Persistent truncus arteriosus pathophysiology & etiology: Difference between revisions
No edit summary |
|||
| Line 20: | Line 20: | ||
* Too much blood circulation in the lungs may cause extra fluid to build up in and around them, making it difficult to breathe. | * Too much blood circulation in the lungs may cause extra fluid to build up in and around them, making it difficult to breathe. | ||
* The blood vessels to the lungs become permanently damaged. Over time, it becomes very hard for the heart to force blood to them. This is called pulmonary hypertension and it can be life-threatening. | * The blood vessels to the lungs become permanently damaged. Over time, it becomes very hard for the heart to force blood to them. This is called pulmonary hypertension and it can be life-threatening. | ||
===Gross Pathology=== | |||
<div align="left"> | |||
<gallery heights="175" widths="175"> | |||
Image:Congenital heart defect 0035.jpg|Truncus Arteriosus with Subvalvular Ventricular Septal Defect: Gross, natural color, an excellent view of subvalvular defect. Quadricuspid truncus valve and type I origin of pulmonary arteries | |||
Image:Congenital heart defect 0036.jpg|Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross, natural color, defect is shown from the right side (view toward right ventricular outlet) | |||
Image:Congenital heart defect 0037.jpg|Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross natural color excellent view of lesion looking at opened aortic ring with quadricuspid aortic valve. A large subvalvular defect (origin of pulmonary arteries is at forceps) | |||
</gallery> | |||
</div> | |||
===Associated Conditions=== | ===Associated Conditions=== | ||
Revision as of 16:09, 3 January 2013
|
Persistent truncus arteriosus Microchapters |
|
Differentiating Persistent truncus arteriosus from other Diseases |
|---|
|
Case Studies |
|
Persistent truncus arteriosus pathophysiology & etiology On the Web |
|
American Roentgen Ray Society Images of Persistent truncus arteriosus pathophysiology & etiology |
|
FDA on Persistent truncus arteriosus pathophysiology & etiology |
|
CDC on Persistent truncus arteriosus pathophysiology & etiology |
|
Persistent truncus arteriosus pathophysiology & etiology in the news |
|
Blogs on Persistent truncus arteriosus pathophysiology & etiology |
|
Risk calculators and risk factors for Persistent truncus arteriosus pathophysiology & etiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor-in-Chief: Keri Shafer, M.D. [2]
Overview
Pathophysiology
Diagrams to illustrate the transformation of the bulbus cordis. Ao. Truncus arteriosus. Au. Atrium. B. Bulbus cordis. RV. Right ventricle. LV. Left ventricle. P. Pulmonary artery.
 In normal circulation, the pulmonary artery comes out of the right ventricle and the aorta comes out of the left ventricle, which are separate from each other. Coronary arteries (which supply blood to the heart muscle) come out of the aorta just above the valve at the entrance of the aorta.
In normal circulation, the pulmonary artery comes out of the right ventricle and the aorta comes out of the left ventricle, which are separate from each other. Coronary arteries (which supply blood to the heart muscle) come out of the aorta just above the valve at the entrance of the aorta.
In truncus arteriosus, a single artery comes out of the ventricles. There is usually also a large hole between the two ventricles (ventricular septal defect). As a result, the blue (without oxygen) and red (oxygen-rich) blood mix.
Some of this mixed blood goes to the lungs, some goes to the coronary arteries, and the rest goes to the body. Usually, too much blood is sent to the lungs.
If this condition is not treated, two problems occur:
- Too much blood circulation in the lungs may cause extra fluid to build up in and around them, making it difficult to breathe.
- The blood vessels to the lungs become permanently damaged. Over time, it becomes very hard for the heart to force blood to them. This is called pulmonary hypertension and it can be life-threatening.
Gross Pathology
-
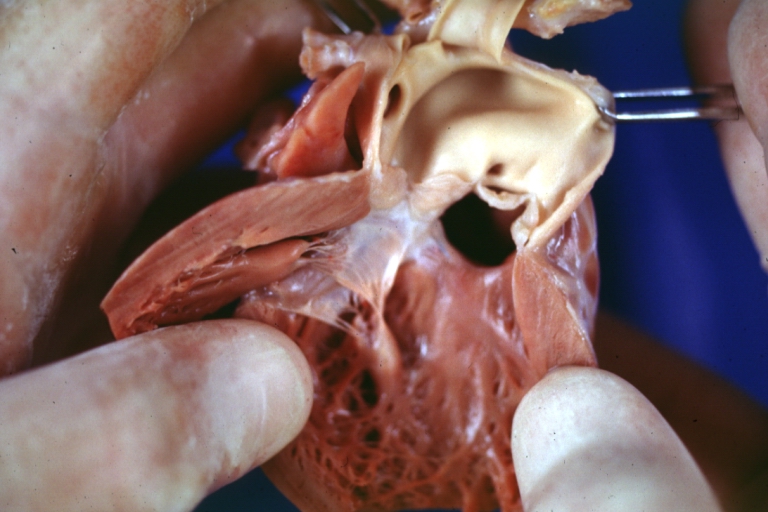
Truncus Arteriosus with Subvalvular Ventricular Septal Defect: Gross, natural color, an excellent view of subvalvular defect. Quadricuspid truncus valve and type I origin of pulmonary arteries
-

Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross, natural color, defect is shown from the right side (view toward right ventricular outlet)
-
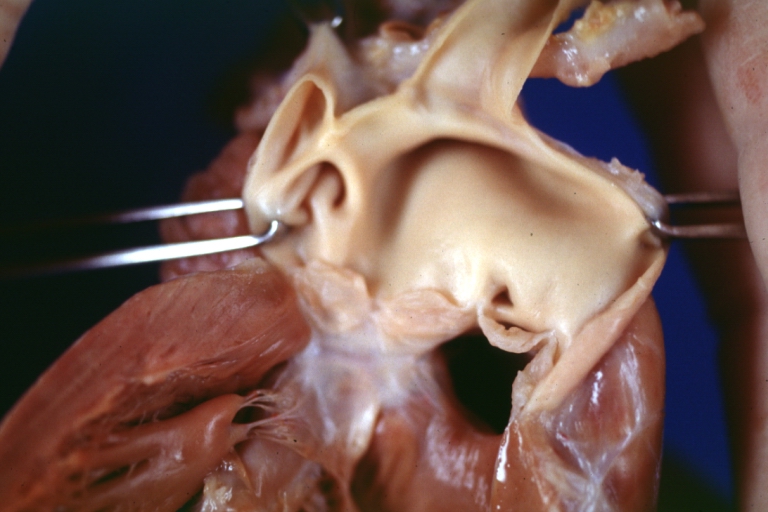
Truncus Arteriosus with Subvalvular Interventricular Septal Defect: Gross natural color excellent view of lesion looking at opened aortic ring with quadricuspid aortic valve. A large subvalvular defect (origin of pulmonary arteries is at forceps)



Associated Conditions
Anatomical changes associated with this disorder includes:
- single artery arising from the two ventricles which gives rise to both the aortic and pulmonary vessels
- abnormal truncal valve
- right sided aortic arch in about 30% of cases (not shown)
- large ventricular septal defect
- pulmonary hypertension
- complete mixing occurring at level of the great vessel
- right-to-left shunting of blood