Scabies
Template:DiseaseDisorder infobox Template:Search infobox Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Scabies is a transmissible ectoparasite skin infection characterized by superficial burrows, intense pruritus (itching) and secondary infection. The word scabies comes from the Latin word for "scratch" (scabere).
Etiology
Scabies is caused by the mite Sarcoptes scabiei, variety hominis, as shown by the Italian biologist Diacinto Cestoni in the 18th century. It produces intense, itchy skin rashes when the impregnated female tunnels into the stratum corneum of the skin and deposits eggs in the burrow. The larvae, which hatch in 3-10 days, move about on the skin, molt into a "nymphal" stage, and then mature into adult mites. The adult mites live 3-4 weeks in the host's skin.
The action of the mites moving within the skin and on the skin itself produces an intense itch which may resemble an allergic reaction in appearance. The presence of the eggs produces a massive allergic response which, in turn, produces more itching.
Scabies is transmitted readily, often throughout an entire household, by skin-to-skin contact with an infected person (e.g. bed partners, schoolmates, daycare), and thus is sometimes, although inaccurately, classed as a sexually transmitted disease. Spread by clothing, bedding, or towels is a less significant risk, though possible.
Onset
It takes approximately 4-6 weeks to develop symptoms after initial infestation. Therefore, a person may have been contagious for at least a month before being diagnosed. This means that person might have passed scabies to anyone at that time with whom they had close contact. Someone who sleeps in the same room with a person with scabies has a high possibility of having scabies as well, although they may not show symptoms.
The symptoms are caused by an allergic reaction that the body develops over time to the mites and their by-products under the skin, thus the 4-6 week "incubation" period. There are usually relatively few mites on a normal, healthy person — about 11 females in burrows. Scabies are microscopic although sometimes they are visible as a pinpoint of white. The females burrow into the skin and lay eggs there. Males roam on top of the skin, however, they can and do occasionally burrow. Both males and females surface at times, especially at night. They can be washed or scratched off (however scratching should be done with a washcloth to avoid cutting the skin as this can lead to infection), which, although not a cure, helps to keep the total population low. Also, humans create antibodies to the scabies mites which do kill some of them.
Signs, symptoms, and diagnosis

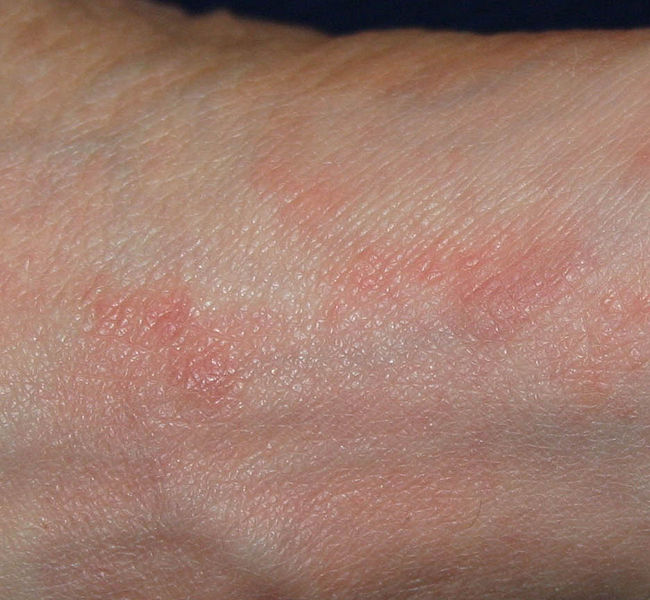
A delayed hypersensitivity (allergic) response resulting in a papular eruption (red, elevated area on skin) often occurs 30-40 days after infestation. While there may be hundreds of papules, fewer than 10 burrows are typically found. The burrow appears as a fine, wavy and slightly scaly line a few millimeters to one centimeter long. A tiny mite (0.3 to 0.9.08 mm) may sometimes be seen at the end of the burrow. Most burrows occur in the webs of fingers, flexing surfaces of the wrists, around elbows and armpits, the areolae of the breasts in females and on genitals of males, along the belt line, and on the lower buttocks. The face usually does not become involved in adults.
The rash may become secondarily infected; scratching the rash may break the skin and make secondary infection more likely. In persons with severely reduced immunity, such as those with HIV infection, or people being treated with immunosuppressive drugs like steroids, a widespread rash with thick scaling may result. This variety of scabies is called Norwegian scabies.
Scabies is frequently misdiagnosed as intense pruritus (itching of healthy skin) before papular eruptions form. Upon initial pruritus the burrows appear as small, barely noticeable bumps on the hands and may be slightly shiny and dark in color rather than red. Initially the itching may not exactly correlate to the location of these bumps. As the infestation progresses, these bumps become more red in color.
Generally diagnosis is made by finding burrows, which often may be difficult because they are scarce, because they are obscured by scratch marks, or by secondary dermatitis (unrelated skin irritation). If burrows are not found in the primary areas known to be affected, the entire skin surface of the body should be examined.
The suspicious area can be rubbed with ink from a fountain pen or alternately a topical tetracycline solution which will glow under a special light. The surface is then wiped off with an alcohol pad; if the person is infected with scabies, the characteristic zigzag or S pattern of the burrow across the skin will appear.
When a suspected burrow is found, diagnosis may be confirmed by microscopy of surface scrapings, which are placed on a slide in glycerol, mineral oil or immersion in oil and covered with a coverslip. Avoiding potassium hydroxide is necessary because it may dissolve fecal pellets. Positive diagnosis is made when the mite, ova, or fecal pellets are found.
Physical Examination
Skin
-
Scabies on the Foot
-

Scabies on the Arm
-

Scabies on the Hand
-

Scabies of the Finger
-
![Scabies (common location in ventral wrist) [1]](/images/7/75/Scabies_%28common_location_is_ventral_wrist%29.jpg)
Scabies (common location in ventral wrist) [1]




![Scabies (common location in ventral wrist) [1]](/index.php/File:Scabies_(common_location_is_ventral_wrist).jpg)
Scabies in animals
The most frequently diagnosed form is Sarcoptic mange in dogs. In dogs and other animals, scabies produces severe itching and secondary skin infections. Affected animals often lose weight and become unthrifty.

Many domestic animals have their own species of Sarcoptes mites, and all can transiently affect humans.[2][3]
Compromised immune systems
People with compromised immune systems may not develop antibodies to the mites and may develop crusted Norwegian scabies. In this case, many form scabs or develop very red skin especially in the elderly and the mentally handicapped where white or gray crusted areas develop with little itching and little or no red bumps and mite population numbers soar to hundreds, thousands, or millions in AIDS patients. These cases require additional treatment options to ensure a complete kill. Ivermectin is the treatment of choice in these patients combined with any other topical treatment.

Evolution of infection
-

Day 4
-

Day 8 (treatment begins)
-

Day 12 (under treatment)
-
Healed




Treatment
Medications
Expect increased itching and red bumps for the first week after taking any medication for scabies. The dead mites remain in the skin for 30 days. They are removed with the body's natural shedding process. During those 30 days expect new bumps and itching.
The following agents have been used in the treatment of scabies:
Oral
- Ivermectin (Stromectol): Broad spectrum anti-parasite medication. Newest scabies treatment. Safer than other alternatives and is the easiest and quickest to use. [3]
A single dose of ivermectin (dosing: 200 µg/kg) has been reported to cure, but is an off-label use; some authorities recommend repeating treatment at 14 days.
Topical
- Crotamiton (except to eyes, nose, mouth), 25% benzyl benzoate cream or lotion.
- Malathion: Common pesticide, nervous system toxin in high quantities, no known mutagenic or carcinogenic properties in humans have been confirmed.[4]
- Permethrin: Another pesticide, lacks carcinogenic and teratogenic testing in humans although animal tests showed no signs of carcinogenic or teratogenic effects. Toxicity may resemble allergic reactions. [5]
- Crotamiton (Eurax): Less toxic, but less effective. Must use for roughly 3 days. [6]
- Benzyl benzoate: Less toxic, but can cause asthmatic and allergic reactions. Must use for a week on 1st, 4th, and 7th day.
- 10% sulfur ointment: Can be used in pregnant women and infants under two months of age. It is available over-the-counter.
- Lindane: (Kwell, Kwellada). For use with patients where permethrin use is contraindicated.[7]
Lindane has been used in the past to treat both scabies and lice. While infrequent, serious side effects have occurred when using lindane and is therefore considered a treatment option of last resort [8]. Lindane is no longer available in the UK or Australia, but is still available in the U.S.. Lindane is readily absorbed through the skin if the shower to wash it off is too hot. Similarly, 5–10% sulfur ointments are considered historical.[4]
Preventing Reinfection
All family and close contacts should be treated at the same time, even if asymptomatic. After treatment has been applied or taken, (or directly before treatment if you are careful and wear gloves) cleaning of environment should occur. A person can easily be reinfected with scabies.
Without a host, scabies mites can on average survive up to 48-72 hours away from human skin. [9] As in cases of Crusted Scabies, they can survive much longer, up to 7 days. Therefore it is recommended, after treatment, to wash all material (such as clothes, bedding, and towels) that has been in contact with all infested persons in the last three days.
All household members should be treated at the same time and cleaning must be thorough and simultaneous. Either isolate long enough for the mites to die in a plastic bag for at least 1 week, or clean or freeze overnight.
- Vacuuming floors, carpets, and rugs.
- Disinfecting floor and bathroom surfaces by mopping (this only needs to be done after the first treatment).
- Daily washing of recently worn clothes, towels and bedding in hot water and drying in a hot dryer.
- Hot drying pillows for 30 minutes.
- Overnight freezing, in a plastic bag: stuffed animals, brushes, combs, shoes, coats, gloves, hats, robes, wetsuits, etc.
- Quarantine in a plastic bag for two weeks: things that cannot be washed, hot dried, frozen or drycleaned.
- Drycleaning: things that cannot be washed, hot dried or frozen or quarantined.
Treatment for Pets
Pets and humans get infected with different types of mites. The mites that we get can not survive and reproduce on pets.
Itchiness During Treatment
Options to combat itchiness include antihistamines such as cetirizine. Prescription: Doxepin (Sinequan - oral or Zonalon - topical).
Resources
- Center for Disease Control
- The Merck Manual of Diagnosis and Therapy, 17th edition, 1999
- Clinician's Pocket Reference, 9th edition, 2002
- Taber's Cyclopedic Medical Dictionary, 17th edition, 1993
- United States Centers for Disease Control and Protection
- World Health Organization Essential Medicines Library
- American Social Health Association
- Chosidow O. "Scabies". New Engl J Med. 354 (16): 1718&ndash, 1727.
- MedlinePlus Drug Information: Lindane
References
- ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ Chakrabarti A (1985). "Some epidemiological aspects of animal scabies in human population". Int J Zoonoses. 12 (1): 39&ndash, 52. PMID 4055268.
- ↑ Ulmer A, Schanz S, Röcken M, Fierlbeck G (2007). "A papulovesicular rash in a farmer and his wife". Clin Infect Dis. 45 (3): 395&ndash, 96.
- ↑ Topical (surface) medications are often effective and should be applied thoroughly to all skin from the neck down, especially to areas known to be primarily affected (skin folds, hands, etc.). The topical medication of choice is 5% permethrin because it is safe for all age groups.Scheinfeld NS (2004). "Controlling scabies in institutional settings: a review of medications, treatment models, and implementation". Amer J Clin Dermatol. 5 (1): 31–7.
External links
http://stdhelp.org/about/scabies.php Scabies Pictures & Symptoms
Template:Pediculosis, acariasis and other infestations Template:SIB
af:Scabies ar:جرب ca:Sarna da:Fnat de:Scabies et:Sarkoptoos id:Kudis it:Scabbia he:גרדת lb:Krätz hu:Rühösség nl:Schurft (mens) no:Skabb fi:Syyhy sv:Skabb