Pulmonary edema chest x ray
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
|
Pulmonary edema Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Pulmonary edema chest x ray On the Web |
|
Risk calculators and risk factors for Pulmonary edema chest x ray |
Overview
The diagnosis is confirmed on X-ray of the lungs, which shows increased fluid in the alveolar walls. Kerley B lines, increased vascular filling, pleural effusions, upper lobe diversion (increased blood flow to the higher parts of the lung) may be indicative of cardiogenic pulmonary edema, while patchy alveolar infiltrates with air bronchograms are more indicative of noncardiogenic edema
Chest X Ray
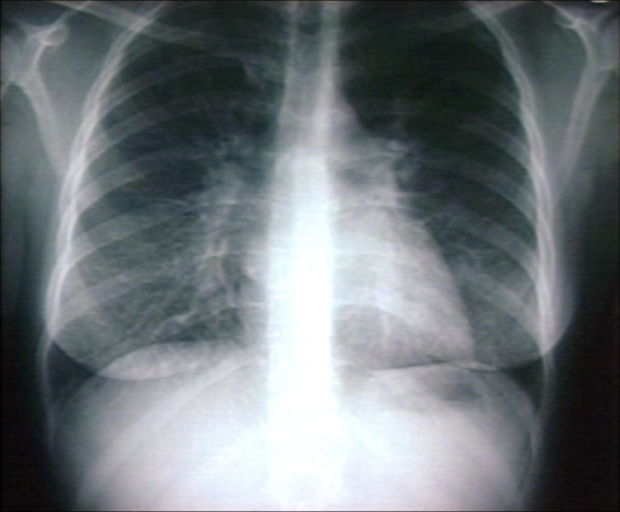
The chest x-ray is the diagnostic modality of choice in the evaluation of the patient with suspected pulmonary edema. Chest x-ray findings include:
- Kerley B lines or thickening of the interlobular septa
- Peribronchial cuffing
- Thickening of the fissures
- Cephalization
- Increased vascular markings
- Interstitial edema
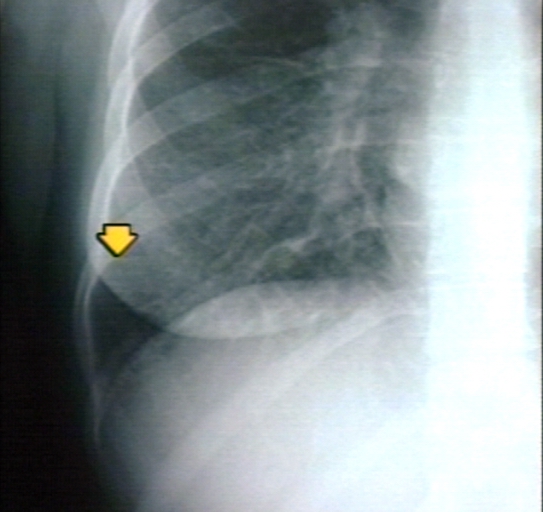
- Pleural effusions
Differentiating Cardiogenic Versus Noncardiogenic Pulmonary Edema
Cardiogenic Pulmonary Edema
Cardiogenic pulmonary edema can be distinguished from noncardiogenic pulmonary edema by the presence of redistribution of blood flow to the upper lobes (increased blood flow to the higher parts of the lung) and interstitial edema.

Noncardiogenic Pulmonary Edema
In contrast, patchy alveolar infiltrates with air bronchograms are more indicative of noncardiogenic edema.

Correlation of Chest X-Ray Findings with Pulmonary Capillary Wedge Pressure
- Normal:5-10 mm Hg
- Cephalization: 10-15 mm Hg
- Kerley B Lines: 15-20 mm Hg
- Pulmonary Interstitial Edema: 20-25 mm Hg
- Pulmonary Alveolar Edema: > 25 mm Hg
Kerley B Lines
Kerley B lines are short parallel lines at the lung periphery. These lines represent distended interlobular septa, which are usually less than 1 cm in length and parallel to one another at right angles to the pleura. They are located peripherally in contact with the pleura, but are generally absent along fissural surfaces. They may be seen in any zone but are most frequently observed at the lung bases at the costophrenic angles on the PA radiograph, and in the substernal region on lateral radiographs.
-
Plain film: Mitral stenosis, Kerley B lines
-
Plain film: Mitral stenosis, Kerley B lines
-

Plain film: Mitral stenosis, Kerley B lines



Peribronchial Cuffing
Peribronchial cuffing is an abnormality on a chest x-ray whereby the usually thin bronchial walls are thickened and take on a doughnut-like appearance.
Shown below is a chest x ray with the red arrows which demonstrate thickened bronchial walls that have a doughnut-like appearance.

Cephalization
Cephalization refers to the redistribution of blood into the upper lobe vessels. It has been hypothesized that once the hydrostatic pressure exceeds 10 mm Hg, then fluid begins to leak into the interstitium of the lung. This excess fluid initially compresses the lower lobe vessels, perhaps as a result of gravity. After this, the upper lobe vessels are recruited to distribute a greater volume of blood. In order to carry a greater volume of blood, the upper lobe vessels increase in size.
Shown below is a chest x ray with the red arrow which demonstrate cephalization of blood vessels
