Chickenpox physical examination: Difference between revisions
No edit summary |
No edit summary |
||
| Line 1: | Line 1: | ||
__NOTOC__ | |||
{{CMG}} | {{CMG}} | ||
{{MJM}} | {{MJM}} | ||
| Line 15: | Line 16: | ||
===Appearance of the Patient=== | ===Appearance of the Patient=== | ||
====Chickenpox in | ====Chickenpox in Unvaccinated People==== | ||
The rash is generalized and [[pruritic]] (itchy). It progresses rapidly from [[macules]] to [[papules]] to [[vesicular lesions]] before crusting. The rash usually appears first on the [[head]], [[chest]], and [[back]] then spreads to the rest of the [[body]]. The lesions are usually most concentrated on the chest and back. | The rash is generalized and [[pruritic]] (itchy). It progresses rapidly from [[macules]] to [[papules]] to [[vesicular lesions]] before crusting. The rash usually appears first on the [[head]], [[chest]], and [[back]] then spreads to the rest of the [[body]]. The lesions are usually most concentrated on the chest and back. | ||
| Line 21: | Line 22: | ||
In healthy children, varicella is generally mild, with an itchy rash, malaise, and temperature up to 102°F for 2 to 3 days. Adults are at risk for more severe [[disease]] and have a higher incidence of complications. Recovery from primary varicella infection usually provides [[immunity]] for life. In otherwise healthy people, a second occurrence of varicella is uncommon and usually occurs in people who are [[immunocompromised]]. As with other [[viral]] infections, re-exposure to natural (wild-type) varicella may lead to re-infection that boosts [[antibody]]] [[titers]] without causing illness or detectable [[viremia]]. | In healthy children, varicella is generally mild, with an itchy rash, malaise, and temperature up to 102°F for 2 to 3 days. Adults are at risk for more severe [[disease]] and have a higher incidence of complications. Recovery from primary varicella infection usually provides [[immunity]] for life. In otherwise healthy people, a second occurrence of varicella is uncommon and usually occurs in people who are [[immunocompromised]]. As with other [[viral]] infections, re-exposure to natural (wild-type) varicella may lead to re-infection that boosts [[antibody]]] [[titers]] without causing illness or detectable [[viremia]]. | ||
====Chickenpox in | ====Chickenpox in Vaccinated People==== | ||
Chickenpox in people who are vaccinated is referred to as breakthrough varicella. | Chickenpox in people who are vaccinated is referred to as breakthrough varicella. | ||
Breakthrough varicella is [[infection]] with wild-type VZV occurring in a vaccinated person more than 42 days after varicella vaccination. Breakthrough varicella is usually mild. Patients typically are [[afebrile]] or have low fever and develop fewer than 50 [[skin]] lesions. They usually have a shorter illness compared to unvaccinated people who get varicella. The rash is more likely to be predominantly maculopapular rather than vesicular. However, 25%-30% of persons vaccinated with 1 dose with breakthrough varicella have clinical features typical of varicella in unvaccinated people. | Breakthrough varicella is [[infection]] with wild-type VZV occurring in a vaccinated person more than 42 days after varicella vaccination. Breakthrough varicella is usually mild. Patients typically are [[afebrile]] or have low fever and develop fewer than 50 [[skin]] lesions. They usually have a shorter illness compared to unvaccinated people who get varicella. The rash is more likely to be predominantly maculopapular rather than vesicular. However, 25%-30% of persons vaccinated with 1 dose with breakthrough varicella have clinical features typical of varicella in unvaccinated people. | ||
| Line 27: | Line 28: | ||
Since the clinical features of breakthrough varicella are often mild, it can be difficult to make a diagnosis on clinical presentation alone. Laboratory testing is increasingly important for confirming varicella and appropriately managing cases and their contacts. There is limited information about breakthrough varicella in persons who have received two doses of varicella vaccine, though it appears to occur less frequently among people vaccinated with two doses of varicella vaccine compared to persons who have received a single dose of varicella vaccine. | Since the clinical features of breakthrough varicella are often mild, it can be difficult to make a diagnosis on clinical presentation alone. Laboratory testing is increasingly important for confirming varicella and appropriately managing cases and their contacts. There is limited information about breakthrough varicella in persons who have received two doses of varicella vaccine, though it appears to occur less frequently among people vaccinated with two doses of varicella vaccine compared to persons who have received a single dose of varicella vaccine. | ||
====Unvaccinated | ====Unvaccinated Individuals==== | ||
<gallery> | <gallery> | ||
Image:Chickenpox U1.jpg|Girl with a secondary skin infection due to chickenpox. | Image:Chickenpox U1.jpg|Girl with a secondary skin infection due to chickenpox. | ||
| Line 35: | Line 36: | ||
</gallery> | </gallery> | ||
====Vaccinated | ====Vaccinated Individuals==== | ||
<gallery> | <gallery> | ||
Image:Chickenpox V1.jpg|Image of Breakthrough Chickenpox: Back of child with breakthrough varicella. | Image:Chickenpox V1.jpg|Image of Breakthrough Chickenpox: Back of child with breakthrough varicella. | ||
| Line 46: | Line 47: | ||
==References== | ==References== | ||
{{Reflist|2}} | {{Reflist|2}} | ||
[[Category:Viral diseases]] | |||
[[Category:Pediatrics]] | |||
[[Category:Poxviruses]] | |||
[[Category:Infectious disease]] | |||
[[Category:Overview complete]] | |||
[[Category:primary care]] | |||
{{WikiDoc Help Menu}} | |||
{{WikiDoc Sources}} | |||
Revision as of 20:46, 22 February 2013
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Michael Maddaleni, B.S.
|
Chickenpox Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Chickenpox physical examination On the Web |
|
American Roentgen Ray Society Images of Chickenpox physical examination |
|
Risk calculators and risk factors for Chickenpox physical examination |
Overview
The diagnosis of varicella is primarily clinical. In a non-immunized individual with typical prodromal symptoms associated with the appropriate appearing rash occurring in "crops", no further investigation would normally be undertaken.
If further investigation is undertaken, confirmation of the diagnosis can be sought through either examination of the fluid within the vesicles, or by testing blood for evidence of an acute immunologic reposnse. Vesicle fluid can be examined with a Tsanck smear, or better with examination for direct fluorescent antibody. The fluid can also be "cultured", whereby attempts are made to grow the virus from a fluid sample. Blood tests can be used to identify a response to acute infection (IgM) or previous infection and subsequent immunity (IgE).[1]
Prenatal diagnosis of foetal varicella infection can be performed using ultrasound, though a delay of 5 weeks following primary maternal infection is advised. A PCR (DNA) test of the mother's amniotic fluid can also be performed, though the risk of spontaneous abortion due to the amniocentesis procedure is higher than the risk of the baby developing foetal varicella syndrome.
Physical Examination
Appearance of the Patient
Chickenpox in Unvaccinated People
The rash is generalized and pruritic (itchy). It progresses rapidly from macules to papules to vesicular lesions before crusting. The rash usually appears first on the head, chest, and back then spreads to the rest of the body. The lesions are usually most concentrated on the chest and back.
In healthy children, varicella is generally mild, with an itchy rash, malaise, and temperature up to 102°F for 2 to 3 days. Adults are at risk for more severe disease and have a higher incidence of complications. Recovery from primary varicella infection usually provides immunity for life. In otherwise healthy people, a second occurrence of varicella is uncommon and usually occurs in people who are immunocompromised. As with other viral infections, re-exposure to natural (wild-type) varicella may lead to re-infection that boosts antibody] titers without causing illness or detectable viremia.
Chickenpox in Vaccinated People
Chickenpox in people who are vaccinated is referred to as breakthrough varicella. Breakthrough varicella is infection with wild-type VZV occurring in a vaccinated person more than 42 days after varicella vaccination. Breakthrough varicella is usually mild. Patients typically are afebrile or have low fever and develop fewer than 50 skin lesions. They usually have a shorter illness compared to unvaccinated people who get varicella. The rash is more likely to be predominantly maculopapular rather than vesicular. However, 25%-30% of persons vaccinated with 1 dose with breakthrough varicella have clinical features typical of varicella in unvaccinated people.
Since the clinical features of breakthrough varicella are often mild, it can be difficult to make a diagnosis on clinical presentation alone. Laboratory testing is increasingly important for confirming varicella and appropriately managing cases and their contacts. There is limited information about breakthrough varicella in persons who have received two doses of varicella vaccine, though it appears to occur less frequently among people vaccinated with two doses of varicella vaccine compared to persons who have received a single dose of varicella vaccine.
Unvaccinated Individuals
-
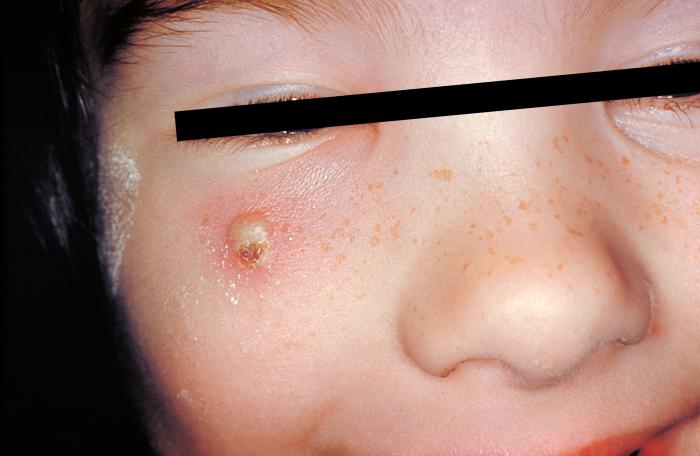
Girl with a secondary skin infection due to chickenpox.
-

Chickenpox in an unvaccinated child.
-

Chickenpox in an unvaccinated adult.
-

Chickenpox in unvaccinated adult.




Vaccinated Individuals
-

Image of Breakthrough Chickenpox: Back of child with breakthrough varicella.
-

Image of Breakthrough Chickenpox: Back of child with breakthrough varicella.
-

The skin lesions of breakthrough varicella can be macular rather than vesicular. They are rarely bullous or hemorrhagic, and residual scarring is less common.
-

Breakthrough varicella on the abdomen of a vaccinated child.
-

Breakthrough varicella on the back of a vaccinated child.





References
- ↑ McPherson & Pincus: Henry's Clinical Diagnosis and Management by Laboratory Methods, 21st ed., 2007, Chapter 54.