Neonatal respiratory distress syndrome
Template:DiseaseDisorder infobox For the WikiPatient page for this topic, click here
|
Neonatal respiratory distress syndrome Microchapters |
|
Differentiating Neonatal respiratory distress syndrome from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Neonatal respiratory distress syndrome On the Web |
|
American Roentgen Ray Society Images of Neonatal respiratory distress syndrome |
|
Directions to Hospitals Treating Neonatal respiratory distress syndrome |
|
Risk calculators and risk factors for Neonatal respiratory distress syndrome |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: Respiratory distress syndrome of new born; surfactant deficient disease
Overview
Infant respiratory distress syndrome ("RDS", also called "Respiratory distress syndrome of newborn", previously called hyaline membrane disease), is a syndrome caused in premature infants by developmental insufficiency of surfactant production and structural immaturity in the lungs. It can also result from a genetic problem with the production of surfactant associated proteins. RDS affects about 1% of newborn infants and is the leading cause of death in preterm infants [1]. The incidence decreases with advancing gestational age (length of pregnancy), from about 50% in babies born at 26-28 weeks, to about 25% at 30-31 weeks. The syndrome is more frequent in infants of diabetic mothers and in the second born of premature twins.
Clinical course
Respiratory distress syndrome begins shortly after birth, and is manifest by tachypnea and chest wall retractions ("sucking in") during breathing efforts. In addition, grunting on expiration, flaring of the nostrils and cyanosis are frequent.
As the disease progresses, the baby may develop ventilatory failure (rising carbon dioxide concentrations in the blood), and prolonged cessations of breathing ("apnea"). Whether treated or not, the clinical course for the acute disease lasts about 2 to 3 days. During the first, the patient worsens and requires more support. During the second the baby may be remarkably stable on adequate support and resolution is noted during the third day, heralded by a prompt diuresis. Despite huge advances in care, RDS remains the most common single cause of death in the first month of life. Complications include metabolic disorders (acidosis, low blood sugar), patent ductus arteriosus, low blood pressure, chronic lung changes, and intracranial hemorrhage. The disease is frequently complicated by prematurity and its additional defects in other organ function.
Pathology
The characteristic pathology seen in babies who die from RDS was the source of the name "hyaline membrane disease". These waxy-appearing layers line the collapsed tiny air sacs ("alveoli") of the lung. In addition, the lungs show bleeding, over-distention of airways and damage to the lining cells.
Pathological Findings: A Case Example
Clinical Summary
A 28-hour-old newborn, after an uncomplicated vaginal delivery by a G1 24-year-old mother whose pregnancy had also been uncomplicated.
The infant was born pre-term at 36 weeks gestation and was appropriate for gestational age, weighing 2550 grams. Three hours after birth, the infant developed cyanosis and required 40% oxygen to maintain a pink color. Because of a worsening respiratory distress syndrome, the infant (1 day old) was transferred to a tertiary care hospital with a neonatal intensive care unit.
Following the transfer, the respiratory distress progressed and the admitting arterial blood gases were pH 7.31, pCO2 35, and pO2 35. The condition of the patient continued to deteriorate despite therapy, and he became "shocky" with efforts to increase blood volume. He developed a persistent bradycardia and died about 4 hours after admission.
Autopsy Findings
The organs generally showed no abnormalities other than those of immaturity expected at this gestational age. There was moderate diffuse subarachnoid hemorrhage and a small amount of blood in the pleural and pericardial cavities.
-

This is a gross photograph of lung demonstrating hyaline membrane disease (Infant respiratory distress syndrome) and atelectasis.
-
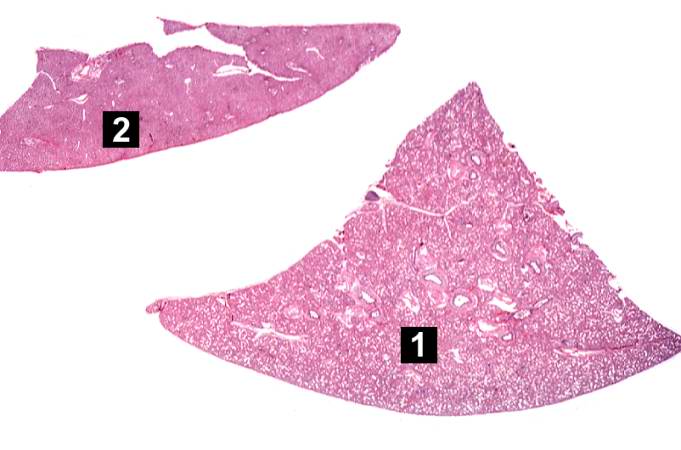
This is a low-power photomicrograph of a triangular-shaped section of lung (1) and an oblong section of liver (2). The lack of open air spaces in this neonatal lung indicates its immaturity.
-
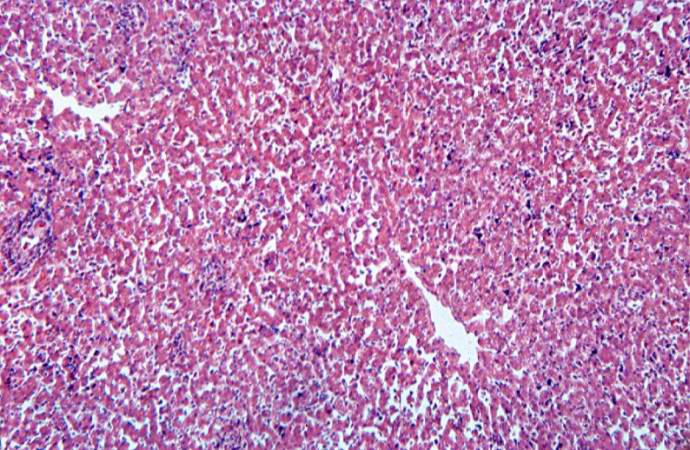
This is a low-power photomicrograph of liver which contains dark blue-stained cells in the hepatic sinusoids. These are immature blood cell precursors and this represents extramedullary hematopoiesis of the liver.



-
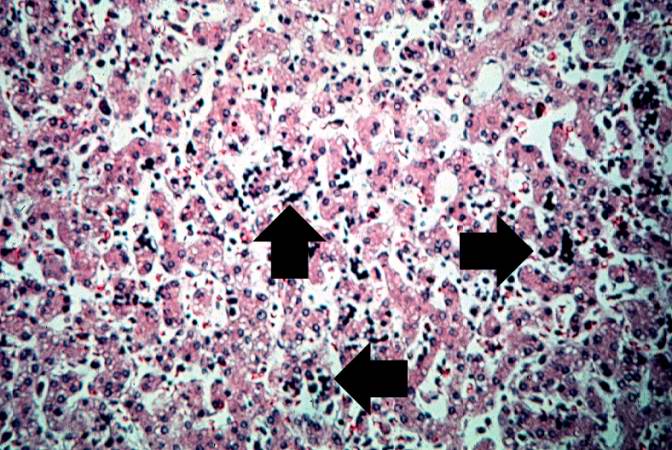
This high-power photomicrograph of liver shows more clearly the immature blood cell precursors (arrows) which represent extramedullary hematopoiesis of the liver. The liver is a normal site of fetal hematopoiesis and, for this stage of gestation, extramedullary hematopoiesis of the liver is normal.
-
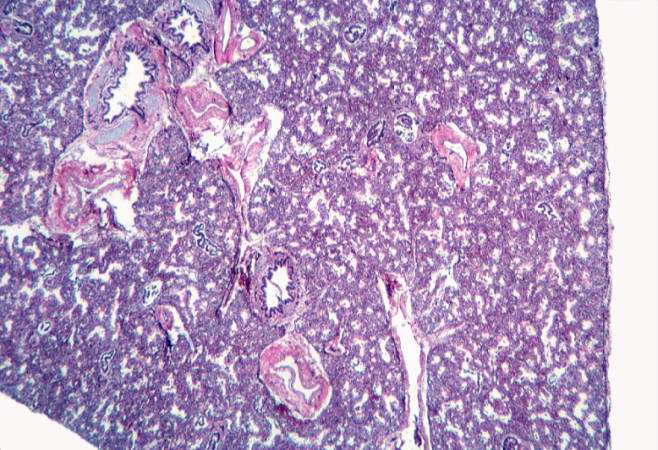
This low-power photomicrograph of lung demonstrates hypercellular pulmonary interstitium and small air spaces (as compared to adult lungs).
-
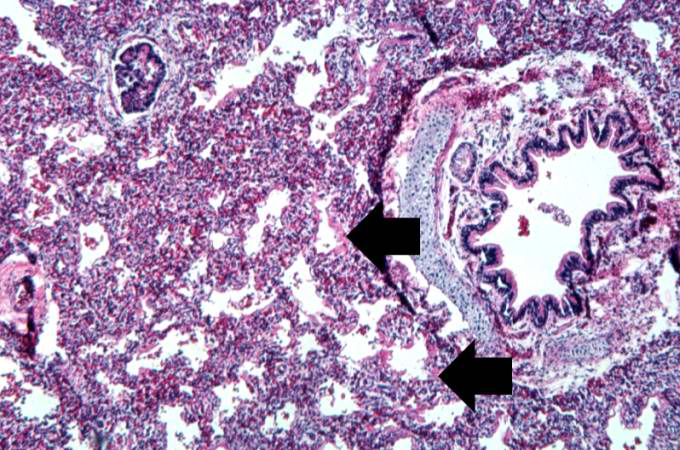
This is a medium-power photomicrograph showing a large bronchus with cartilage. Interstitial congestion with numerous red cells is apparent. Even at this magnification hyaline membranes (arrows) can be seen lining the alveoli.



-
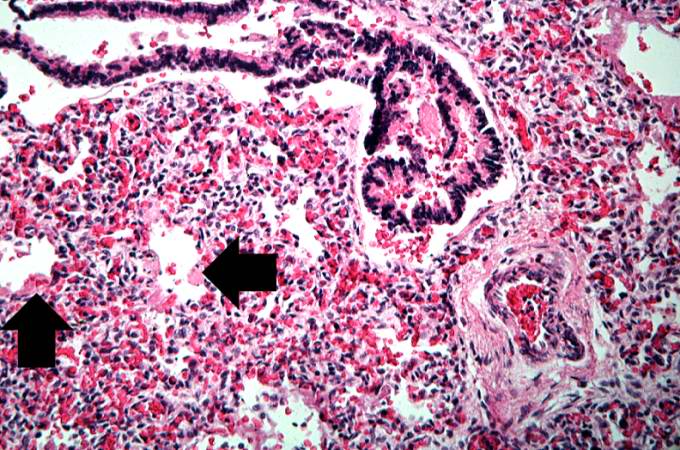
This high-power photomicrograph shows an airway with adjacent lung tissue. Some alveoli have hyaline membranes (arrows). There is severe congestion of the interstitium throughout this section.
-
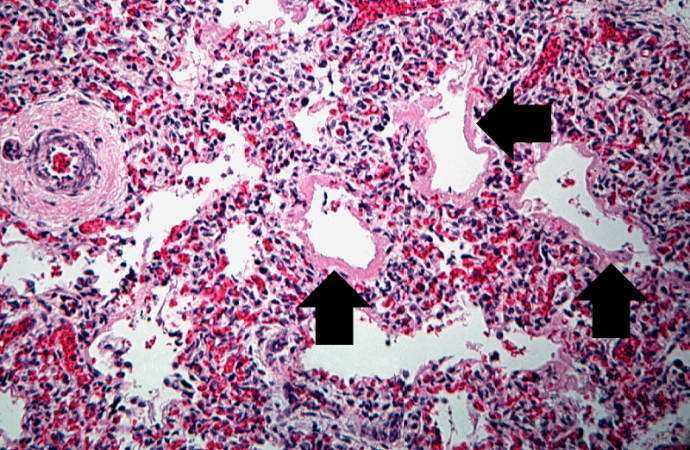
This medium-power photomicrograph shows the pink acellular homogeneous material lining the alveoli which comprises the hyaline membranes (arrows). The interstitium shows congestion, as in previous sections.
-
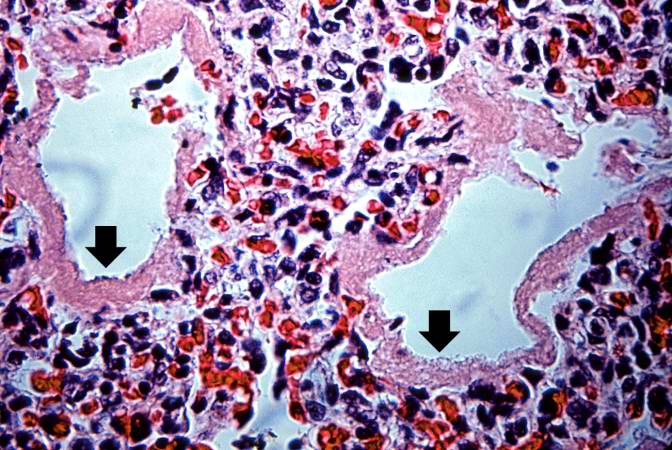
This higher-power photomicrograph shows more clearly the hyaline membranes (arrows) and the congestion in the interstitium.



Pathophysiology
The lungs are developmentally deficient in a material called surfactant, which allows the alveoli to remain open throughout the normal cycle of inhalation and exhalation. Surfactant is a complex system of lipids, proteins and glycoproteins which are produced in specialized lung cells called Type II cells or Type II pneumocytes. The surfactant is packaged by the cell in structures called lamellar bodies, and extruded into the alveoli. The lamellar bodies then unfold into a complex lining of the alveoli. This layer reduces the surface tension of the fluid that lines the alveolar walls. During exhalation the walls of the alveoli come in contact and surface tension tends to cause them to stick together, preventing re-inflation. By reducing surface tension, surfactant allows the alveoli to re-expand with inspiration. Without adequate amounts of surfactant, the alveoli collapse and are very difficult to expand. Microscopically, a surfactant deficient lung is characterized by collapsed alveoli alternating with hyperaerated alveoli, vascular congestion and, in time, hyaline membranes. Hyaline membranes are composed of fibrin, cellular debris, red blood cells, rare neutrophils and macrophages. They appear as an eosinophilic, amorphous material, lining or filling the alveolar spaces and blocking gas exchange.[2]. As a result, blood passing through the lungs is unable to pick up oxgen and unload carbon dioxide from the alveolar spaces. Blood oxygen levels fall and carbon dioxide rises, resulting in rising blood acid levels and hypoxia. Structural immaturity, as manifest by low numbers of alveoli, also contributes to the disease process. Therapeutic oxygen and positive-pressure ventilation, while potentially life-saving, can also damage the lung. The diagnosis is made by the clinical picture and the chest xray, which demonstrates decreased lung volumes (bell-shaped chest), absence of the thymus (after about 6 hours), a small (0.5-1 mm), discrete, uniform infiltrate (sometimes described as a "ground glass" appearance) that involves all lobes of the lung, and air-bronchograms (ie the infiltrate will outline the larger airways passages which remain air-filled). In severe cases, this becomes exaggerated until the cardiac borders become inapparent (a 'white-out' appearance).
Diagnosis
Imaging findings are
- Low lung volumes
- Bilateral granular opacities (represent areas of collapsed alveoli mixed with areas of open alveoli)
-

-

Post surfactant treatment


Prevention
Most cases of hyaline membrane disease can be ameliorated or prevented if mothers who are about to deliver prematurely can be given one of a group of hormones glucocorticoids. This speeds the production of surfactant. For very premature deliveries, a glucocorticoid is given without testing the fetal lung maturity. In pregnancies of greater than 30 weeks, the fetal lung maturity may be tested by sampling the amount of surfactant in the amniotic fluid, obtained by inserting a needle through the mother's abdomen and uterus. The 'maturity level' is expressed as the lecithin-sphingomyelin (or "L/S") ratio. If this ratio is less than 2, the fetal lungs may be surfactant deficient, and a glucocorticoid is given.
Treatment
Oxygen is given with a small amount of continuous positive airway pressure ("CPAP"), and intravenous fluids are administered to stabilize the blood sugar, blood salts, and blood pressure. If the baby's condition worsens, an endotracheal tube (breathing tube) is inserted into the trachea and intermittent breaths are given by a mechanical device. An exogenous preparation of surfactant, either synthetic or extracted from animal lungs, is given through the breathing tube into the lungs. One of the most commonly used surfactants is Survanta, derived from cow lungs, which can decrease the risk of death in hospitalized very-low-birth-weight infants by 30%[2]. Such small premature infants may remain ventilated for months. Chronic lung disease including bronchopulmonary dysplasia are common in severe RDS. The etiology of BPD is problematic and may be due to oxygen, overventilation or underventilation. The mortality rate for babies greater than 27 weeks gestation is less than 10%.
Related disorders
Acute respiratory distress syndrome (ARDS) has some similarities to IRDS.
References
{{reflist|2}]
Further reading
Wyman ML. "Neonatal Respiratory Distress" in Essentials of Pediatric Intensive Care (2 volume set) by Levin and Morriss, 1997.
Template:Certain conditions originating in the perinatal period
de:Atemnotsyndrom des Neugeborenen
- ↑ Rodriguez RJ, Martin RJ, and Fanaroff, AA. Respiratory distress syndrome and its management. Fanaroff and Martin (eds.) Neonatal-perinatal medicine: Diseases of the fetus and infant; 7th ed. (2002):1001-1011. St. Louis: Mosby.
- ↑ Schwartz, R.M., Luby, A.M., Scanlon, J.W., & Kellogg, R.J. Effect of surfactant on morbidity, mortality, and resource use in newborn infants weighing 500 to 1500 g. New England Journal of Medicine, 330 (1994): 1476-1480.