Squamous cell carcinoma of the skin pathophysiology: Difference between revisions
No edit summary |
No edit summary |
||
| Line 12: | Line 12: | ||
Although poorly differentiated tumors tend to behave more aggressively, well-differentiated tumors can also give rise to metastasis and result in death. Several histologic variants of squamous cell carcinoma have been documented, including verrucous, spindle cell and pseudovascular. | Although poorly differentiated tumors tend to behave more aggressively, well-differentiated tumors can also give rise to metastasis and result in death. Several histologic variants of squamous cell carcinoma have been documented, including verrucous, spindle cell and pseudovascular. | ||
Frequently an actinic keratosis or squamous cell carcinoma overlies the invasive component and the two are focally contiguous. Occasionally squamous tumors arise rapidly, have a crater-form morphology and spontaneously regress. These tumors are known as keratoacanthomas. Some craterform squamous lesions do not regress, but continue to invade and grow and represent invasive squamous cell carcinomas. | Frequently an actinic keratosis or squamous cell carcinoma overlies the invasive component and the two are focally contiguous. Occasionally squamous tumors arise rapidly, have a crater-form morphology and spontaneously regress. These tumors are known as keratoacanthomas. Some craterform squamous lesions do not regress, but continue to invade and grow and represent invasive squamous cell carcinomas. | ||
'''<u>Skin</u>''' | |||
Persons who present with Squamous cell carcinoma of skin may have one of the following risk factors like | |||
* significant sun exposure | |||
* benign lesions like Chalazion | |||
* chronic ulcers. | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:squamous cell skin cancer.jpg|Squamous cell skin cancer.<ref>http://picasaweb.google.com/mcmumbi/USMLEIIImages</ref> | |||
Image:Squamous cell carcinoma oral 003.jpg|Squamous cell carcinoma in oral cavity. <br> <small> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> | |||
Image:AuricleMelanoma SqCC.jpg|This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma <ref>http://www.ghorayeb.com</ref>. | |||
</gallery> | |||
</div> | |||
<u>Presentation</u> : They usually notice plaque. Ulcers are commonly seen over the face causing disfiguration. At times they can be exophytic over the lips etc. | |||
'''<u>Tongue and Esophagus</u>''' | |||
Persons who present with Squamous cell carcinoma of tongue and esophagus are most likely to have following risk factor | |||
* Tobacco chewing/smoking | |||
* Alcohol Abuse | |||
* Poor dental hygiene | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Squamous cell carcinoma oral 001.jpg|Squamous cell carcinoma in oral cavity. <br> <small> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> | |||
Image:Squamous_cell_carcinoma.jpg|A large squamous cell carcinoma of the tongue<ref>http://picasaweb.google.com/mcmumbi/USMLEIIImages</ref> | |||
</gallery> | |||
</div> | |||
<u>Presentation</u> : Its usually ulcerated in the lateral part of the tongue, pink - red color. Patient finds tough to eat or swallow. As it bleeds on touch or biting. They have dysphagia/ odynophagia when esophagus is involved. In later stages even liquids are tough to go thru. Swelling of lymph nodes is seen in advanced stages where we can find lumps in the neck | |||
'''<u>Nasopharynx</u>''' | |||
Persons who have SCC of this region seldom have any risk factors. It most of the times caused by EBV infection. | |||
<u>Presentation</u> : Patient presents with symptoms from the mass effect of the tumour. They include nasal discharge, bleeding, obstruction; ear infection, deafness , tinnitus are complained. Other important complaints include headache and neck swelling due to lymph nodal spread.<ref>Sham JS, Poon YF, Wei WI, Choy D. Nasopharyngeal carcinoma in young patients. Cancer. Jun 1 1990;65(11):2606-10.</ref> | |||
'''<u>Lungs</u>''' | |||
Persons who have SCC of lungs usually have risk factors like | |||
* Therapeutic radiation (PUVA for psoriais) | |||
* Tobacco smoking | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Oral cancer (1) squamous cell carcinoma histopathology.jpg|[[Biopsy]] of a highly differentiated squamous cell carcinoma of the mouth.[[H&E stain|Haematoxylin & eosin stain]]. | |||
Image:Ca bronchus.jpg|Photograph of a squamous cell carcinoma. Tumour is on the left, obstructing the bronchus (lung). Beyond the tumour the bronchus is inflammed and contains mucus | |||
</gallery> | |||
</div> | |||
<u>Presentation</u> : Persons who present with SCC of lungs doesn't present usually with any typical symptoms of pulmonary. But in few we may see persistent cough, hemoptysis when it is exophytic and occupies whole of the bronchi which can even lead to recurrent infections. | |||
'''<u>Penis</u>''' | |||
Persons who present with Squamous cell carcinoma of penis are most likely to have | |||
* Pre-malignanat lesions ([[Bowen's disease]], [[Condyloma]] , [[Warts]]) | |||
* Smoking and tobacco chewing | |||
<u>Presentation</u> : Unhealed lesions, subtle indurations may be the intial presentation. Often presentation to the clinic is delayed due to embarrassment most of the times. Warts can be a pre-disposing factor.Large warts lead to infections and necrosis leading to hemorrhages at times. | |||
<u>'''Others'''</u> | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Head_oral_scc2.jpg|Squamous Cell Cancer of the Mouth: Cancer that began along the lower gum line has spread to left submandibular lymph nodes. | |||
Image:Head_oral_scc3.jpg|Squamous Cell Cancer of the Mouth: Cancer that began along the lower gum line has spread to left submandibular lymph nodes. | |||
</gallery> | |||
</div> | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Auriclesqccastellateexcision.jpg|Recurrent squamous cell carcinoma of the auricle (far left) excised with a stellate incision across the antihelix. | |||
Image:Auricle003.jpg|The final result of the excision. | |||
</gallery> | |||
</div> | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Squamous cell carcinoma of prostate.jpg|Prostate: Squamous cell carcinoma | |||
Image:Squamous cell carcinoma of prostate 2.jpg|Prostate: Squamous cell carcinoma | |||
</gallery> | |||
</div> | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Head oral scc.jpg|Squamous Cell Cancer of the Mouth: Irregular, necrotic appearing tissue on the inside of the mouth due to extensive squamous cell cancer. Patient has limited ability to open his mouth (aka trismus) as a result of the infiltrating cancer. | |||
Image:head_oral_scc1.jpg|Squamous Cell Cancer, Base of Tongue: Note white area with swelling, right base of tongue. | |||
Image:Squamous cell carcinoma oral 002.jpg|Squamous cell carcinoma in oral cavity. <br> <small> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> | |||
</gallery> | |||
</div> | |||
=== Cervix: Squamous cell carcinoma=== | |||
{{#ev:youtube|zB47nE-i8dQ}} | |||
{{#ev:youtube|J3kULzKGzws}} | |||
==References== | ==References== | ||
Revision as of 15:47, 28 August 2012
|
Squamous cell carcinoma of the skin Microchapters |
|
Differentiating Squamous cell carcinoma of the skin from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Squamous cell carcinoma of the skin pathophysiology On the Web |
|
American Roentgen Ray Society Images of Squamous cell carcinoma of the skin pathophysiology |
|
Squamous cell carcinoma of the skin pathophysiology in the news |
|
Blogs on Squamous cell carcinoma of the skin pathophysiology |
|
Directions to Hospitals Treating Squamous cell carcinoma of the skin |
|
Risk calculators and risk factors for Squamous cell carcinoma of the skin pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aditya Govindavarjhulla, M.B.B.S. [2], Raviteja Guddeti, M.B.B.S. [3]
Overview
Squamous cell carcinoma (SCC) is type of non-melanoma skin cancer. The cancer arises as a result of uncontrolled growth of the squamous cells in the epidermis of the skin. Unlike it's counter part, the basal cell carcinoma which also belongs to the group of non-melanoma cancer, SCC is rapid growing and invasive. SCCs may occur on all areas of the body including the mucous membranes and genitals, but are most common in areas frequently exposed to the sun, such as the rim of the ear, lower lip, face, bald scalp, neck, hands, arms and legs. Wrinkling, changes in pigmentation, and loss of elasticity of the skin are often the telltale signs of sun damage
Pathophysiology
Squamous cell carcinoma is a potentially invasive cancer that arises from the surface epithelium.The development of squamous cell carcinoma is frequently a multistep process. Early lesions tend to be either actinic keratoses, with atypia of the basal keratinocytic layer of the epidermis or squamous cell carcinoma in situ, in which keratinocytic atypia spans the full thickness epidermis.
These precursors are frequently present adjacent to invasive squamous cell carcinomas which invade the dermis as nests, islands, or cords squamous cells with or occasionally as individual cells. Several grading schemes have been developed for squamous cell carcinoma and incorporate the extent of keratinization (a form of differentiation) and nuclear atypia. A widely used scheme divides tumors into well, moderately, or poorly differentiated.
Although poorly differentiated tumors tend to behave more aggressively, well-differentiated tumors can also give rise to metastasis and result in death. Several histologic variants of squamous cell carcinoma have been documented, including verrucous, spindle cell and pseudovascular.
Frequently an actinic keratosis or squamous cell carcinoma overlies the invasive component and the two are focally contiguous. Occasionally squamous tumors arise rapidly, have a crater-form morphology and spontaneously regress. These tumors are known as keratoacanthomas. Some craterform squamous lesions do not regress, but continue to invade and grow and represent invasive squamous cell carcinomas.
Skin
Persons who present with Squamous cell carcinoma of skin may have one of the following risk factors like
- significant sun exposure
- benign lesions like Chalazion
- chronic ulcers.
-
![Squamous cell skin cancer.[1]](/images/1/17/Squamous_cell_skin_cancer.jpg)
Squamous cell skin cancer.[1]
-

Squamous cell carcinoma in oral cavity.
Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology -
![This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma [2].](/images/f/f4/AuricleMelanoma_SqCC.jpg)
This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma [2].
![Squamous cell skin cancer.[1]](/index.php/File:Squamous_cell_skin_cancer.jpg)

![This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma [2].](/index.php/File:AuricleMelanoma_SqCC.jpg)
Presentation : They usually notice plaque. Ulcers are commonly seen over the face causing disfiguration. At times they can be exophytic over the lips etc.
Tongue and Esophagus
Persons who present with Squamous cell carcinoma of tongue and esophagus are most likely to have following risk factor
- Tobacco chewing/smoking
- Alcohol Abuse
- Poor dental hygiene
-

Squamous cell carcinoma in oral cavity.
Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology -
![A large squamous cell carcinoma of the tongue[3]](/images/e/e9/Squamous_cell_carcinoma.jpg)
A large squamous cell carcinoma of the tongue[3]

![A large squamous cell carcinoma of the tongue[3]](/index.php/File:Squamous_cell_carcinoma.jpg)
Presentation : Its usually ulcerated in the lateral part of the tongue, pink - red color. Patient finds tough to eat or swallow. As it bleeds on touch or biting. They have dysphagia/ odynophagia when esophagus is involved. In later stages even liquids are tough to go thru. Swelling of lymph nodes is seen in advanced stages where we can find lumps in the neck
Nasopharynx
Persons who have SCC of this region seldom have any risk factors. It most of the times caused by EBV infection.
Presentation : Patient presents with symptoms from the mass effect of the tumour. They include nasal discharge, bleeding, obstruction; ear infection, deafness , tinnitus are complained. Other important complaints include headache and neck swelling due to lymph nodal spread.[4]
Lungs
Persons who have SCC of lungs usually have risk factors like
- Therapeutic radiation (PUVA for psoriais)
- Tobacco smoking
-
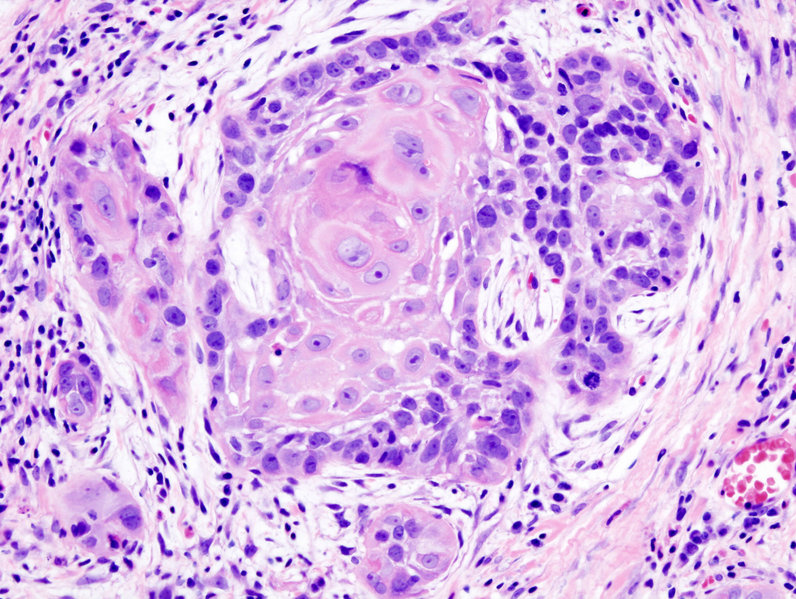
Biopsy of a highly differentiated squamous cell carcinoma of the mouth.Haematoxylin & eosin stain.
-

Photograph of a squamous cell carcinoma. Tumour is on the left, obstructing the bronchus (lung). Beyond the tumour the bronchus is inflammed and contains mucus
_squamous_cell_carcinoma_histopathology.jpg)

Presentation : Persons who present with SCC of lungs doesn't present usually with any typical symptoms of pulmonary. But in few we may see persistent cough, hemoptysis when it is exophytic and occupies whole of the bronchi which can even lead to recurrent infections.
Penis
Persons who present with Squamous cell carcinoma of penis are most likely to have
- Pre-malignanat lesions (Bowen's disease, Condyloma , Warts)
- Smoking and tobacco chewing
Presentation : Unhealed lesions, subtle indurations may be the intial presentation. Often presentation to the clinic is delayed due to embarrassment most of the times. Warts can be a pre-disposing factor.Large warts lead to infections and necrosis leading to hemorrhages at times.
Others
-

Squamous Cell Cancer of the Mouth: Cancer that began along the lower gum line has spread to left submandibular lymph nodes.
-

Squamous Cell Cancer of the Mouth: Cancer that began along the lower gum line has spread to left submandibular lymph nodes.


-
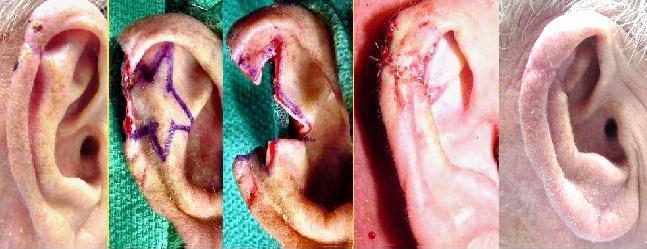
Recurrent squamous cell carcinoma of the auricle (far left) excised with a stellate incision across the antihelix.
-

The final result of the excision.


-

Prostate: Squamous cell carcinoma
-
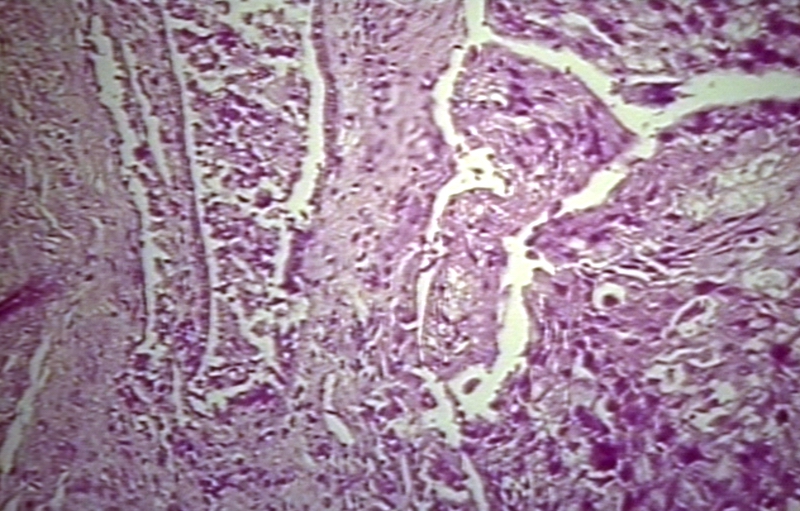
Prostate: Squamous cell carcinoma


-
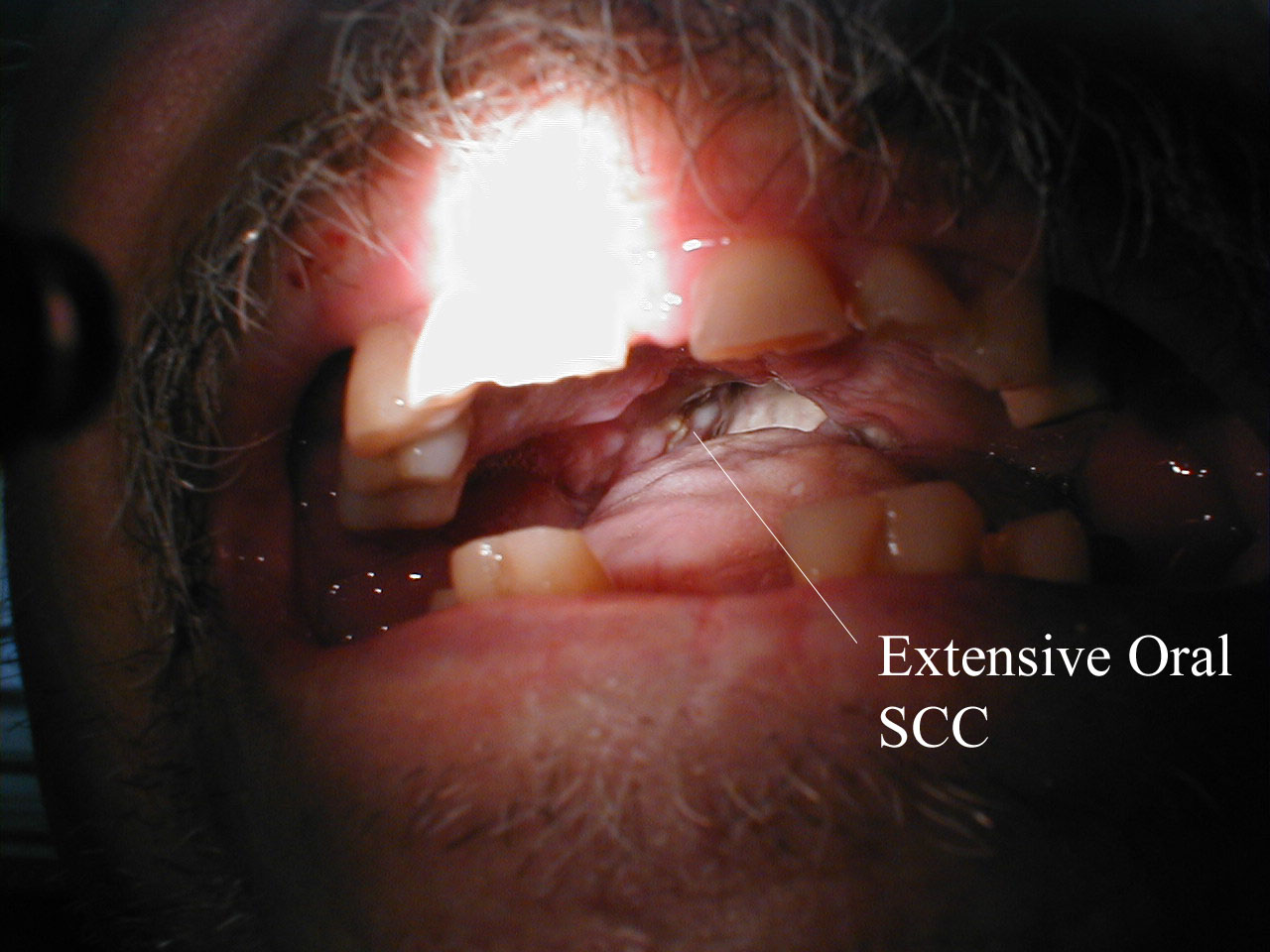
Squamous Cell Cancer of the Mouth: Irregular, necrotic appearing tissue on the inside of the mouth due to extensive squamous cell cancer. Patient has limited ability to open his mouth (aka trismus) as a result of the infiltrating cancer.
-

Squamous Cell Cancer, Base of Tongue: Note white area with swelling, right base of tongue.
-

Squamous cell carcinoma in oral cavity.
Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology



Cervix: Squamous cell carcinoma
{{#ev:youtube|zB47nE-i8dQ}}
{{#ev:youtube|J3kULzKGzws}}
References
- ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ http://www.ghorayeb.com
- ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ Sham JS, Poon YF, Wei WI, Choy D. Nasopharyngeal carcinoma in young patients. Cancer. Jun 1 1990;65(11):2606-10.