Endocarditis pathophysiology: Difference between revisions
| Line 44: | Line 44: | ||
====Nonbacterial thrombotic endocarditis==== | ====Nonbacterial thrombotic endocarditis==== | ||
[[Nonbacterial thrombotic endocarditis]] (NBTE), also called '''marantic endocarditis''' is most commonly found on previously undamaged valves.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> As opposed to infective endocarditis, the vegetations in NBTE are small, sterile, and tend to aggregate along the edges of the valve or the cusps.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> Also unlike infective endocarditis, NBTE does not cause an inflammation response from the body.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> NBTE usually occurs due to hypercoaguable states such as systemic bacterial infection or pregnancy.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> NBTE may also occur in patients with [[cancer]], particularly mucinous [[adenocarcinoma]].<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> [[Libman-Sacks endocarditis]] is another form of sterile endocarditis; this form occurs more often in patients with [[lupus erythematosus]] and is thought to be due to the deposition of immune complexes. [[Libman-Sacks endocarditis]] involves small | [[Nonbacterial thrombotic endocarditis]] (NBTE), also called '''marantic endocarditis''' is most commonly found on previously undamaged valves.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> As opposed to infective endocarditis, the vegetations in NBTE are small, sterile, and tend to aggregate along the edges of the valve or the cusps.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> Also unlike infective endocarditis, NBTE does not cause an inflammation response from the body.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> NBTE usually occurs due to hypercoaguable states such as systemic bacterial infection or pregnancy.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> NBTE may also occur in patients with [[cancer]], particularly mucinous [[adenocarcinoma]].<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> [[Libman-Sacks endocarditis]] is another form of sterile endocarditis; this form occurs more often in patients with [[lupus erythematosus]] and is thought to be due to the deposition of immune complexes. [[Libman-Sacks endocarditis]] involves small vegetations, while infective endocarditis is composed of large vegetations.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> These immune complexes precipitate an inflammatory reaction, which helps to differentiate it from NBTE.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> Also unlike NBTE, Libman-Sacks endocarditis does not seem to have a preferred location of deposition and may form on the undersurfaces of the valves or even on the endocardium.<ref name=endo> Endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015</ref> | ||
===Gross and Microscopic Pathology=== | ===Gross and Microscopic Pathology=== | ||
Revision as of 13:28, 23 September 2015
|
Endocarditis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease |
|
Case Studies |
|
Endocarditis pathophysiology On the Web |
|
Risk calculators and risk factors for Endocarditis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
The turbulent blood flow around the heart valves is a risk factor for the development of endocarditis. The valves may be damaged congenitally, from surgery, by auto-immune mechanisms, or simply as a consequence of old age. The damaged endothelium of these areas becomes a site for attachment of infectious agents in infectious endocarditis. Dental procedures, colorectal cancer, urinary tract infections and intravenous drug use are the most common routes of introducing the infectious agent into the bloodstream. In non-bacterial thrombotic endocarditis (NBTE), the damaged part of a heart valve becomes covered with a blood clot which organizes.
Pathophysiology
Pathogenesis
Infective Endocarditis
The pathogenesis of infective endocarditis includes:[1][2]
| Pathogenic Factors | Mechanism |
|---|---|
|
|
|
|
|
|
Nonbacterial thrombotic endocarditis
Nonbacterial thrombotic endocarditis (NBTE), also called marantic endocarditis is most commonly found on previously undamaged valves.[2] As opposed to infective endocarditis, the vegetations in NBTE are small, sterile, and tend to aggregate along the edges of the valve or the cusps.[2] Also unlike infective endocarditis, NBTE does not cause an inflammation response from the body.[2] NBTE usually occurs due to hypercoaguable states such as systemic bacterial infection or pregnancy.[2] NBTE may also occur in patients with cancer, particularly mucinous adenocarcinoma.[2] Libman-Sacks endocarditis is another form of sterile endocarditis; this form occurs more often in patients with lupus erythematosus and is thought to be due to the deposition of immune complexes. Libman-Sacks endocarditis involves small vegetations, while infective endocarditis is composed of large vegetations.[2] These immune complexes precipitate an inflammatory reaction, which helps to differentiate it from NBTE.[2] Also unlike NBTE, Libman-Sacks endocarditis does not seem to have a preferred location of deposition and may form on the undersurfaces of the valves or even on the endocardium.[2]
Gross and Microscopic Pathology
Characteristic features of endocarditis on gross pathology and histopathological analysis include:[3]
| Endocarditis Subtype | Features on Gross Pathology | Features on Histopathological Microscopic Analysis |
| Infective Endocarditis |
|
|
| Nonbacterial Thrombotic Endocarditis |
|
|
Pathology
-
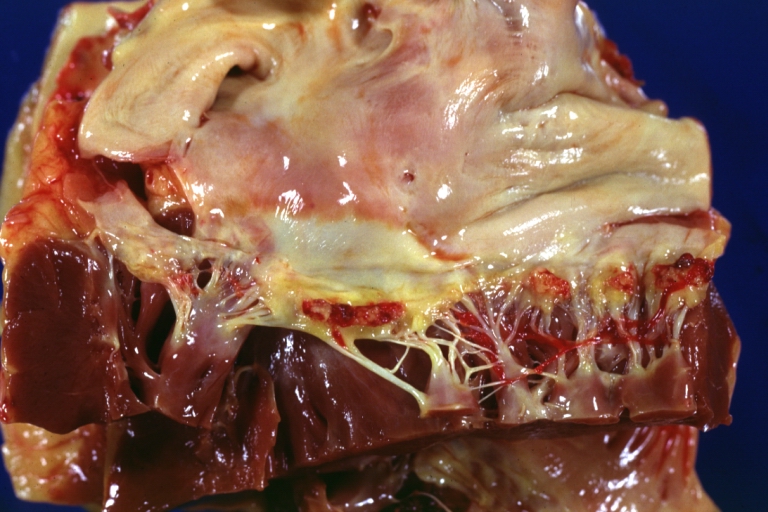
Heart; Breast intraductal papilloma metastasis. Thrombotic Nonbacterial Endocarditis (Infected): Gross mitral valve natural color vegetations well illustrated these were secondarily infected with staphylococcus case of 8 year survival breast intraductal papillary adenocarcinoma with extensive metastases. Aortic valve also involved
-
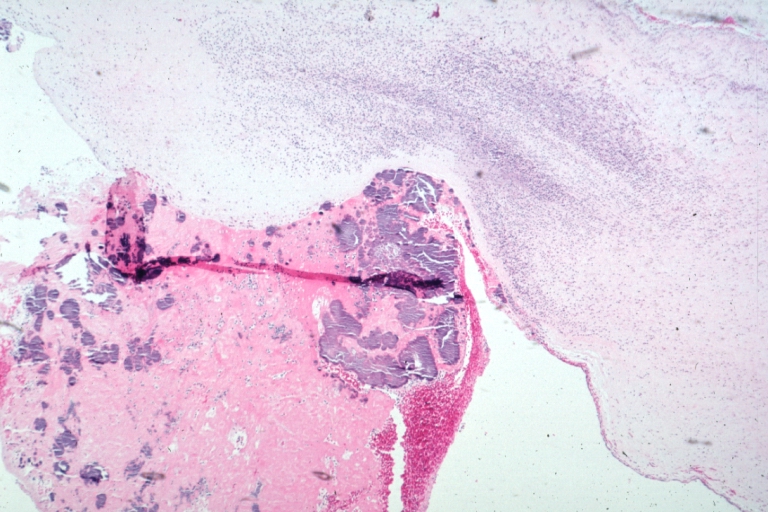
Thrombotic Nonbacterial Endocarditis Infected: Micro low mag H&E fibrin vegetation with masses of staphylococci and inflammatory cells in valve secondarily infected case 8 year survival breast papillary intraductal adenocarcinoma with extensive metastases gross is aortic valve lesions.


References
- ↑ Infective endocarditis. Wikipedia (2015). URL=https://en.wikipedia.org/wiki/Infective_endocarditis#Pathogenesis Accessed on September 21, 2015
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 Endocarditis. Wikipedia (2015). URL= https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015
- ↑ Infective Endocarditis. Libre Pathology (2015). URL=http://librepathology.org/wiki/index.php/Infective_endocarditis Accessed on September 21, 2015