Quetiapine: Difference between revisions
No edit summary |
No edit summary |
||
| Line 8: | Line 8: | ||
|genericName= | |genericName= | ||
Quetiapine | |||
|aOrAn= | |aOrAn= | ||
| Line 20: | Line 20: | ||
|indication= | |indication= | ||
schizophrenia, bipolar I disorder, manic or mixed episodes, bipolar disorder, depressive episodes, major depressive disorder, adjunctive therapy with antidepressants | |||
|hasBlackBoxWarning= | |hasBlackBoxWarning= | ||
| Line 28: | Line 28: | ||
|adverseReactions= | |adverseReactions= | ||
somnolence, dry mouth, constipation, dizziness, increased appetite, dyspepsia, weight gain, fatigue, dysarthria, and nasal congestion in the adults. | |||
somnolence, dizziness, fatigue, increased appetite, nausea, vomiting, dry mouth, tachycardia, weight increase in children and adolescents | |||
<!--Black Box Warning--> | <!--Black Box Warning--> | ||
|blackBoxWarningTitle= | |blackBoxWarningTitle= | ||
Title | Title INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS; and SUICIDAL THOUGHTS AND BEHAVIORS | ||
|blackBoxWarningBody= | |blackBoxWarningBody= | ||
<i><span style="color:#FF0000;">ConditionName: </span></i> | <i><span style="color:#FF0000;">ConditionName: </span></i> | ||
* | *Increased Mortality in Elderly Patients with Dementia-Related Psychosis | ||
:*Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. SEROQUEL XR is not approved for elderly patients with dementia-related psychosis | |||
*Suicidal Thoughts and Behaviors | |||
:*Increased risk of suicidal thoughts and behavior in children, adolescents and young adults taking antidepressants | |||
:*Monitor for worsening and emergence of suicidal thoughts and behaviors | |||
<!--Adult Indications and Dosage--> | <!--Adult Indications and Dosage--> | ||
| Line 46: | Line 52: | ||
|fdaLIADAdult= | |fdaLIADAdult= | ||
*Important Administration Instructions | |||
:*SEROQUEL XR tablets should be swallowed whole and not split, chewed or crushed. | |||
:*It is recommended that SEROQUEL XR be taken without food or with a light meal (approximately 300 calories). | |||
:*SEROQUEL XR should be administered once daily, preferably in the evening. | |||
* Dosing | *Recommended Dosing | ||
:*The recommended initial dose, titration, dose range and maximum SEROQUEL XR dose for each approved indication is displayed in Table 1 below. After initial dosing, adjustments can be made upwards or downwards, if necessary, depending upon the clinical response and tolerability of the patient | |||
: | : [[File:{{PAGENAME}}01.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | ||
* | *Maintenance Treatment for Schizophrenia and Bipolar I Disorder | ||
:*Maintenance Treatment | |||
:**Patients should be periodically reassessed to determine the need for maintenance treatment and the appropriate dose for such treatment. | |||
:* | *Dose Modifications in Elderly Patients | ||
:*Consideration should be given to a slower rate of dose titration and a lower target dose in the elderly and in patients who are debilitated or who have a predisposition to hypotensive reactions [see Use in Specific Populations (8.5, 8.7) and Clinical Pharmacology (12)]. When indicated, dose escalation should be performed with caution in these patients. | |||
:*Elderly patients should be started on SEROQUEL XR 50 mg/day and the dose can be increased in increments of 50 mg/day depending on the clinical response and tolerability of the individual patient. | |||
*Dose Modifications in Hepatically Impaired Patients | |||
:*Patients with hepatic impairment should be started on SEROQUEL XR 50 mg/day. The dose can be increased daily in increments of 50 mg/day to an effective dose, depending on the clinical response and tolerability of the patient. | |||
* | *Dose Modifications when used with CYP3A4 Inhibitors | ||
:*SEROQUEL XR dose should be reduced to one sixth of original dose when co-medicated with a potent CYP3A4 inhibitor (e.g., ketoconazole, itraconazole, indinavir, ritonavir, nefazodone, etc.). When the CYP3A4 inhibitor is discontinued, the dose of SEROQUEL XR should be increased by 6 fold. | |||
:* | *Dose Modifications when used with CYP3A4 Inducers | ||
:*SEROQUEL XR dose should be increased up to 5 fold of the original dose when used in combination with a chronic treatment (e.g., greater than 7-14 days) of a potent CYP3A4 inducer (e.g., phenytoin, carbamazepine, rifampin, avasimibe, St. John’s wort etc.). The dose should be titrated based on the clinical response and tolerance of the individual patient. When the CYP3A4 inducer is discontinued, the dose of SEROQUEL XR should be reduced to the original level within 7-14 days [see Clinical Pharmacology (12.3) and Drug Interactions (7.1)]. | |||
*Reinitiation of Treatment in Patients Previously Discontinued | |||
:*Although there are no data to specifically address re-initiation of treatment, it is recommended that when restarting therapy of patients who have been off SEROQUEL XR for more than one week, the initial dosing schedule should be followed. When restarting patients who have been off SEROQUEL XR for less than one week, gradual dose escalation may not be required and the maintenance dose may be reinitiated. | |||
* | *Switching Patients from SEROQUEL Tablets to SEROQUEL XR Tablets | ||
:*Patients who are currently being treated with SEROQUEL (immediate release formulation) may be switched to SEROQUEL XR at the equivalent total daily dose taken once daily. Individual dosage adjustments may be necessary. | |||
:* | *Switching from Antipsychotics | ||
:*There are no systematically collected data to specifically address switching patients from other antipsychotics to SEROQUEL XR, or concerning concomitant administration with other antipsychotics. While immediate discontinuation of the previous antipsychotic treatment may be acceptable for some patients, more gradual discontinuation may be most appropriate for others. In all cases, the period of overlapping antipsychotic administration should be minimized. When switching patients from depot antipsychotics, if medically appropriate, initiate SEROQUEL XR therapy in place of the next scheduled injection. The need for continuing existing extrapyramidal syndrome medication should be re-evaluated periodically. | |||
<!--Off-Label Use and Dosage (Adult)--> | <!--Off-Label Use and Dosage (Adult)--> | ||
| Line 162: | Line 181: | ||
|contraindications= | |contraindications= | ||
* | *Hypersensitivity to quetiapine or to any excipients in the SEROQUEL XR formulation. Anaphylactic reactions have been reported in patients treated with SEROQUEL XR. | ||
<!--Warnings--> | <!--Warnings--> | ||
| Line 168: | Line 187: | ||
|warnings= | |warnings= | ||
* | ====Precautions==== | ||
=====Increased Mortality in Elderly Patients with Dementia-Related Psychosis===== | |||
*Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. Analysis of 17 placebo-controlled trials (modal duration of 10 weeks), largely in patients taking atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of between 1.6 to 1.7 times the risk of death in placebo-treated patients. Over the course of a typical 10-week controlled trial, the rate of death in drug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. SEROQUEL XR is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning]. | |||
=====Suicidal Thoughts and Behaviors in Adolescents and Young Adults===== | |||
*Patients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment. Pooled analyses of short-term placebo-controlled trials of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18-24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older. | |||
*The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk differences (drug vs. placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 2. | |||
: [[File:{{PAGENAME}}02.png|thumb|none|600px|This image is provided by the National Library of Medicine.]] | |||
*No suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was not sufficient to reach any conclusion about drug effect on suicide. | |||
*It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression. | |||
*All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases. | |||
*The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality. | |||
*Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset, or were not part of the patient's presenting symptoms. | |||
*Families and caregivers of patients being treated with antidepressants for major depressive disorder or other indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to healthcare providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for SEROQUEL XR should be written for the smallest quantity of tablets consistent with good patient management, in order to reduce the risk of overdose. | |||
=====Screening Patients for Bipolar Disorder===== | |||
A major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled trials) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, including SEROQUEL XR, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression. | |||
5.3 Cerebrovascular Adverse Reactions, Including Stroke, in Elderly Patients with Dementia-Related Psychosis | |||
In placebo-controlled trials with risperidone, aripiprazole, and olanzapine in elderly subjects with dementia, there was a higher incidence of cerebrovascular adverse reactions (cerebrovascular accidents and transient ischemic attacks), including fatalities, compared to placebo-treated subjects. SEROQUEL XR is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning and Warnings and Precautions (5.1)]. | |||
5.4 Neuroleptic Malignant Syndrome (NMS) | |||
A potentially fatal symptom complex sometimes referred to as Neuroleptic Malignant Syndrome (NMS) has been reported in association with administration of antipsychotic drugs, including quetiapine. Rare cases of NMS have been reported with quetiapine. Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status, and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia). Additional signs may include elevated creatine phosphokinase, myoglobinuria (rhabdomyolysis) and acute renal failure. | |||
The diagnostic evaluation of patients with this syndrome is complicated. In arriving at a diagnosis, it is important to exclude cases where the clinical presentation includes both serious medical illness (e.g., pneumonia, systemic infection, etc.) and untreated or inadequately treated extrapyramidal signs and symptoms (EPS). Other important considerations in the differential diagnosis include central anticholinergic toxicity, heat stroke, drug fever and primary central nervous system (CNS) pathology. | |||
The management of NMS should include: 1) immediate discontinuation of antipsychotic drugs and other drugs not essential to concurrent therapy; 2) intensive symptomatic treatment and medical monitoring; and 3) treatment of any concomitant serious medical problems for which specific treatments are available. There is no general agreement about specific pharmacological treatment regimens for NMS. | |||
If a patient requires antipsychotic drug treatment after recovery from NMS, the potential reintroduction of drug therapy should be carefully considered. The patient should be carefully monitored since recurrences of NMS have been reported. | |||
5.5 Metabolic Changes | |||
Atypical antipsychotic drugs have been associated with metabolic changes that include hyperglycemia/diabetes mellitus, dyslipidemia, and body weight gain. While all of the drugs in the class have been shown to produce some metabolic changes, each drug has its own specific risk profile. In some patients, a worsening of more than one of the metabolic parameters of weight, blood glucose, and lipids was observed in clinical studies. Changes in these metabolic profiles should be managed as clinically appropriate. | |||
Hyperglycemia and Diabetes Mellitus | |||
Hyperglycemia, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients treated with atypical antipsychotics, including quetiapine. Assessment of the relationship between atypical antipsychotic use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given these confounders, the relationship between atypical antipsychotic use and hyperglycemia-related adverse reactions is not completely understood. However, epidemiological studies suggest an increased risk of treatment-emergent hyperglycemia-related adverse reactions in patients treated with the atypical antipsychotics. Precise risk estimates for hyperglycemia-related adverse reactions in patients treated with atypical antipsychotics are not available. | |||
Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g., obesity, family history of diabetes) who are starting treatment with atypical antipsychotics should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patient treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia, and weakness. Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics should undergo fasting blood glucose testing. In some cases, hyperglycemia has resolved when the atypical antipsychotic was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of the suspect drug. | |||
Adults: | |||
<!--Adverse Reactions--> | <!--Adverse Reactions--> | ||
Revision as of 21:53, 4 August 2014
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Black Box Warning
|
Title INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS; and SUICIDAL THOUGHTS AND BEHAVIORS
See full prescribing information for complete Boxed Warning.
ConditionName:
|
Overview
Quetiapine is a that is FDA approved for the {{{indicationType}}} of schizophrenia, bipolar I disorder, manic or mixed episodes, bipolar disorder, depressive episodes, major depressive disorder, adjunctive therapy with antidepressants. There is a Black Box Warning for this drug as shown here. Common adverse reactions include somnolence, dry mouth, constipation, dizziness, increased appetite, dyspepsia, weight gain, fatigue, dysarthria, and nasal congestion in the adults. somnolence, dizziness, fatigue, increased appetite, nausea, vomiting, dry mouth, tachycardia, weight increase in children and adolescents.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
- Important Administration Instructions
- SEROQUEL XR tablets should be swallowed whole and not split, chewed or crushed.
- It is recommended that SEROQUEL XR be taken without food or with a light meal (approximately 300 calories).
- SEROQUEL XR should be administered once daily, preferably in the evening.
- Recommended Dosing
- The recommended initial dose, titration, dose range and maximum SEROQUEL XR dose for each approved indication is displayed in Table 1 below. After initial dosing, adjustments can be made upwards or downwards, if necessary, depending upon the clinical response and tolerability of the patient
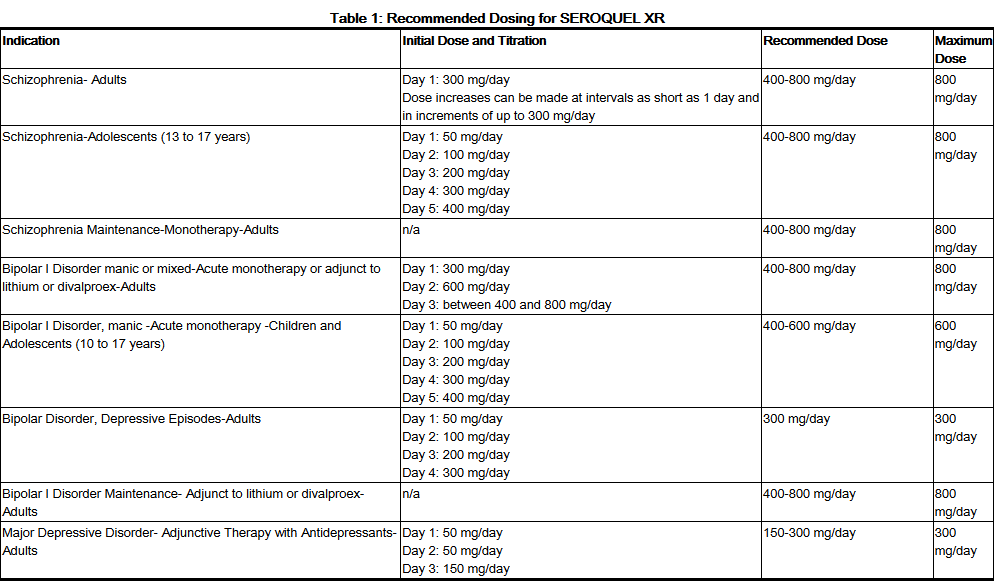
This image is provided by the National Library of Medicine.

- Maintenance Treatment for Schizophrenia and Bipolar I Disorder
- Maintenance Treatment
- Patients should be periodically reassessed to determine the need for maintenance treatment and the appropriate dose for such treatment.
- Maintenance Treatment
- Dose Modifications in Elderly Patients
- Consideration should be given to a slower rate of dose titration and a lower target dose in the elderly and in patients who are debilitated or who have a predisposition to hypotensive reactions [see Use in Specific Populations (8.5, 8.7) and Clinical Pharmacology (12)]. When indicated, dose escalation should be performed with caution in these patients.
- Elderly patients should be started on SEROQUEL XR 50 mg/day and the dose can be increased in increments of 50 mg/day depending on the clinical response and tolerability of the individual patient.
- Dose Modifications in Hepatically Impaired Patients
- Patients with hepatic impairment should be started on SEROQUEL XR 50 mg/day. The dose can be increased daily in increments of 50 mg/day to an effective dose, depending on the clinical response and tolerability of the patient.
- Dose Modifications when used with CYP3A4 Inhibitors
- SEROQUEL XR dose should be reduced to one sixth of original dose when co-medicated with a potent CYP3A4 inhibitor (e.g., ketoconazole, itraconazole, indinavir, ritonavir, nefazodone, etc.). When the CYP3A4 inhibitor is discontinued, the dose of SEROQUEL XR should be increased by 6 fold.
- Dose Modifications when used with CYP3A4 Inducers
- SEROQUEL XR dose should be increased up to 5 fold of the original dose when used in combination with a chronic treatment (e.g., greater than 7-14 days) of a potent CYP3A4 inducer (e.g., phenytoin, carbamazepine, rifampin, avasimibe, St. John’s wort etc.). The dose should be titrated based on the clinical response and tolerance of the individual patient. When the CYP3A4 inducer is discontinued, the dose of SEROQUEL XR should be reduced to the original level within 7-14 days [see Clinical Pharmacology (12.3) and Drug Interactions (7.1)].
- Reinitiation of Treatment in Patients Previously Discontinued
- Although there are no data to specifically address re-initiation of treatment, it is recommended that when restarting therapy of patients who have been off SEROQUEL XR for more than one week, the initial dosing schedule should be followed. When restarting patients who have been off SEROQUEL XR for less than one week, gradual dose escalation may not be required and the maintenance dose may be reinitiated.
- Switching Patients from SEROQUEL Tablets to SEROQUEL XR Tablets
- Patients who are currently being treated with SEROQUEL (immediate release formulation) may be switched to SEROQUEL XR at the equivalent total daily dose taken once daily. Individual dosage adjustments may be necessary.
- Switching from Antipsychotics
- There are no systematically collected data to specifically address switching patients from other antipsychotics to SEROQUEL XR, or concerning concomitant administration with other antipsychotics. While immediate discontinuation of the previous antipsychotic treatment may be acceptable for some patients, more gradual discontinuation may be most appropriate for others. In all cases, the period of overlapping antipsychotic administration should be minimized. When switching patients from depot antipsychotics, if medically appropriate, initiate SEROQUEL XR therapy in place of the next scheduled injection. The need for continuing existing extrapyramidal syndrome medication should be re-evaluated periodically.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
Condition1
- Developed by:
- Class of Recommendation:
- Strength of Evidence:
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Quetiapine in adult patients.
Non–Guideline-Supported Use
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Quetiapine in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding FDA-Labeled Use of Quetiapine in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
Condition1
- Developed by:
- Class of Recommendation:
- Strength of Evidence:
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Quetiapine in pediatric patients.
Non–Guideline-Supported Use
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Quetiapine in pediatric patients.
Contraindications
- Hypersensitivity to quetiapine or to any excipients in the SEROQUEL XR formulation. Anaphylactic reactions have been reported in patients treated with SEROQUEL XR.
Warnings
|
Title INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS; and SUICIDAL THOUGHTS AND BEHAVIORS
See full prescribing information for complete Boxed Warning.
ConditionName:
|
Precautions
Increased Mortality in Elderly Patients with Dementia-Related Psychosis
- Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. Analysis of 17 placebo-controlled trials (modal duration of 10 weeks), largely in patients taking atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of between 1.6 to 1.7 times the risk of death in placebo-treated patients. Over the course of a typical 10-week controlled trial, the rate of death in drug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. SEROQUEL XR is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning].
Suicidal Thoughts and Behaviors in Adolescents and Young Adults
- Patients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment. Pooled analyses of short-term placebo-controlled trials of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18-24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older.
- The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk differences (drug vs. placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 2.
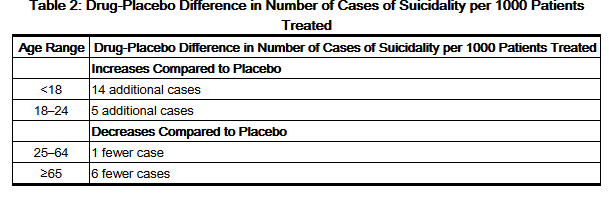
This image is provided by the National Library of Medicine.

- No suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was not sufficient to reach any conclusion about drug effect on suicide.
- It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression.
- All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases.
- The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.
- Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset, or were not part of the patient's presenting symptoms.
- Families and caregivers of patients being treated with antidepressants for major depressive disorder or other indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to healthcare providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for SEROQUEL XR should be written for the smallest quantity of tablets consistent with good patient management, in order to reduce the risk of overdose.
Screening Patients for Bipolar Disorder
A major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled trials) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, including SEROQUEL XR, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression.
5.3 Cerebrovascular Adverse Reactions, Including Stroke, in Elderly Patients with Dementia-Related Psychosis
In placebo-controlled trials with risperidone, aripiprazole, and olanzapine in elderly subjects with dementia, there was a higher incidence of cerebrovascular adverse reactions (cerebrovascular accidents and transient ischemic attacks), including fatalities, compared to placebo-treated subjects. SEROQUEL XR is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning and Warnings and Precautions (5.1)].
5.4 Neuroleptic Malignant Syndrome (NMS)
A potentially fatal symptom complex sometimes referred to as Neuroleptic Malignant Syndrome (NMS) has been reported in association with administration of antipsychotic drugs, including quetiapine. Rare cases of NMS have been reported with quetiapine. Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status, and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia). Additional signs may include elevated creatine phosphokinase, myoglobinuria (rhabdomyolysis) and acute renal failure.
The diagnostic evaluation of patients with this syndrome is complicated. In arriving at a diagnosis, it is important to exclude cases where the clinical presentation includes both serious medical illness (e.g., pneumonia, systemic infection, etc.) and untreated or inadequately treated extrapyramidal signs and symptoms (EPS). Other important considerations in the differential diagnosis include central anticholinergic toxicity, heat stroke, drug fever and primary central nervous system (CNS) pathology.
The management of NMS should include: 1) immediate discontinuation of antipsychotic drugs and other drugs not essential to concurrent therapy; 2) intensive symptomatic treatment and medical monitoring; and 3) treatment of any concomitant serious medical problems for which specific treatments are available. There is no general agreement about specific pharmacological treatment regimens for NMS.
If a patient requires antipsychotic drug treatment after recovery from NMS, the potential reintroduction of drug therapy should be carefully considered. The patient should be carefully monitored since recurrences of NMS have been reported.
5.5 Metabolic Changes
Atypical antipsychotic drugs have been associated with metabolic changes that include hyperglycemia/diabetes mellitus, dyslipidemia, and body weight gain. While all of the drugs in the class have been shown to produce some metabolic changes, each drug has its own specific risk profile. In some patients, a worsening of more than one of the metabolic parameters of weight, blood glucose, and lipids was observed in clinical studies. Changes in these metabolic profiles should be managed as clinically appropriate.
Hyperglycemia and Diabetes Mellitus
Hyperglycemia, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients treated with atypical antipsychotics, including quetiapine. Assessment of the relationship between atypical antipsychotic use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given these confounders, the relationship between atypical antipsychotic use and hyperglycemia-related adverse reactions is not completely understood. However, epidemiological studies suggest an increased risk of treatment-emergent hyperglycemia-related adverse reactions in patients treated with the atypical antipsychotics. Precise risk estimates for hyperglycemia-related adverse reactions in patients treated with atypical antipsychotics are not available.
Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g., obesity, family history of diabetes) who are starting treatment with atypical antipsychotics should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patient treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia, and weakness. Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics should undergo fasting blood glucose testing. In some cases, hyperglycemia has resolved when the atypical antipsychotic was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of the suspect drug.
Adults:
Adverse Reactions
Clinical Trials Experience
There is limited information regarding Clinical Trial Experience of Quetiapine in the drug label.
Body as a Whole
Cardiovascular
Digestive
Endocrine
Hematologic and Lymphatic
Metabolic and Nutritional
Musculoskeletal
Neurologic
Respiratory
Skin and Hypersensitivy Reactions
Special Senses
Urogenital
Miscellaneous
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Quetiapine in the drug label.
Body as a Whole
Cardiovascular
Digestive
Endocrine
Hematologic and Lymphatic
Metabolic and Nutritional
Musculoskeletal
Neurologic
Respiratory
Skin and Hypersensitivy Reactions
Special Senses
Urogenital
Miscellaneous
Drug Interactions
- Drug
- Description
Use in Specific Populations
Pregnancy
- Pregnancy Category
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Quetiapine in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Quetiapine during labor and delivery.
Nursing Mothers
There is no FDA guidance on the use of Quetiapine with respect to nursing mothers.
Pediatric Use
There is no FDA guidance on the use of Quetiapine with respect to pediatric patients.
Geriatic Use
There is no FDA guidance on the use of Quetiapine with respect to geriatric patients.
Gender
There is no FDA guidance on the use of Quetiapine with respect to specific gender populations.
Race
There is no FDA guidance on the use of Quetiapine with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Quetiapine in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Quetiapine in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Quetiapine in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Quetiapine in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
- Intravenous
Monitoring
There is limited information regarding Monitoring of Quetiapine in the drug label.
- Description
IV Compatibility
There is limited information regarding IV Compatibility of Quetiapine in the drug label.
Overdosage
Acute Overdose
Signs and Symptoms
- Description
Management
- Description
Chronic Overdose
There is limited information regarding Chronic Overdose of Quetiapine in the drug label.
Pharmacology
There is limited information regarding Quetiapine Pharmacology in the drug label.
Mechanism of Action
Structure
This image is provided by the National Library of Medicine.
Pharmacodynamics
There is limited information regarding Pharmacodynamics of Quetiapine in the drug label.
Pharmacokinetics
There is limited information regarding Pharmacokinetics of Quetiapine in the drug label.
Nonclinical Toxicology
There is limited information regarding Nonclinical Toxicology of Quetiapine in the drug label.
Clinical Studies
There is limited information regarding Clinical Studies of Quetiapine in the drug label.
How Supplied
Storage
There is limited information regarding Quetiapine Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Quetiapine |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Quetiapine |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
There is limited information regarding Patient Counseling Information of Quetiapine in the drug label.
Precautions with Alcohol
- Alcohol-Quetiapine interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- ®[1]
Look-Alike Drug Names
- A® — B®[2]
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Empty citation (help)
- ↑ "http://www.ismp.org". External link in
|title=(help)
{{#subobject:
|Page Name=Quetiapine |Pill Name=No image.jpg |Drug Name= |Pill Ingred=|+sep=; |Pill Imprint= |Pill Dosage= |Pill Color=|+sep=; |Pill Shape= |Pill Size (mm)= |Pill Scoring= |Pill Image= |Drug Author= |NDC=
}}
{{#subobject:
|Label Page=Quetiapine |Label Name=Quetiapine11.png
}}
{{#subobject:
|Label Page=Quetiapine |Label Name=Quetiapine11.png
}}