colorectal distension in animals.
Structure
Tegaserod maleate tablets contain tegaserod as the hydrogen maleate salt. As the maleate salt, tegaserod is chemically designated as 3-(5-methoxy-1H-indol-3-ylmethylene)-N-pentylcarbazimidamide hydrogen maleate. Its empirical formula is C16H23N5O•C4H4O4. The molecular weight is 417.47 and the structural formula is
This image is provided by the National Library of Medicine.
Tegaserod as the maleate salt is a white to off-white crystalline powder and is slightly soluble in ethanol and very slightly soluble in water. Each 1.385 mg of tegaserod as the maleate is equivalent to 1 mg of tegaserod. Tegaserod maleate is available for oral use in the following tablet formulations:
2-mg and 6-mg tablets (blister packs) containing 2 mg and 6 mg tegaserod, respectively and the following inactive ingredients: crospovidone, glyceryl monostearate, hypromellose, lactose monohydrate, poloxamer 188, and polyethylene glycol 4000
6-mg tablets (bottles) containing 6 mg tegaserod and the following inactive ingredients: crospovidone, glyceryl behenate, hypromellose, lactose monohydrate, and colloidal silicon dioxide.
Pharmacodynamics
There is limited information regarding Pharmacodynamics of Tegaserod in the drug label.
Pharmacokinetics
Absorption
Peak plasma concentrations are reached approximately 1 hour after oral dosing. The absolute bioavailability of tegaserod when administered to fasting subjects is approximately 10%. The pharmacokinetics are dose proportional over the 2 mg to 12 mg range given twice daily for 5 days. There was no clinically relevant accumulation of tegaserod in plasma when a 6 mg b.i.d. dose was given for 5 days.
Food Effects
When the drug is administered with food, the bioavailability of tegaserod is reduced by 40%-65% and Cmax by approximately 20%-40%. Similar reductions in plasma concentration occur when tegaserod is administered to subjects within 30 minutes prior to a meal, or 2.5 hours after a meal. Tmax of tegaserod is prolonged from approximately 1 hour to 2 hours when taken following a meal, but decreased to 0.7 hours when taken 30 minutes prior to a meal.
Distribution
Tegaserod is approximately 98% bound to plasma proteins, predominantly alpha-1-acid glycoprotein. Tegaserod exhibits pronounced distribution into tissues following intravenous dosing with a volume of distribution at steady-state of 368 ± 223 L.
Metabolism
Tegaserod is metabolized mainly via two pathways. The first is a presystemic acid catalyzed hydrolysis in the stomach followed by oxidation and conjugation which produces the main metabolite of tegaserod, 5-methoxyindole-3-carboxylic acid glucuronide. The main metabolite has negligible affinity for 5-HT4 receptors in vitro. In humans, systemic exposure to tegaserod was not altered at neutral gastric pH values. The second metabolic pathway of tegaserod is direct glucuronidation which leads to generation of three isomeric N-glucuronides.
Elimination
The plasma clearance of tegaserod is 77 ± 15 L/h with an estimated terminal half-life (T1/2) of 11 ± 5 hours following intravenous dosing. Approximately two-thirds of the orally administered dose of tegaserod is excreted unchanged in the feces, with the remaining one-third excreted in the urine, primarily as the main metabolite.
Sub Populations
Patients
The pharmacokinetics of tegaserod in IBS patients are comparable to those in healthy subjects. The pharmacokinetics of tegaserod in patients with chronic idiopathic constipation have not been studied.
Reduced Renal Function: No change in the pharmacokinetics of tegaserod was observed in subjects with severe renal impairment requiring hemodialysis (creatinine clearance <15 mL/min/1.73 m2). Cmax and AUC of the main pharmacologically inactive metabolite of tegaserod, 5-methoxy-indole-3-carboxylic acid glucuronide, increased 2- and 10-fold respectively, in subjects with severe renal impairment compared to healthy controls. No dosage adjustment is required in patients with mild-to-moderate renal impairment. Tegaserod is not recommended in patients with severe renal impairment.
Reduced Hepatic Function
In subjects with mild hepatic impairment, mean AUC was 31% higher and Cmax 16% higher compared to subjects with normal hepatic function. No dosage adjustment is required in patients with mild impairment, however, caution is recommended when using tegaserod in this patient population. Tegaserod has not adequately been studied in patients with moderate and severe hepatic impairment, and is therefore not recommended in these patients.
Gender
Gender has no effect on the pharmacokinetics of tegaserod.
Race
Data were inadequate to assess the effect of race on the pharmacokinetics of tegaserod.
Age
In a clinical pharmacology study conducted to assess the pharmacokinetics of tegaserod administered to healthy young (18-40 years) and healthy elderly (65-85 years) subjects, peak plasma concentration and exposure were 22% and 40% greater, respectively, in elderly females than young females but still within the variability seen in tegaserod pharmacokinetics in healthy subjects. Based on an analysis across several pharmacokinetic studies in healthy subjects, there is no age effect on the pharmacokinetics of tegaserod when allowing for body weight as a covariate. Therefore, dose adjustment in elderly patients who have IBS with constipation is not necessary.
Nonclinical Toxicology
There is limited information regarding Nonclinical Toxicology of Tegaserod in the drug label.
Clinical Studies
IBS with Constipation
RESULTS IN WOMEN: In three multicenter, double-blind, placebo-controlled studies, 2,470 women (mean age 43 years [range 17-89 years]; 86% Caucasian, 10% African American) with at least a 3-month history of IBS symptoms prior to the study baseline period that included abdominal pain, bloating and constipation received either tegaserod maleate® (tegaserod maleate) 6 mg b.i.d. or placebo. In all patients, constipation was characterized by at least two of the following three symptoms each occurring ≥25% of the time over a 3-month period:< 3 bowel movements/week, hard or lumpy stools, or straining with a bowel movement. The study design consisted of a 4-week placebo-free baseline period followed by a 12-week double-blind treatment period. Study 1 and 2 evaluated a fixed dose regimen of tegaserod 6 mg b.i.d. while Study 3 utilized a dose-titration design.
Each week of the 4-week placebo-free baseline period and the 12-week double-blind treatment period, patients were asked the question, “Please consider how you felt this past week in regard to your IBS, in particular your overall well-being, and symptoms of abdominal discomfort, pain and altered bowel habit. Compared to the way you usually felt before entering the study, how would you rate your relief of symptoms during the past week?” The response variable consisted of the following 5 categories: completely relieved, considerably relieved, somewhat relieved, unchanged, or worse. Patients were classified as responders within a month if they were considerably or completely relieved for at least two of the four weeks, or if they were at least somewhat relieved for each of the four weeks.
Calculated response rates during month 1 and during month 3 as described above are shown in the table below. The differences in response rates vs. placebo were greater at month 1 than month 3.
This image is provided by the National Library of Medicine.
Response: ≥ 2 of 4 weeks complete or considerable relief or 4 of 4 weeks with at least somewhat relief.
The same efficacy variable (i.e., complete relief, considerable relief, somewhat relief, unchanged, worse) was analyzed on a weekly basis. The proportion of female patients with complete, considerable or somewhat relief at weeks 1, 4, 6, 8 and 12 are shown in the figure below.
This image is provided by the National Library of Medicine.
In addition, individual symptoms of abdominal pain/discomfort and bloating were assessed daily using a 6 or 7 point intensity scale. A positive response was defined as at least a 1 point reduction in the scale. During the first four weeks in the fixed dose studies, 8 to 11% more Zelnorm-treated patients than placebo patients were responders for abdominal pain/discomfort. Similarly, 9 to 12% more tegaserod maleate-treated patients were responders for bloating. Corresponding differences at month 3 were 1 to 10% for abdominal pain/discomfort and 4 to 11% for bloating. Patients on tegaserod maleate also experienced an increase in median number of stools from 3.8/week at baseline to 6.3/week at month 1 and 6.0/week at month 3, while placebo patients increased from 4.0/week to 5.1/week at month 1 and 5.5/week at month 3.
RESULTS IN MEN: In two randomized, placebo-controlled, double-blind studies enrolling 288 males, there were no significant differences between placebo and tegaserod maleate response rates in subgroup analyses by gender.
Chronic Idiopathic Constipation
In two multicenter, double-blind, placebo-controlled studies, 2,612 patients with chronic constipation were randomized to receive either tegaserod maleate 6 mg b.i.d., 2 mg b.i.d., or placebo.
RESULTS IN PATIENTS UNDER AGE 65: A total of 2,281 patients were less than 65 years of age. Patients (91% female, mean age 43 [range 18-64], 90% Caucasian, 4.3% African American) had constipation defined as less than 3 complete spontaneous bowel movements [CSBM] per week and at least one of the following symptoms for at least 25% of defecations: straining, hard/very hard stools, incomplete evacuation. A bowel movement was evaluated by the patient as complete if it resulted in a feeling of complete emptying of their bowel. A bowel movement was considered to be spontaneous [SBM] if no laxatives were taken in the preceding 24 hours. The study population consisted of patients with a 6 month or longer history of constipation symptoms (median 12 years). Patients with constipation known to be due to other known colon diseases, pelvic floor dysfunction, metabolic or neurological disturbances, or concomitant medications were excluded.
After a 2-week baseline, patients were randomized to a 12-week double-blind treatment with tegaserod maleate 6 mg b.i.d., tegaserod maleate 2 mg b.i.d., or placebo. This treatment period was followed, in Study 1, by an extension period where patients received either 6 mg b.i.d. or 2 mg b.i.d. for an additional 13 months. The drop out rate for lack of efficacy for the additional 13-month period was 19% for 6 mg b.i.d. and 22% for 2 mg b.i.d.. In Study 2, the 12-week treatment period was followed by a 4-week drug-free withdrawal period.
Patients were classified as responders (primary efficacy variable) if they achieved an average increase of at least one CSBM per week during the first four weeks of treatment compared to baseline, and had at least 7 days of exposure in the study.
The response rate for the primary efficacy variable in patients under 65 years of age was higher in the tegaserod maleate 6 mg b.i.d. group compared to the placebo group for each of the 2 trials (p <0.0001, Table 2). This difference was statistically significant for CSBM changes averaged over the first 4 weeks of treatment and the full 12 weeks of treatment. The results with tegaserod maleate 2 mg b.i.d. showed significant changes during the first 4 weeks, however, no statistically significant changes were observed over 12 weeks in one study.
Infrequent defecation
At baseline, the median number of CSBM’s per week was zero and the mean number of CSBM’s per week was 0.5. Regardless of baseline, tegaserod maleate significantly increased the number of complete spontaneous bowel movements compared to placebo at each week (p<0.05).
Tegaserod maleate also significantly increased the number of SBM’s compared to placebo at each week (p<0.05).
Constipation symptoms
Patients treated with tegaserod maleate experienced a statistically significant reduction in the individual symptoms of straining, abdominal distension/bloating, and abdominal discomfort/pain, and a statistically significant improvement in stool consistency and frequency compared to placebo when averaged over the 12 weeks (p<0.05). In addition, a global constipation relief score, computed as an average of 4 scores measuring abdominal discomfort/pain, abdominal distension/bloating, bothersomeness of constipation and satisfaction with bowel habits, showed statistically significant improvement for tegaserod maleate compared to placebo when averaged over the 12 weeks (p<0.05).
RESULTS IN PATIENTS AGE 65 AND OVER: Subgroup analyses of patients 65 and older (n=331) showed no significant treatment effects for tegaserod maleate over placebo.
How Supplied
tegaserod maleate® (tegaserod maleate) is available as whitish to slightly yellowish, marbled, circular flat tablets with a bevelled edge containing 2 mg or 6 mg tegaserod as follows:
2-mg Tablet - white round engraved with “NVR” and “DL”
Unit Dose (blister pack)
Box of 60 (strips of 10)…………………………………………….NDC 0078-0355-80
6-mg Tablet - white round engraved with “NVR” and “EH”
Unit Dose (blister pack)
Box of 60 (strips of 10) ……………………………………………NDC 0078-0356-80
Bottle of 60………………………………………………………………...NDC 0078-0426-20
Storage
Store at 25°C (77°F); excursions permitted to 15-30°C (59-86°F).
Images
Drug Images
{{#ask: Page Name::Tegaserod
|?Pill Name
|?Drug Name
|?Pill Ingred
|?Pill Imprint
|?Pill Dosage
|?Pill Color
|?Pill Shape
|?Pill Size (mm)
|?Pill Scoring
|?NDC
|?Drug Author
|format=template
|template=DrugPageImages
|mainlabel=-
|sort=Pill Name
}}
Package and Label Display Panel
This image is provided by the National Library of Medicine.
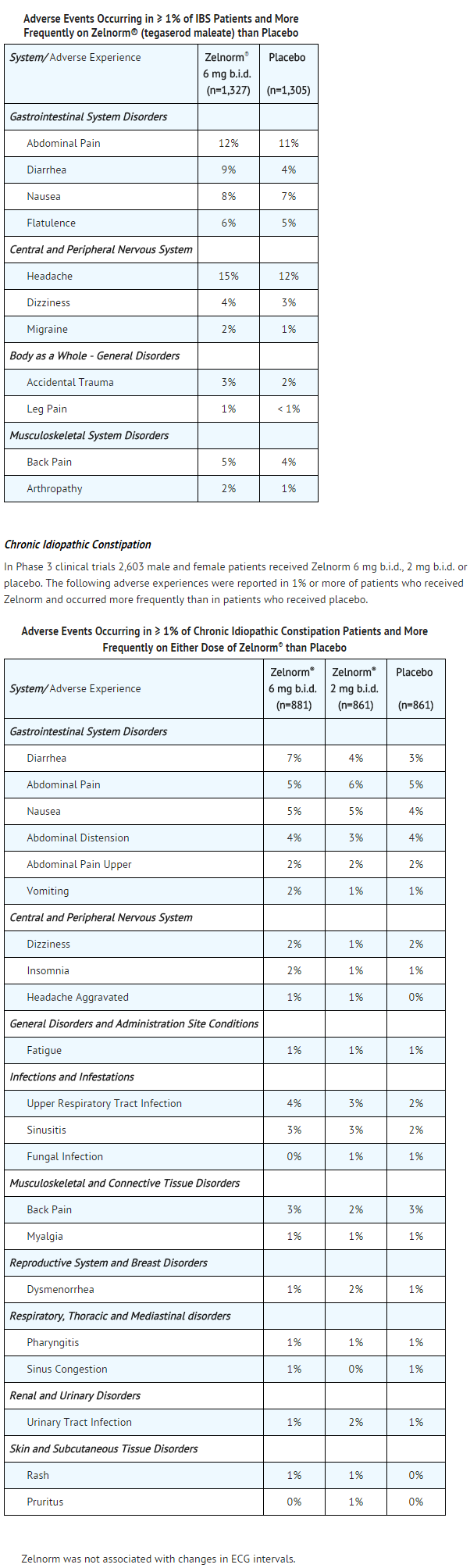

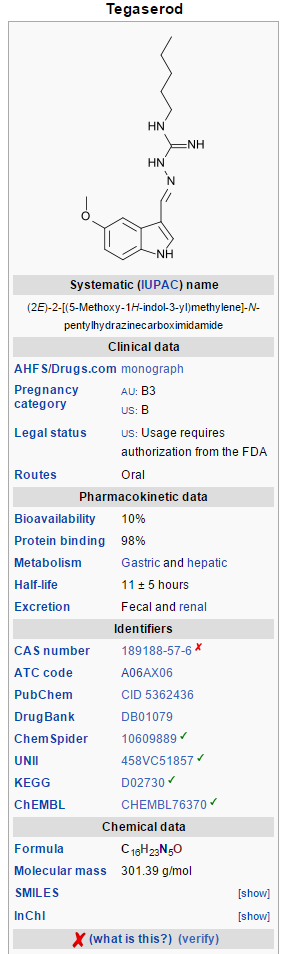

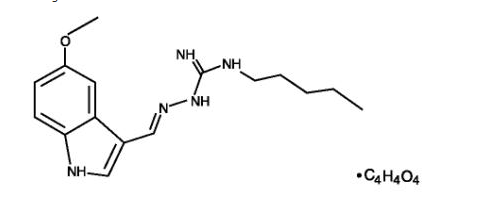

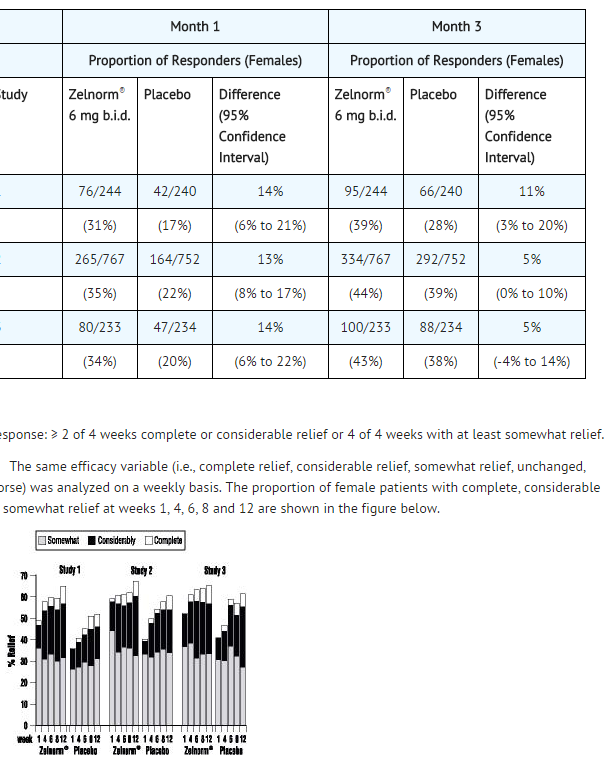

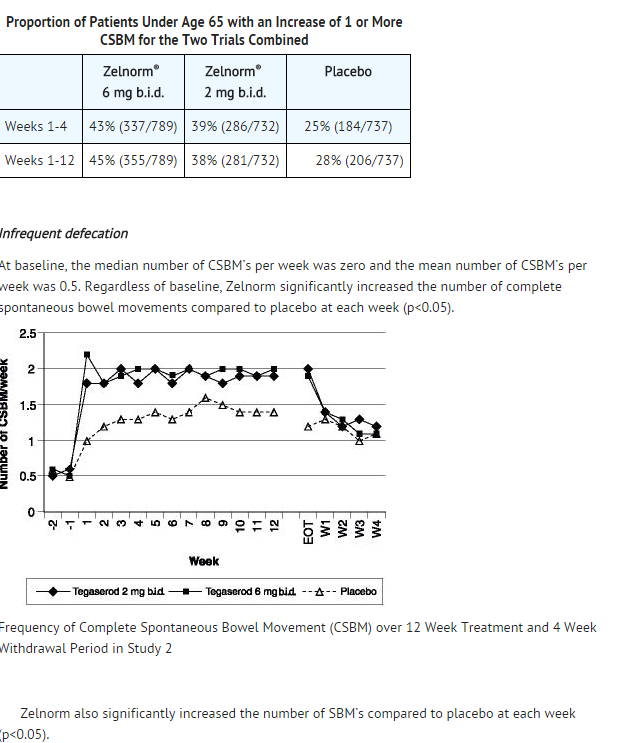

{kind=link}
