Ebstein's anomaly of the tricuspid valve
| Ebstein's anomaly of the tricuspid valve | |
 | |
|---|---|
| Chest X-ray of a patient with Ebstein's anomaly (Image courtesy of RadsWiki) |
| Cardiology Network |
 Discuss Ebstein's anomaly of the tricuspid valve further in the WikiDoc Cardiology Network |
| Adult Congenital |
|---|
| Biomarkers |
| Cardiac Rehabilitation |
| Congestive Heart Failure |
| CT Angiography |
| Echocardiography |
| Electrophysiology |
| Cardiology General |
| Genetics |
| Health Economics |
| Hypertension |
| Interventional Cardiology |
| MRI |
| Nuclear Cardiology |
| Peripheral Arterial Disease |
| Prevention |
| Public Policy |
| Pulmonary Embolism |
| Stable Angina |
| Valvular Heart Disease |
| Vascular Medicine |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] and Claudia P. Hochberg, M.D. [2]
Please Join in Editing This Page and Apply to be an Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
Ebstein's anomaly is a congenital heart defect in which the opening of the tricuspid valve is displaced towards the apex of the right ventricle of the heart (congenital apical displacement of the tricuspid valve that typically causes significant tricuspid regurgitation).
The annulus of the valve is in normal position. The valve leaflets however, are to a varying degree attached to the walls and septum of the right ventricle. There is subsequent atrialization of a portion of the morphologic right ventricle (which is then contiguous with the right atrium). This causes the right atrium to be large and the anatomic right ventricle to be small in size. 50% of cases involve an atrial shunt (either a PFO or an ASD).
History
Ebstein's anomaly was named after Wilhelm Ebstein.
Associated Abnormalities
While Ebstein's anomaly is defined as the congenital displacement of the tricuspid valve towards the apex of the right ventricle, it is often associated with other abnormalities.
Anatomy
Typically, there are anatomic abnormalities of the tricuspid valve, with enlargement of the anterosuperior leaflet of the valve which is often adherent to the right ventricular free wall.
About 50% of individuals with Ebstein's anomaly have an associated shunt between the right and left atriums, either an atrial septal defect ASD or a patent foramen ovale PFO.
- The tricuspid valve leaflets are displaced toward the RV apex.
- The RV cavity is dilated and the free wall is thin.
- May be associated with LV dysfunction and mitral valve prolapse (MVP).
- It has also been associated with pulmonic stenosis (PS), VSD, pulmonary hypertension, bicuspid aortic valve and right sided aortic arch.
-It is commonly associated with congenitally corrected transposition of the great vessels and occasionally with tetralogy of Fallot.
- Is often associated with one or more accessory conduction pathways in 25%, and WPW in 13%. Usually this is a right sided accessory pathway.
- The presence of an ASD permits right-to-left shunting and cyanosis. The degree of cyanosis is related to the degree of tricuspid regurgitation (TR), tricuspid stenosis (TS) and the compliance of the RV.
-
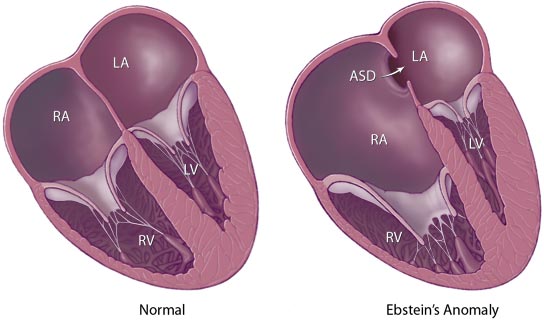
Graphical represntation of Ebstein's Anomaly from the Mayo Clinic website (note there is also an ASD on this diagram)

Epidemiology and Demographics
- Is a rare congenital heart disease.
- About 1:1,000 patients with congenital heart disease, or 1:210,000 live births.
- Males = females.
- Higher incidence in infants whose mothers are treated with Lithium Carbonate during pregnancy
Genetics
- Multifactorial inheritance, risk if a sibling has the disease is 1%.
Diagnosis
History
- Presentation depends greatly on the degree of apical displacement of the tricuspid valve leaflet as well as the degree of dysfunction of the tricuspid valve. If the tricuspid valve is severely deformed, fetal hydrops may occur. If the valve is functioning, patients may remain symptom free for many years.
- Palpitations may occur secondary to SVTs (supraventricular tachycardia) and WPW (Wolff-Parkinson-White syndrome) (8%).
- Growth and development are normal.
Physical Examination
General Appearance
Patients may have a bluish coloration of their face depending on the degree of cyanosis and right to left shunting.
Heart
Because the RA is dilated and compliant, there are no large v waves even in the presence of TR (tricuspid regurgitation) and the jugular venous pressure is often normal on exam. The chest may be asymmetric due to an enlarged right heart.
The first heart sound is widely split. There is a wide split S2 as a result of RBBB and delayed closure of the pulmonic valve. TR (tricuspid regurgitation), produces a holosystolic murmur which is heard best along the left lower sternal border and increases with inspiration.
Laboratory Findings
Electrocardiogram
The EKG is abnormal in 50 to 67%.
About 50% of individuals with Ebstein's anomaly have evidence of Wolff-Parkinson-White Syndrome (syndrome of pre-excitation of the ventricles due to an accessory pathway known as the Bundle of Kent), secondary to the the apical displacement of the septal tricuspid valve leaflet resulting in discontinuity of the central fibrous body.
The EKG can also shows prolonged AV condunction, tall peaked p waves consistent with right atrial enlargement, RBBB (Right Bundle Branch Block), a short PR interval and a delta wave and low voltages.
Chest X Ray
The Chest X-ray shows a balloon shaped heart that looks a lot like a pericardial effusion. The RA is dilated. The heart looks globular.
Echocardiogram
See Echo in Ebstein's anomaly of the tricuspid valve for more info/images
a) Can be used to assess the severity of dilatation of the right atrium, and the functional status of the tricuspid valve as well as the right ventricle.
b) Normally the tricuspid valve closes within 30 msec of the mitral valve. In Ebstein's, the tricuspid valve closes 50 to 60 msec after the mitral valve.
c) The delayed tricuspid closure is not due to RBBB because it also occurs with preexcitation.
d) 2D ECHO allows you to assess whether the repair can be accomplished without a prosthetic valve, and detects whether an interatrial shunt is present.
Image:Ebstein4.jpg|left|400px|thumb|]]
Below is an apical 4-chamber transthoracic view, showing apically-displaced leaflets of the tricuspid valve. Note substantial tricuspid regurgitation, which originates close to the apex, where the abnormal leaflets actually coapt:
<Youtube v=KEko3kM26bY/>
CT and MRI
Inferior displacement of tricuspid valve leaflets with enlargement of the right atrium and enlargement and dysfunction of the right ventricle.
Cardiac catheterization and hemodynamics
a) RA pressure usually not increased due to the fact that the RA is enlarged and compliant.
b) Normal RV pressures unless significant TR is present.
c) PA pressures are normal or slightly decreased due to TR and a large right-to-left shunt.
d) An ASD may be present
Treatment
Mechanical and Device Based Therapy
The protracted natural history of this disease in contrast to the uncertainty of long-term results of surgical intervention supports the policy of postponing surgical intervention until the onset of disability.
Adverse prognostic factors are
a) NYHA Class III or IV
b) Moderate to severe cardiomegaly
c) Cyanosis or an O2 sat < 90%
d) Disability during infancy
e)Paradoxical emboli
Surgery may include
- Tricuspid valve repair or replacement (when possible repair is preferable to replacement as it is associated with a lower mortality rate and fewer complications).
- Atrial septal defect repair.
- Right atrial plication (unclear whther this improves right ventricular function).
- Cardiac defibrillator implantation.
- Accessory pathways may require surgical intervention or ablation.
Hospital mortality at the Mayo for valve reconstruction is 6.7%. Only 1.6% in the Mayo series required reoperation. Long term follow up in the Mayo series showed 92% to have Class I or II symptoms and a 10 year mortality rate of 8%.
Generally, surgical treatment improves the exercise intolerance from NYHA-FC III or IV to NYHA-FC I or II.
Regardless of severity of the Ebstein’s Anomaly and type of treatment, risk of sudden death remains an important issue in patients with Ebstein's anomaly.
References
- Emma C. Ferguson, Rajesh Krishnamurthy, and Sandra A. A. Oldham. Classic Imaging Signs of Congenital Cardiovascular Abnormalities. RadioGraphics 2007 27: 1323-1334.
- Joris P. A. Beerepoot, and Pamela K. Woodard. Case 71: Ebstein Anomaly. Radiology 2004 231: 747-751.
External Links
Acknowledgements and Initial Contributors to Page
Leida Perez, M.D.