Endocarditis pathophysiology: Difference between revisions
No edit summary |
|||
| Line 50: | Line 50: | ||
* The exact pathogenesis of nonbacterial thrombotic endocarditis is not completely understood. | * The exact pathogenesis of nonbacterial thrombotic endocarditis is not completely understood. | ||
*[[Nonbacterial thrombotic endocarditis]] (NBTE), also called | *[[Nonbacterial thrombotic endocarditis]] (NBTE), also called marantic endocarditis is most commonly found on previously undamaged valves. | ||
*The vegetations in nonbacterial thrombotic endocarditis are sterile and small. | *The vegetations in nonbacterial thrombotic endocarditis are sterile and small. | ||
*The vegetations mostly aggregate at the edges of the valve or the cusps. | *The vegetations mostly aggregate at the edges of the valve or the cusps. | ||
* We can divide the pathogenesis pathway of nonbacterial endocarditis into to phase: | * We can divide the pathogenesis pathway of nonbacterial endocarditis into to phase: | ||
** Initiating phase | ** Initiating phase | ||
*** Immune complexes<ref name="pmid3135393">{{cite journal |vauthors=Ford PM, Ford SE, Lillicrap DP |title=Association of lupus anticoagulant with severe valvular heart disease in systemic lupus erythematosus |journal=J. Rheumatol. |volume=15 |issue=4 |pages=597–600 |date=April 1988 |pmid=3135393 |doi= |url=}}</ref><ref>{{cite book | last = Williams | first = Ralph | title = Immune complexes in clinical and experimental medicine | publisher = Harvard University Press | location = Cambridge, Mass | year = 1980 | isbn = 978-0674444386 }}</ref> | *** Immune complexes:<ref name="pmid3135393">{{cite journal |vauthors=Ford PM, Ford SE, Lillicrap DP |title=Association of lupus anticoagulant with severe valvular heart disease in systemic lupus erythematosus |journal=J. Rheumatol. |volume=15 |issue=4 |pages=597–600 |date=April 1988 |pmid=3135393 |doi= |url=}}</ref><ref>{{cite book | last = Williams | first = Ralph | title = Immune complexes in clinical and experimental medicine | publisher = Harvard University Press | location = Cambridge, Mass | year = 1980 | isbn = 978-0674444386 }}</ref> | ||
**** | ****Circulating immune complexes and complement deposition can initiate the process. | ||
****The example for this initiating factor in libman sacks endocarditis in lupus patients. | ****The example for this initiating factor in libman sacks endocarditis in lupus patients. | ||
*** Hypoxia<ref name="pmid9808440">{{cite journal |vauthors=Nakanishi K, Tajima F, Nakata Y, Osada H, Ogata K, Kawai T, Torikata C, Suga T, Takishima K, Aurues T, Ikeda T |title=Tissue factor is associated with the nonbacterial thrombotic endocarditis induced by a hypobaric hypoxic environment in rats |journal=Virchows Arch. |volume=433 |issue=4 |pages=375–9 |date=October 1998 |pmid=9808440 |doi=10.1007/s004280050262 |url=}}</ref><ref name="pmid11355169">{{cite journal |vauthors=Truskinovsky AM, Hutchins GM |title=Association between nonbacterial thrombotic endocarditis and hypoxigenic pulmonary diseases |journal=Virchows Arch. |volume=438 |issue=4 |pages=357–61 |date=April 2001 |pmid=11355169 |doi=10.1007/s004280000372 |url=}}</ref> | *** Hypoxia:<ref name="pmid9808440">{{cite journal |vauthors=Nakanishi K, Tajima F, Nakata Y, Osada H, Ogata K, Kawai T, Torikata C, Suga T, Takishima K, Aurues T, Ikeda T |title=Tissue factor is associated with the nonbacterial thrombotic endocarditis induced by a hypobaric hypoxic environment in rats |journal=Virchows Arch. |volume=433 |issue=4 |pages=375–9 |date=October 1998 |pmid=9808440 |doi=10.1007/s004280050262 |url=}}</ref><ref name="pmid11355169">{{cite journal |vauthors=Truskinovsky AM, Hutchins GM |title=Association between nonbacterial thrombotic endocarditis and hypoxigenic pulmonary diseases |journal=Virchows Arch. |volume=438 |issue=4 |pages=357–61 |date=April 2001 |pmid=11355169 |doi=10.1007/s004280000372 |url=}}</ref> | ||
****Some studies demonstrated that hypoxia may lead to tissue factor activation. | ****Some studies demonstrated that hypoxia may lead to tissue factor activation. | ||
****Higher tissue factor level has an association with higher rate of endocarditis. | ****Higher tissue factor level has an association with higher rate of endocarditis. | ||
****Other studies implies that the rate of endocarditis is higher in smokers and patients with chronic lung disease and possibly hypoxia. | ****Other studies implies that the rate of endocarditis is higher in smokers and patients with chronic lung disease and possibly hypoxia. | ||
*** Hypercoagulability<ref name="pmid13403513">{{cite journal |vauthors=MACDONALD RA, ROBBINS SL |title=The significance of nonbacterial thrombotic endocarditis: an autopsy and clinical study of 78 cases |journal=Ann. Intern. Med. |volume=46 |issue=2 |pages=255–73 |date=February 1957 |pmid=13403513 |doi=10.7326/0003-4819-46-2-255 |url=}}</ref><ref name="pmid834136">{{cite journal |vauthors=Sack GH, Levin J, Bell WR |title=Trousseau's syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: clinical, pathophysiologic, and therapeutic features |journal=Medicine (Baltimore) |volume=56 |issue=1 |pages=1–37 |date=January 1977 |pmid=834136 |doi= |url=}}</ref> | *** Hypercoagulability:<ref name="pmid13403513">{{cite journal |vauthors=MACDONALD RA, ROBBINS SL |title=The significance of nonbacterial thrombotic endocarditis: an autopsy and clinical study of 78 cases |journal=Ann. Intern. Med. |volume=46 |issue=2 |pages=255–73 |date=February 1957 |pmid=13403513 |doi=10.7326/0003-4819-46-2-255 |url=}}</ref><ref name="pmid834136">{{cite journal |vauthors=Sack GH, Levin J, Bell WR |title=Trousseau's syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: clinical, pathophysiologic, and therapeutic features |journal=Medicine (Baltimore) |volume=56 |issue=1 |pages=1–37 |date=January 1977 |pmid=834136 |doi= |url=}}</ref> | ||
****There is an association between hypercoagulable state and clotting factor abnormalities with initiation of nonbacterial thrombotic endocarditis. | ****There is an association between hypercoagulable state and clotting factor abnormalities with initiation of nonbacterial thrombotic endocarditis. | ||
***** | ***** | ||
*** Carcinomatosis<ref name="pmid4577065">{{cite journal |vauthors=Gralnick HR, Abrell E |title=Studies of the procoagulant and fibrinolytic activity of promyelocytes in acute promyelocytic leukaemia |journal=Br. J. Haematol. |volume=24 |issue=1 |pages=89–99 |date=January 1973 |pmid=4577065 |doi=10.1111/j.1365-2141.1973.tb05730.x |url=}}</ref> | *** Carcinomatosis:<ref name="pmid4577065">{{cite journal |vauthors=Gralnick HR, Abrell E |title=Studies of the procoagulant and fibrinolytic activity of promyelocytes in acute promyelocytic leukaemia |journal=Br. J. Haematol. |volume=24 |issue=1 |pages=89–99 |date=January 1973 |pmid=4577065 |doi=10.1111/j.1365-2141.1973.tb05730.x |url=}}</ref> | ||
****The association between cancer and nonbacterial thrombotic endocarditis is well established. | ****The association between cancer and nonbacterial thrombotic endocarditis is well established. | ||
****In most of the cases of cancer related endocarditis we have abnormal activity of tissue factor. | ****In most of the cases of cancer related endocarditis we have abnormal activity of tissue factor. | ||
| Line 82: | Line 82: | ||
Genes involved in the pathogenesis of nonbacterial thrombotic endocarditis include:<ref name="pmid21560828">{{cite journal |vauthors=Durante-Mangoni E, Iossa D, Nappi F, Utili R |title=Inherited hyper-homocysteinemia as a cause of nonbacterial thrombotic endocarditis |journal=J. Heart Valve Dis. |volume=20 |issue=2 |pages=232–3 |date=March 2011 |pmid=21560828 |doi= |url=}}</ref> | Genes involved in the pathogenesis of nonbacterial thrombotic endocarditis include:<ref name="pmid21560828">{{cite journal |vauthors=Durante-Mangoni E, Iossa D, Nappi F, Utili R |title=Inherited hyper-homocysteinemia as a cause of nonbacterial thrombotic endocarditis |journal=J. Heart Valve Dis. |volume=20 |issue=2 |pages=232–3 |date=March 2011 |pmid=21560828 |doi= |url=}}</ref> | ||
* Homozygous for the C677T mutation of the methylenetetrahydrofolate reductase gene which leads to hyper-homocysteinemia. | * Homozygous for the C677T mutation of the [[Methylenetetrahydrofolate-tRNA-(uracil-5-)-methyltransferase|methylenetetrahydrofolate]] reductase gene which leads to [[Hyperhomocysteinemia|hyper-homocysteinemia]]. | ||
* | * | ||
| Line 108: | Line 108: | ||
| align="center" style="background: #4479BA;" | {{fontcolor|#FFF|'''Features on Gross Pathology'''}} | | align="center" style="background: #4479BA;" | {{fontcolor|#FFF|'''Features on Gross Pathology'''}} | ||
|- | |- | ||
! Infective Endocarditis | |||
| | |||
*Left-sided valve involvement (mitral, aortic) more common generally | *Left-sided valve involvement (mitral, aortic) more common generally | ||
*Right-sided valve involvement (pulmonic, tricuspid valve) more common in intravenous drug abusers | *Right-sided valve involvement (pulmonic, tricuspid valve) more common in intravenous drug abusers | ||
| Line 114: | Line 115: | ||
*Valvular destruction | *Valvular destruction | ||
|- | |- | ||
! Nonbacterial Thrombotic Endocarditis | |||
| | |||
*Round non-destructive vegetations, usually at the line of closure | *Round non-destructive vegetations, usually at the line of closure | ||
|- | |- | ||
| Line 122: | Line 124: | ||
On microscopic histopathological, characteristic findings of endocarditis are: | On microscopic histopathological, characteristic findings of endocarditis are: | ||
* Vegetation | * Vegetation: | ||
** Vegetations are composed of fibrin, inflammatory cells, platelets, and microorganisms.<ref name="pmid11794152">{{cite journal| author=Mylonakis E, Calderwood SB| title=Infective endocarditis in adults. | journal=N Engl J Med | year= 2001 | volume= 345 | issue= 18 | pages= 1318-30 | pmid=11794152 | doi=10.1056/NEJMra010082 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11794152 }}</ref> <ref> Infective Endocarditis. Libre Pathology (2015). URL=http://librepathology.org/wiki/index.php/Infective_endocarditis Accessed on September 21, 2015</ref> | ** Vegetations are composed of fibrin, inflammatory cells, platelets, and microorganisms.<ref name="pmid11794152">{{cite journal| author=Mylonakis E, Calderwood SB| title=Infective endocarditis in adults. | journal=N Engl J Med | year= 2001 | volume= 345 | issue= 18 | pages= 1318-30 | pmid=11794152 | doi=10.1056/NEJMra010082 | pmc= | url=http://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=11794152 }}</ref> <ref> Infective Endocarditis. Libre Pathology (2015). URL=http://librepathology.org/wiki/index.php/Infective_endocarditis Accessed on September 21, 2015</ref> | ||
| Line 129: | Line 131: | ||
| align="center" style="background: #4479BA;" |{{fontcolor|#FFF|'''Features on Histopathological Microscopic Analysis'''}} | | align="center" style="background: #4479BA;" |{{fontcolor|#FFF|'''Features on Histopathological Microscopic Analysis'''}} | ||
|- | |- | ||
! Infective Endocarditis | |||
| | | | ||
*Inflammatory infiltrate | *Inflammatory infiltrate | ||
| Line 136: | Line 138: | ||
*Microorganisms present | *Microorganisms present | ||
|- | |- | ||
! Nonbacterial Thrombotic Endocarditis | |||
| | | | ||
*Vegetations without inflammation and microorganisms | *Vegetations without inflammation and microorganisms | ||
| Line 144: | Line 146: | ||
[http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] | [http://www.peir.net Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] | ||
<div align="left"> | <div align="left"><gallery heights="150" widths="150"> | ||
<gallery heights="150" widths="150"> | |||
Image:Breast intraductal papilloma metastasis.jpg|Heart; Breast intraductal papilloma metastasis. Thrombotic Nonbacterial Endocarditis (Infected): Gross mitral valve natural color vegetations well illustrated these were secondarily infected with staphylococcus case of 8 year survival breast intraductal papillary adenocarcinoma with extensive metastases. Aortic valve also involved. | Image:Breast intraductal papilloma metastasis.jpg|Heart; Breast intraductal papilloma metastasis. Thrombotic Nonbacterial Endocarditis (Infected): Gross mitral valve natural color vegetations well illustrated these were secondarily infected with staphylococcus case of 8 year survival breast intraductal papillary adenocarcinoma with extensive metastases. Aortic valve also involved. | ||
Image:Papillar intraductal carcinoma metastasis to heart.JPG|Nonbacterial Thrombotic Endocarditis Infected: Micro low mag H&E fibrin vegetation with masses of staphylococci and inflammatory cells in valve secondarily infected case 8 year survival breast papillary intraductal adenocarcinoma with extensive metastases gross is aortic valve lesions. | Image:Papillar intraductal carcinoma metastasis to heart.JPG|Nonbacterial Thrombotic Endocarditis Infected: Micro low mag H&E fibrin vegetation with masses of staphylococci and inflammatory cells in valve secondarily infected case 8 year survival breast papillary intraductal adenocarcinoma with extensive metastases gross is aortic valve lesions. | ||
Revision as of 21:03, 3 March 2020
| https://https://www.youtube.com/watch?v=kW-85yk0ErQ%7C350}} |
|
Endocarditis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease |
|
Case Studies |
|
Endocarditis pathophysiology On the Web |
|
Risk calculators and risk factors for Endocarditis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
The pathogenesis of infective endocarditis includes valvular damage, altered and turbulent flow, bacteremia, and lack of blood supply to the valves. Damaged endothelium becomes a site for attachment of infectious agents in infectious endocarditis. Nonbacterial thrombotic endocarditis is related to hypercoaguable states such as pregnancy or systemic bacterial infection. The characteristic lesion of endocarditis is a vegetation. Vegetations are composed of fibrin, inflammatory cells, platelets, and microorganisms.
Pathophysiology
Pathogenesis
Infective Endocarditis
| Pathogenic Factors | Mechanism |
|---|---|
|
|
|
|
|
|
Nonbacterial Thrombotic Endocarditis
- The exact pathogenesis of nonbacterial thrombotic endocarditis is not completely understood.
- Nonbacterial thrombotic endocarditis (NBTE), also called marantic endocarditis is most commonly found on previously undamaged valves.
- The vegetations in nonbacterial thrombotic endocarditis are sterile and small.
- The vegetations mostly aggregate at the edges of the valve or the cusps.
- We can divide the pathogenesis pathway of nonbacterial endocarditis into to phase:
- Initiating phase
- Immune complexes:[3][4]
- Circulating immune complexes and complement deposition can initiate the process.
- The example for this initiating factor in libman sacks endocarditis in lupus patients.
- Hypoxia:[5][6]
- Some studies demonstrated that hypoxia may lead to tissue factor activation.
- Higher tissue factor level has an association with higher rate of endocarditis.
- Other studies implies that the rate of endocarditis is higher in smokers and patients with chronic lung disease and possibly hypoxia.
- Hypercoagulability:[7][8]
- There is an association between hypercoagulable state and clotting factor abnormalities with initiation of nonbacterial thrombotic endocarditis.
- There is an association between hypercoagulable state and clotting factor abnormalities with initiation of nonbacterial thrombotic endocarditis.
- Carcinomatosis:[9]
- The association between cancer and nonbacterial thrombotic endocarditis is well established.
- In most of the cases of cancer related endocarditis we have abnormal activity of tissue factor.
- Tissue factor may be secreted from promyelocytic leukaemia cells.
- Tissue factor may be expressed on the surface of adenocarcinoma cells which leads to increased expression of tissue factor by endothelial cells.
- Immune complexes:[3][4]
- Verrucae formation
- Initiating phase
Genetics
Genes involved in the pathogenesis of infective endocarditis include:[10]
- Interleukin-6 c.471+870G>A
- Interleukin-1b c.315C>T
- Selectin-E c.-19 GT
Genes involved in the pathogenesis of nonbacterial thrombotic endocarditis include:[11]
- Homozygous for the C677T mutation of the methylenetetrahydrofolate reductase gene which leads to hyper-homocysteinemia.
Associated Conditions
Conditions associated with endocarditis include:
- Prosthetic heart valves[12]
- Valvular heart disease (mitral valve prolapse is the most common valvular lesion that predisposes to endocarditis)[13][14]
- Intravenous drug abuse[15]
- Intracardiac devices, such as implantable cardioverter-defibrillators[16]
- Hemodialysis[17]
- Congenital heart disease[18]
- History of rheumatic heart disease[19]
- Diabetes mellitus[20][21]
- Colon cancer[22]
- Hypercoagulable state such as pregnancy and systemic bacterial infection [23][24]
- Malignancy especially mucin-producing adenocarcinomas (most commonly associated with pancreatic adenocarcinomas)[25]
- Systemic lupus erythematosus[26]
Gross Pathology
On gross pathology, characteristic findings of endocarditis are:
| Endocarditis Subtype | Features on Gross Pathology |
| Infective Endocarditis |
|
|---|---|
| Nonbacterial Thrombotic Endocarditis |
|
Microscopic Pathology
On microscopic histopathological, characteristic findings of endocarditis are:
- Vegetation:
| Endocarditis Subtype | Features on Histopathological Microscopic Analysis |
| Infective Endocarditis |
|
|---|---|
| Nonbacterial Thrombotic Endocarditis |
|
-
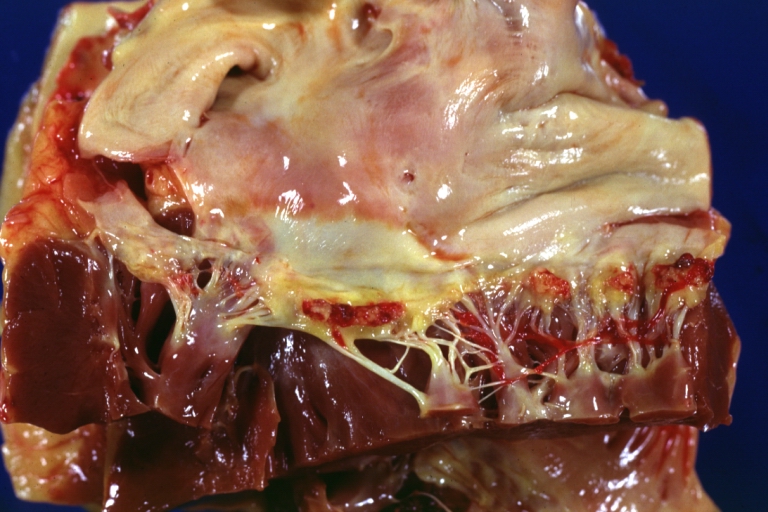
Heart; Breast intraductal papilloma metastasis. Thrombotic Nonbacterial Endocarditis (Infected): Gross mitral valve natural color vegetations well illustrated these were secondarily infected with staphylococcus case of 8 year survival breast intraductal papillary adenocarcinoma with extensive metastases. Aortic valve also involved.
-
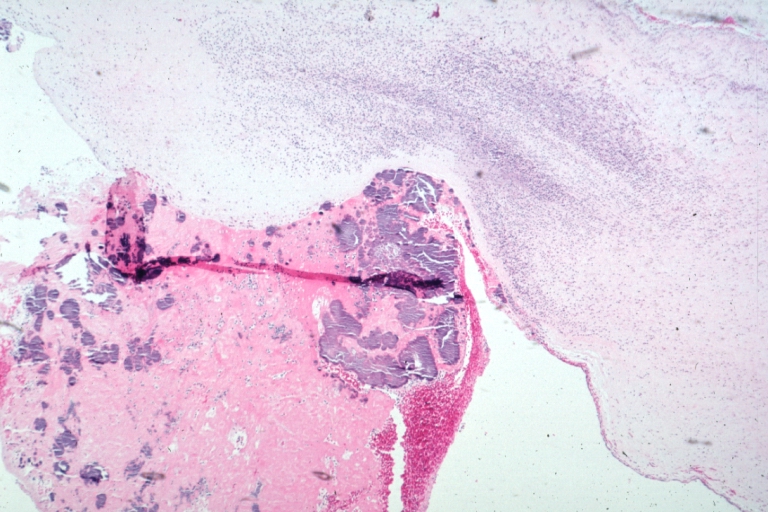
Nonbacterial Thrombotic Endocarditis Infected: Micro low mag H&E fibrin vegetation with masses of staphylococci and inflammatory cells in valve secondarily infected case 8 year survival breast papillary intraductal adenocarcinoma with extensive metastases gross is aortic valve lesions.


Videos
{{#ev:youtube|gk7cpP2ymOs}} {{#ev:youtube|BiNulEFh6rU}}
References
- ↑ Infective endocarditis. Wikipedia (2015). https://en.wikipedia.org/wiki/Infective_endocarditis#Pathogenesis Accessed on September 21, 2015
- ↑ Endocarditis. Wikipedia (2015). https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015
- ↑ Ford PM, Ford SE, Lillicrap DP (April 1988). "Association of lupus anticoagulant with severe valvular heart disease in systemic lupus erythematosus". J. Rheumatol. 15 (4): 597–600. PMID 3135393.
- ↑ Williams, Ralph (1980). Immune complexes in clinical and experimental medicine. Cambridge, Mass: Harvard University Press. ISBN 978-0674444386.
- ↑ Nakanishi K, Tajima F, Nakata Y, Osada H, Ogata K, Kawai T, Torikata C, Suga T, Takishima K, Aurues T, Ikeda T (October 1998). "Tissue factor is associated with the nonbacterial thrombotic endocarditis induced by a hypobaric hypoxic environment in rats". Virchows Arch. 433 (4): 375–9. doi:10.1007/s004280050262. PMID 9808440.
- ↑ Truskinovsky AM, Hutchins GM (April 2001). "Association between nonbacterial thrombotic endocarditis and hypoxigenic pulmonary diseases". Virchows Arch. 438 (4): 357–61. doi:10.1007/s004280000372. PMID 11355169.
- ↑ MACDONALD RA, ROBBINS SL (February 1957). "The significance of nonbacterial thrombotic endocarditis: an autopsy and clinical study of 78 cases". Ann. Intern. Med. 46 (2): 255–73. doi:10.7326/0003-4819-46-2-255. PMID 13403513.
- ↑ Sack GH, Levin J, Bell WR (January 1977). "Trousseau's syndrome and other manifestations of chronic disseminated coagulopathy in patients with neoplasms: clinical, pathophysiologic, and therapeutic features". Medicine (Baltimore). 56 (1): 1–37. PMID 834136.
- ↑ Gralnick HR, Abrell E (January 1973). "Studies of the procoagulant and fibrinolytic activity of promyelocytes in acute promyelocytic leukaemia". Br. J. Haematol. 24 (1): 89–99. doi:10.1111/j.1365-2141.1973.tb05730.x. PMID 4577065.
- ↑ Weinstock M, Grimm I, Dreier J, Knabbe C, Vollmer T (2014). "Genetic variants in genes of the inflammatory response in association with infective endocarditis". PLoS ONE. 9 (10): e110151. doi:10.1371/journal.pone.0110151. PMC 4192365. PMID 25299518.
- ↑ Durante-Mangoni E, Iossa D, Nappi F, Utili R (March 2011). "Inherited hyper-homocysteinemia as a cause of nonbacterial thrombotic endocarditis". J. Heart Valve Dis. 20 (2): 232–3. PMID 21560828.
- ↑ Arvay A, Lengyel M (1988). "Incidence and risk factors of prosthetic valve endocarditis". Eur J Cardiothorac Surg. 2 (5): 340–6. PMID 3272238.
- ↑ Mylonakis E, Calderwood SB (2001). "Infective endocarditis in adults". N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152.
- ↑ Corrigall, Denton; Bolen, James; Hancock, E.William; Popp, Richard L. (1977). "Mitral valve prolapse and infective endocarditis". The American Journal of Medicine. 63 (2): 215–222. doi:10.1016/0002-9343(77)90235-2. ISSN 0002-9343.
- ↑ Sousa, C.; Botelho, C.; Rodrigues, D.; Azeredo, J.; Oliveira, R. (2012). "Infective endocarditis in intravenous drug abusers: an update". European Journal of Clinical Microbiology & Infectious Diseases. 31 (11): 2905–2910. doi:10.1007/s10096-012-1675-x. ISSN 0934-9723.
- ↑ Sohail, Muhammad R.; Uslan, Daniel Z.; Khan, Akbar H.; Friedman, Paul A.; Hayes, David L.; Wilson, Walter R.; Steckelberg, James M.; Jenkins, Sarah M.; Baddour, Larry M. (2008). "Infective Endocarditis Complicating Permanent Pacemaker and Implantable Cardioverter-Defibrillator Infection". Mayo Clinic Proceedings. 83 (1): 46–53. doi:10.4065/83.1.46. ISSN 0025-6196.
- ↑ Mccarthy, James T.; Steckelberg, James M. (2000). "Infective Endocarditis in Patients Receiving Long-term Hemodialysis". Mayo Clinic Proceedings. 75 (10): 1008–1014. doi:10.4065/75.10.1008. ISSN 0025-6196.
- ↑ Knirsch, Walter; Nadal, David (2011). "Infective endocarditis in congenital heart disease". European Journal of Pediatrics. 170 (9): 1111–1127. doi:10.1007/s00431-011-1520-8. ISSN 0340-6199.
- ↑ Strom BL, Abrutyn E, Berlin JA, Kinman JL, Feldman RS, Stolley PD, Levison ME, Korzeniowski OM, Kaye D (November 1998). "Dental and cardiac risk factors for infective endocarditis. A population-based, case-control study". Ann. Intern. Med. 129 (10): 761–9. doi:10.7326/0003-4819-129-10-199811150-00002. PMID 9841581.
- ↑ Lin CJ, Chua S, Chung SY, Hang CL, Tsai TH (June 2019). "Diabetes Mellitus: An Independent Risk Factor of In-Hospital Mortality in Patients with Infective Endocarditis in a New Era of Clinical Practice". Int J Environ Res Public Health. 16 (12). doi:10.3390/ijerph16122248. PMC 6617149 Check
|pmc=value (help). PMID 31242695. - ↑ Chirillo F, Bacchion F, Pedrocco A, Scotton P, De Leo A, Rocco F, Valfrè C, Olivari Z (May 2010). "Infective endocarditis in patients with diabetes mellitus". J. Heart Valve Dis. 19 (3): 312–20. PMID 20583393.
- ↑ Lazarovitch, T.; Shango, M.; Levine, M.; Brusovansky, R.; Akins, R.; Hayakawa, K.; Lephart, P. R.; Sobel, J. D.; Kaye, K. S.; Marchaim, D. (2012). "The relationship between the new taxonomy of Streptococcus bovis and its clonality to colon cancer, endocarditis, and biliary disease". Infection. 41 (2): 329–337. doi:10.1007/s15010-012-0314-x. ISSN 0300-8126.
- ↑ "THE SIGNIFICANCE OF NONBACTERIAL THROMBOTIC ENDOCARDITIS: AN AUTOPSY AND CLINICAL STUDY OF 78 CASES". Annals of Internal Medicine. 46 (2): 255. 1957. doi:10.7326/0003-4819-46-2-255. ISSN 0003-4819.
- ↑ Horwitz, Charles A.; Ward, Patrick C.J. (1971). "Disseminated intravascular coagulation, nonbacterial thrombotic endocarditis and adult pulmonary hyaline membranes-an interrelated triad?". The American Journal of Medicine. 51 (2): 272–280. doi:10.1016/0002-9343(71)90245-2. ISSN 0002-9343.
- ↑ Min, Kyung-Whan; Gyorkey, Ferene; Sato, Clifford (1980). "Mucin-producing adenocarcinomas and nonbacterial thrombotic endocarditis. Pathogenetic role of tumor mucin". Cancer. 45 (9): 2374–2382. doi:10.1002/1097-0142(19800501)45:9<2374::AID-CNCR2820450923>3.0.CO;2-J. ISSN 0008-543X.
- ↑ Moyssakis, Ioannis; Tektonidou, Maria G.; Vasilliou, Vassilios A.; Samarkos, Michael; Votteas, Vassilios; Moutsopoulos, Haralampos M. (2007). "Libman-Sacks Endocarditis in Systemic Lupus Erythematosus: Prevalence, Associations, and Evolution". The American Journal of Medicine. 120 (7): 636–642. doi:10.1016/j.amjmed.2007.01.024. ISSN 0002-9343.
- ↑ Mylonakis E, Calderwood SB (2001). "Infective endocarditis in adults". N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152.
- ↑ Infective Endocarditis. Libre Pathology (2015). URL=http://librepathology.org/wiki/index.php/Infective_endocarditis Accessed on September 21, 2015