Follicular thyroid cancer pathophysiology
|
Follicular thyroid cancer Microchapters |
|
Differentiating Follicular thyroid cancer from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Follicular thyroid cancer pathophysiology On the Web |
|
American Roentgen Ray Society Images of Follicular thyroid cancer pathophysiology |
|
Risk calculators and risk factors for Follicular thyroid cancer pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
Follicular thyroid cancer arises from follicular cells of thyroid, which are secretory cells that are normally involved in production and secretion of thyroid hormones thyroxine (T4)and triiodothyronine (T3). Genes involved in the pathogenesis of Follicular thyroid cancer include Ras, PAX8/PPARγ, and PTEN.
Pathogenesis
- Follicular thyroid cancer is the second most common type of cancer. It constitute about 15% of thyroid cancers.

- This occurs more commonly in women of over 50 years old. Thyroglobulin (Tg) can be used as a tumor marker for well-differentiated follicular thyroid cancer. Follicular carcinoma tends to metastasize to the lungs and bone via the bloodstream, while papillary thyroid carcinoma commonly metastasizes to cervical lymph nodes.Unlike papillary it metastasises late to lymph nodes, with only 5-10% of patients having nodal metastases at the time of diagnosis. Haematogenous spread is however much more common with 20% or so of patients having distant haematogenous metastases at presentation.
Genetics
- The Ras oncogene is positive in a significant proportion of individuals. Ras oncogene act through the RAF-MEK-MAPK kinase pathway.
- Other genes involved in the pathogenesis of follicular thyroid cancer are as follows:
- RET/PTC (translocation) associated with MAPK and PI3K-AKT signaling pathways
- HRAS, KRAS, NRAS (mutation) associated with MAPK and PI3K-AKT signaling pathways
- PAX8/PPARγ (translocation) associated with PAX8-associated nuclear transcription signaling pathways. PAX8 is responsible for follicular cell differentiation.
- PTEN (mutation) associated with PI3K-AKT signaling pathways
- PTEN (deletion) associated with PI3K-AKT signaling pathways
- IDH1 (mutation) assciated with IDH1-associated metabolic pathways signaling pathways
- Phosphatase and tensin homologue suppressor gene and the phosphatidylinositol 3-kinase pathway are also involved in the pathogenesis of follicular thyroid tumor.
- p53, c-myc, c-fos, and the thyrotropin (TSH) receptor are some other factors involved in the pathogenesis of follicular thyroid cancer.
- MicroRNAs namely miR-192, miR-197, miR-328, and miR-346 have increased expression in follicular cell carcinoma.

Associated Conditions
- Cowden disease
- Carney complex, type I
Gross Pathology
- Encapsulated tumors

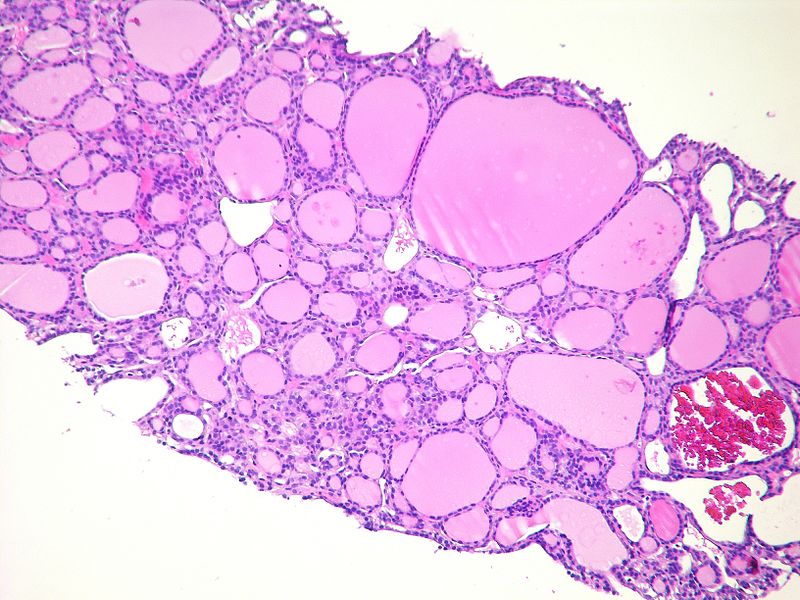
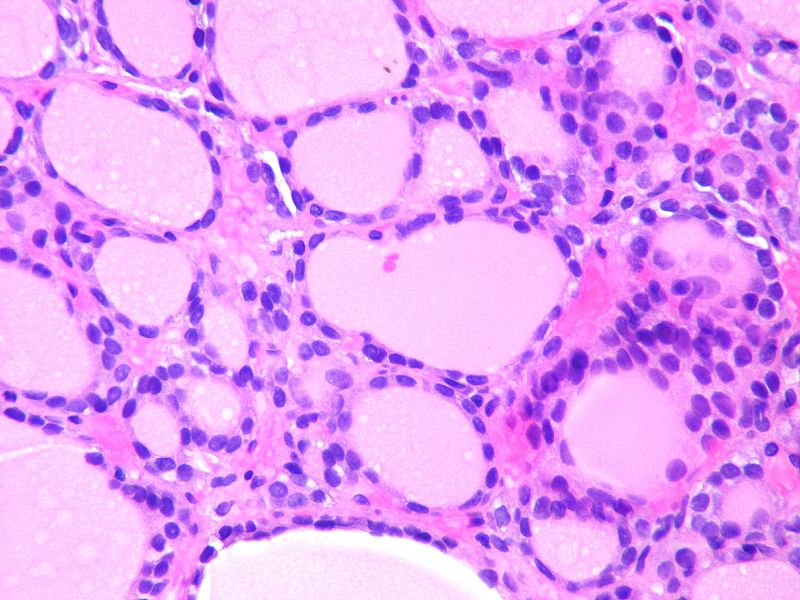
Microscopic Pathology
- It is not possible to distinguish between follicular adenoma and carcinoma on cytological grounds. If fine needle aspiration cytology (FNAC) suggests follicular neoplasm, thyroid lobectomy should be performed to establish the histopathological diagnosis.
- Trabecular, solid, follicular tumor cells that invade tumor capsule or surrounding vascular structures
-
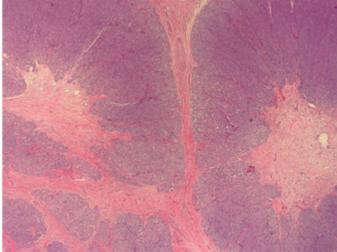
Thyroid, total thyroidectomy. Widely invasive follicular carcinoma, 4.5 cm, with lymphovascular invasion and extracapsular extension. Negative margins
-
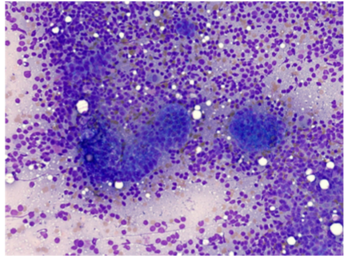
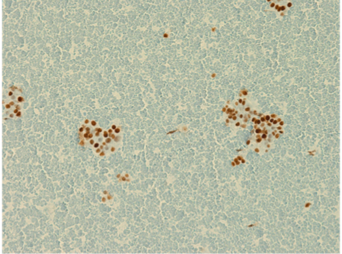
Lymph node FNA showing metastatic follicular carcinoma.
-
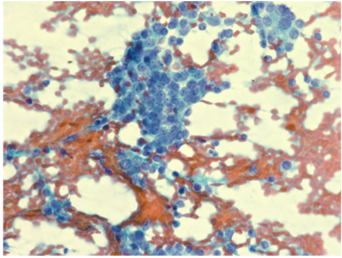
Lymph node FNA showing metastatic follicular carcinoma.
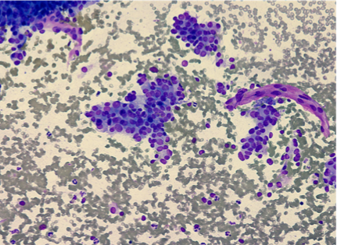
-

Lymph node FNA showing metastatic follicular carcinoma
-
C1 vertebrae biopsy positive for metastatic follicular carcinoma
-
C1 vertebrae biopsy positive for metastatic follicular carcinoma
-
Metastatic follicular carcinoma
-
Metastatic follicular carcinoma






.jpg)

Video
{{#ev:youtube|3_eCHeOkdgg}}