Squamous cell carcinoma clinical features: Difference between revisions
No edit summary |
No edit summary |
||
| (10 intermediate revisions by 3 users not shown) | |||
| Line 1: | Line 1: | ||
{{Squamous cell carcinoma}} | {{Squamous cell carcinoma}} | ||
{{CMG}}; '''Associate Editor(s)-in-Chief:''' [[User:Aditya Govindavarjhulla|Aditya Govindavarjhulla, M.B.B.S.]] [mailto:agovi@ | {{CMG}}; '''Associate Editor(s)-in-Chief:''' [[User:Aditya Govindavarjhulla|Aditya Govindavarjhulla, M.B.B.S.]] [mailto:agovi@wikidoc.org], [[User:Raviteja Reddy Guddeti|Raviteja Guddeti, M.B.B.S.]] [mailto:ravitheja.g@gmail.com] | ||
== Overview == | == Overview == | ||
The majority of squamous cell carcinomas arise on the sun-exposed areas of the skin on the head and neck, with fewer lesions arising on the extremities and the trunk. The early lesions of squamous cell carcinoma frequently present as a red, scaly spots while later lesions may form nodules or firm plaques, either of which can ulcerate ( http://tray.dermatology.uiowa.edu). Diagnosis is established by performing a biopsy and the obtaining histopathological confirmation. Complete excision is curative in the vast majority of cases, however occasionally squamous cell carcinoma will invade along the perineural layer of peripheral nerves and will extend well beyond the clinically apparent mass. Local recurrence is more common in these instances and when occurring on the head, may cause direct intracranial extension. Metastases to draining lymph nodes occurs in a minority of cases and disseminated disease is the cause of most squamous cell carcinoma-related deaths. Higher rates of metastasis (~15%) are observed with primary lesions of the lips or ears (Rowe et al., 1992). Radiation therapy is helpful in some cases of locally recurrent disease in which complete resection is difficult to achieve. | |||
== History / Presenting complaints == | == History / Presenting complaints == | ||
Squamous cell carcinoma is often easy to visualize on the body, as it most often occurs in fairly exposed areas of the body such as the face, ears, neck and arms. It is a slow growing tumor, and its presentation usually depends on the part of the body that is involved. It may vary in appearance from a simple growing lump, a plaque or a bleeding ulcer.<ref>www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001832/</ref> | |||
Systemic symptoms of this carcinoma are seen in the advanced stages where the cancer disseminates | Systemic symptoms of this carcinoma are seen in the advanced stages where the cancer disseminates. Usually, the only systemic symptom is easy fatiguability, however certain symptoms such as dysphagia and odynophagia are seen when the tongue, lips, or esophagus are involved. | ||
'''<u>Skin</u>''' | '''<u>Skin</u>''' | ||
Persons who present with | Persons who present with squamous cell carcinoma of skin may have one of the following risk factors; | ||
* | * Significant sun exposure | ||
* | * Benign lesions such as chalazion | ||
* | * Chronic ulcers | ||
<div align="left"> | <div align="left"> | ||
<gallery heights="175" widths="175"> | <gallery heights="175" widths="175"> | ||
Image:squamous cell skin cancer.jpg|Squamous cell skin cancer.<ref>http://picasaweb.google.com/mcmumbi/USMLEIIImages</ref> | Image:squamous cell skin cancer.jpg|Squamous cell skin cancer.<ref>http://picasaweb.google.com/mcmumbi/USMLEIIImages</ref> | ||
Image:Squamous cell carcinoma oral 003.jpg|Squamous cell carcinoma in oral cavity. <br> <small> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> | Image:Squamous cell carcinoma oral 003.jpg|Squamous cell carcinoma in the oral cavity. <br> <small> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> | ||
Image:AuricleMelanoma SqCC.jpg|This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma <ref>http://www.ghorayeb.com</ref>. | Image:AuricleMelanoma SqCC.jpg|This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma <ref>http://www.ghorayeb.com</ref>. | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
<u>Presentation</u> : | <u>Presentation</u> : Plaques and ulcers are commonly seen over the face causing disfiguration, and can be exophytic over the lips. | ||
'''<u>Tongue and Esophagus</u>''' | '''<u>Tongue and Esophagus</u>''' | ||
Persons who present with | Persons who present with squamous cell carcinoma of tongue and esophagus are likely to have following risk factors; | ||
* Tobacco chewing | * Tobacco chewing or smoking | ||
* Alcohol | * Alcohol abuse | ||
* Poor dental hygiene | * Poor dental hygiene | ||
| Line 47: | Line 46: | ||
</div> | </div> | ||
<u>Presentation</u> : | <u>Presentation</u> : It usually presents as an ulceration on the lateral aspect of the tongue, which is pink to red in color. The patient will often find it tough to eat or swallow as a result of the lesion. Involvement of the throat and esophagus leads to symptoms of dysphagia and odynophagia, first to solids, and then in later stages to liquids also. Swelling of lymph nodes presenting as lumps in the neck will often occur in later stages of cancer. | ||
'''<u>Nasopharynx</u>''' | '''<u>Nasopharynx</u>''' | ||
Persons who have SCC of this region seldom have any risk factors. It | Persons who have SCC of this region seldom have any known risk factors. It is usually caused by infection with Epstein-Barr virus. | ||
<u>Presentation</u> : | <u>Presentation</u> : This patient presented with symptoms from the mass effect of the tumor. Symptoms included nasal discharge, bleeding from the nose, and nasal obstruction. Other complaints included ear infection, deafness, tinnitus, headache, and neck swelling.<ref>Sham JS, Poon YF, Wei WI, Choy D. Nasopharyngeal carcinoma in young patients. Cancer. Jun 1 1990;65(11):2606-10.</ref> | ||
'''<u>Lungs</u>''' | '''<u>Lungs</u>''' | ||
Persons who have SCC of lungs usually have risk factors | Persons who have SCC of lungs usually have the following risk factors in their history; | ||
* Therapeutic radiation (PUVA for psoriais) | * Therapeutic radiation (PUVA for psoriais) | ||
| Line 65: | Line 64: | ||
<gallery heights="175" widths="175"> | <gallery heights="175" widths="175"> | ||
Image:Oral cancer (1) squamous cell carcinoma histopathology.jpg|[[Biopsy]] of a highly differentiated squamous cell carcinoma of the mouth.[[H&E stain|Haematoxylin & eosin stain]]. | Image:Oral cancer (1) squamous cell carcinoma histopathology.jpg|[[Biopsy]] of a highly differentiated squamous cell carcinoma of the mouth.[[H&E stain|Haematoxylin & eosin stain]]. | ||
Image:Ca bronchus.jpg|Photograph of a squamous cell carcinoma. | Image:Ca bronchus.jpg|Photograph of a squamous cell carcinoma. Tumor is on the left, obstructing the bronchus with inflammation and mucus accumulation in the bronchus. | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
<u>Presentation</u> : Persons who present with | <u>Presentation</u> : Persons who present with squamous cell carcinoma of the lungs typically do not present with pulmonary symptoms. However if the cancer is exophytic and occupies the bronchi, persistent cough, hemoptysis, and recurrent infections may be seen. | ||
'''<u>Penis</u>''' | '''<u>Penis</u>''' | ||
Persons who present with Squamous cell carcinoma of penis are most likely to have | Persons who present with Squamous cell carcinoma of penis are most likely to have a history of; | ||
* Pre- | * Pre-malignant lesions ([[Bowen's disease]], [[Condyloma]] , [[Warts]]) | ||
* Smoking and tobacco chewing | * Smoking and tobacco chewing | ||
<u>Presentation</u> : Unhealed lesions | <u>Presentation</u> : Unhealed lesions and subtle indurations may be the intial presentation. Warts can often be a predisposing factor, and large warts can lead to infection and necrosis, occasionally causing hemorrhage. | ||
<u>'''others'''</u> | <u>'''others'''</u> | ||
| Line 85: | Line 84: | ||
<div align="left"> | <div align="left"> | ||
<gallery heights="175" widths="175"> | <gallery heights="175" widths="175"> | ||
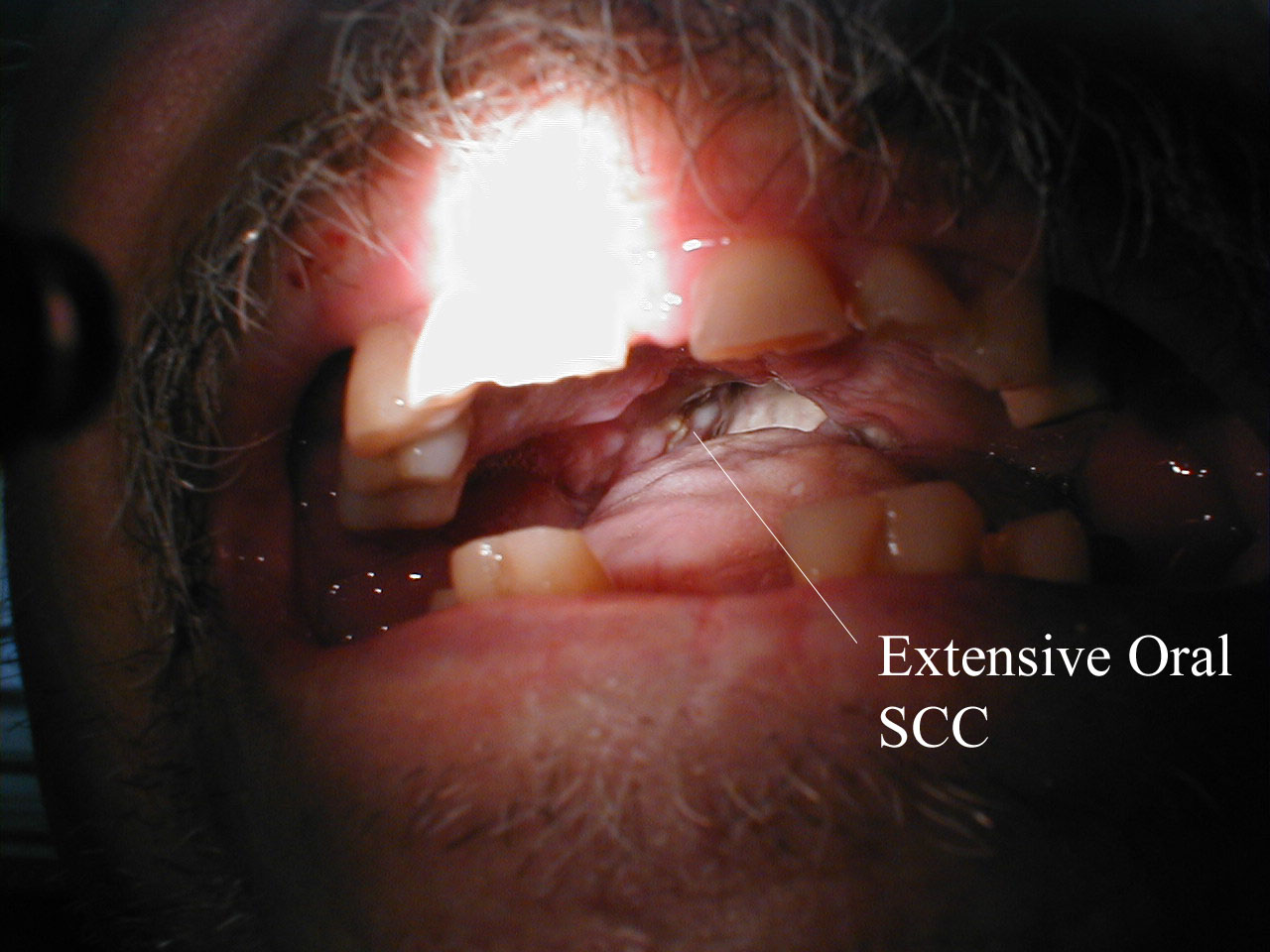
Image:Head_oral_scc2.jpg|Squamous Cell Cancer of the Mouth: Cancer that | Image:Head_oral_scc2.jpg|Squamous Cell Cancer of the Mouth: Cancer that originated along the lower gum line, leading to spread along the left submandibular lymph nodes. | ||
Image:Head_oral_scc3.jpg|Squamous Cell Cancer of the Mouth: Cancer that | Image:Head_oral_scc3.jpg|Squamous Cell Cancer of the Mouth: Cancer that originated along the lower gum line, leading to spread along the left submandibular lymph nodes. | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
| Line 94: | Line 93: | ||
<gallery heights="175" widths="175"> | <gallery heights="175" widths="175"> | ||
Image:Auriclesqccastellateexcision.jpg|Recurrent squamous cell carcinoma of the auricle (far left) excised with a stellate incision across the antihelix<ref>http://www.ghorayeb.com</ref>. | Image:Auriclesqccastellateexcision.jpg|Recurrent squamous cell carcinoma of the auricle (far left) excised with a stellate incision across the antihelix<ref>http://www.ghorayeb.com</ref>. | ||
Image:Auricle003.jpg| | Image:Auricle003.jpg|Final result of the excision<ref>http://www.ghorayeb.com</ref>. | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
| Line 101: | Line 100: | ||
<div align="left"> | <div align="left"> | ||
<gallery heights="175" widths="175"> | <gallery heights="175" widths="175"> | ||
Image:Squamous cell carcinoma of prostate.jpg|Prostate: Squamous cell carcinoma | Image:Squamous cell carcinoma of the prostate.jpg|Prostate: Squamous cell carcinoma | ||
Image:Squamous cell carcinoma of prostate 2.jpg|Prostate: Squamous cell carcinoma | Image:Squamous cell carcinoma of the prostate 2.jpg|Prostate: Squamous cell carcinoma | ||
</gallery> | </gallery> | ||
</div> | </div> | ||
| Line 109: | Line 108: | ||
<div align="left"> | <div align="left"> | ||
<gallery heights="175" widths="175"> | <gallery heights="175" widths="175"> | ||
Image:Head oral scc.jpg|Squamous | Image:Head oral scc.jpg|Squamous cell cancer of the mouth: Irregular, necrotic appearing tissue on the inside of the mouth due to extensive squamous cell cancer, resulting in a limited ability to open the mouth (aka trismus). | ||
Image:head_oral_scc1.jpg|Squamous | Image:head_oral_scc1.jpg|Squamous cell cancer, base of tongue: Note white area with swelling, right base of tongue. | ||
Image:Squamous cell carcinoma oral 002.jpg|Squamous cell carcinoma in oral cavity. <br> <small> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> | Image:Squamous cell carcinoma oral 002.jpg|Squamous cell carcinoma in oral cavity. <br> <small> [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> | ||
| Line 118: | Line 117: | ||
=== Cervix: Squamous cell carcinoma=== | === Cervix: Squamous cell carcinoma=== | ||
{{#ev:youtube|zB47nE-i8dQ}} | |||
{{#ev:youtube|J3kULzKGzws}} | |||
==References== | ==References== | ||
{{reflist|2}} | {{reflist|2}} | ||
[[Category:Dermatology]] | [[Category:Dermatology]] | ||
[[Category:Types of cancer]] | [[Category:Types of cancer]] | ||
[[Category:Otolaryngology]] | [[Category:Otolaryngology]] | ||
[[Category:Mature chapter]] | [[Category:Mature chapter]] | ||
[[Category:Grammar]] | [[Category:Grammar]] | ||
Latest revision as of 19:37, 28 August 2015
|
Squamous cell carcinoma of the skin Microchapters |
|
Differentiating Squamous cell carcinoma of the skin from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Squamous cell carcinoma clinical features On the Web |
|
American Roentgen Ray Society Images of Squamous cell carcinoma clinical features |
|
Directions to Hospitals Treating Squamous cell carcinoma of the skin |
|
Risk calculators and risk factors for Squamous cell carcinoma clinical features |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Aditya Govindavarjhulla, M.B.B.S. [2], Raviteja Guddeti, M.B.B.S. [3]
Overview
The majority of squamous cell carcinomas arise on the sun-exposed areas of the skin on the head and neck, with fewer lesions arising on the extremities and the trunk. The early lesions of squamous cell carcinoma frequently present as a red, scaly spots while later lesions may form nodules or firm plaques, either of which can ulcerate ( http://tray.dermatology.uiowa.edu). Diagnosis is established by performing a biopsy and the obtaining histopathological confirmation. Complete excision is curative in the vast majority of cases, however occasionally squamous cell carcinoma will invade along the perineural layer of peripheral nerves and will extend well beyond the clinically apparent mass. Local recurrence is more common in these instances and when occurring on the head, may cause direct intracranial extension. Metastases to draining lymph nodes occurs in a minority of cases and disseminated disease is the cause of most squamous cell carcinoma-related deaths. Higher rates of metastasis (~15%) are observed with primary lesions of the lips or ears (Rowe et al., 1992). Radiation therapy is helpful in some cases of locally recurrent disease in which complete resection is difficult to achieve.
History / Presenting complaints
Squamous cell carcinoma is often easy to visualize on the body, as it most often occurs in fairly exposed areas of the body such as the face, ears, neck and arms. It is a slow growing tumor, and its presentation usually depends on the part of the body that is involved. It may vary in appearance from a simple growing lump, a plaque or a bleeding ulcer.[1]
Systemic symptoms of this carcinoma are seen in the advanced stages where the cancer disseminates. Usually, the only systemic symptom is easy fatiguability, however certain symptoms such as dysphagia and odynophagia are seen when the tongue, lips, or esophagus are involved.
Skin
Persons who present with squamous cell carcinoma of skin may have one of the following risk factors;
- Significant sun exposure
- Benign lesions such as chalazion
- Chronic ulcers
-
![Squamous cell skin cancer.[2]](/images/1/17/Squamous_cell_skin_cancer.jpg)
Squamous cell skin cancer.[2]
-

Squamous cell carcinoma in the oral cavity.
Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology -
![This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma [3].](/images/f/f4/AuricleMelanoma_SqCC.jpg)
This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma [3].
![Squamous cell skin cancer.[2]](/index.php/File:Squamous_cell_skin_cancer.jpg)

![This patient had two adjacent cancers. The flat black lesion below the antitragus is a malignant melanoma. The white elevated keratotic lesion is a squamous cell carcinoma [3].](/index.php/File:AuricleMelanoma_SqCC.jpg)
Presentation : Plaques and ulcers are commonly seen over the face causing disfiguration, and can be exophytic over the lips.
Tongue and Esophagus
Persons who present with squamous cell carcinoma of tongue and esophagus are likely to have following risk factors;
- Tobacco chewing or smoking
- Alcohol abuse
- Poor dental hygiene
-

Squamous cell carcinoma in oral cavity.
Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology -
![A large squamous cell carcinoma of the tongue[4]](/images/e/e9/Squamous_cell_carcinoma.jpg)
A large squamous cell carcinoma of the tongue[4]

![A large squamous cell carcinoma of the tongue[4]](/index.php/File:Squamous_cell_carcinoma.jpg)
Presentation : It usually presents as an ulceration on the lateral aspect of the tongue, which is pink to red in color. The patient will often find it tough to eat or swallow as a result of the lesion. Involvement of the throat and esophagus leads to symptoms of dysphagia and odynophagia, first to solids, and then in later stages to liquids also. Swelling of lymph nodes presenting as lumps in the neck will often occur in later stages of cancer.
Nasopharynx
Persons who have SCC of this region seldom have any known risk factors. It is usually caused by infection with Epstein-Barr virus.
Presentation : This patient presented with symptoms from the mass effect of the tumor. Symptoms included nasal discharge, bleeding from the nose, and nasal obstruction. Other complaints included ear infection, deafness, tinnitus, headache, and neck swelling.[5]
Lungs
Persons who have SCC of lungs usually have the following risk factors in their history;
- Therapeutic radiation (PUVA for psoriais)
- Tobacco smoking
-
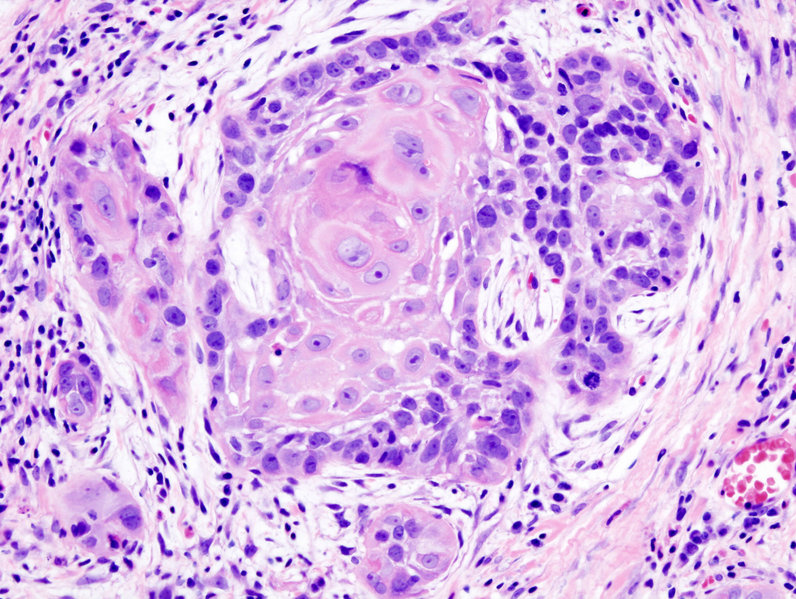
Biopsy of a highly differentiated squamous cell carcinoma of the mouth.Haematoxylin & eosin stain.
-

Photograph of a squamous cell carcinoma. Tumor is on the left, obstructing the bronchus with inflammation and mucus accumulation in the bronchus.
_squamous_cell_carcinoma_histopathology.jpg)

Presentation : Persons who present with squamous cell carcinoma of the lungs typically do not present with pulmonary symptoms. However if the cancer is exophytic and occupies the bronchi, persistent cough, hemoptysis, and recurrent infections may be seen.
Penis
Persons who present with Squamous cell carcinoma of penis are most likely to have a history of;
- Pre-malignant lesions (Bowen's disease, Condyloma , Warts)
- Smoking and tobacco chewing
Presentation : Unhealed lesions and subtle indurations may be the intial presentation. Warts can often be a predisposing factor, and large warts can lead to infection and necrosis, occasionally causing hemorrhage.
others
-

Squamous Cell Cancer of the Mouth: Cancer that originated along the lower gum line, leading to spread along the left submandibular lymph nodes.
-

Squamous Cell Cancer of the Mouth: Cancer that originated along the lower gum line, leading to spread along the left submandibular lymph nodes.


![Recurrent squamous cell carcinoma of the auricle (far left) excised with a stellate incision across the antihelix[6].](/index.php/File:Auriclesqccastellateexcision.jpg)
![Final result of the excision[7].](/index.php/File:Auricle003.jpg)
-
Prostate: Squamous cell carcinoma
-
Prostate: Squamous cell carcinoma
-
Squamous cell cancer of the mouth: Irregular, necrotic appearing tissue on the inside of the mouth due to extensive squamous cell cancer, resulting in a limited ability to open the mouth (aka trismus).
-

Squamous cell cancer, base of tongue: Note white area with swelling, right base of tongue.
-

Squamous cell carcinoma in oral cavity.
Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology



{kind=link}
{kind=link}
Cervix: Squamous cell carcinoma
{{#ev:youtube|zB47nE-i8dQ}}
{{#ev:youtube|J3kULzKGzws}}
References
- ↑ www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001832/
- ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ http://www.ghorayeb.com
- ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ Sham JS, Poon YF, Wei WI, Choy D. Nasopharyngeal carcinoma in young patients. Cancer. Jun 1 1990;65(11):2606-10.
- ↑ http://www.ghorayeb.com
- ↑ http://www.ghorayeb.com