Quetiapine
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
Disclaimer
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Black Box Warning
|
INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS; and SUICIDAL THOUGHTS AND BEHAVIORS
See full prescribing information for complete Boxed Warning.
|
Overview
Quetiapine is a that is FDA approved for the {{{indicationType}}} of schizophrenia, bipolar I disorder, manic or mixed episodes, bipolar disorder, depressive episodes, major depressive disorder, adjunctive therapy with antidepressants. There is a Black Box Warning for this drug as shown here. Common adverse reactions include somnolence, dry mouth, constipation, dizziness, increased appetite, dyspepsia, weight gain, fatigue, dysarthria, and nasal congestion in the adults. somnolence, dizziness, fatigue, increased appetite, nausea, vomiting, dry mouth, tachycardia, weight increase in children and adolescents.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
- Important Administration Instructions
- SEROQUEL XR tablets should be swallowed whole and not split, chewed or crushed.
- It is recommended that SEROQUEL XR be taken without food or with a light meal (approximately 300 calories).
- SEROQUEL XR should be administered once daily, preferably in the evening.
- Recommended Dosing
- The recommended initial dose, titration, dose range and maximum SEROQUEL XR dose for each approved indication is displayed in Table 1 below. After initial dosing, adjustments can be made upwards or downwards, if necessary, depending upon the clinical response and tolerability of the patient
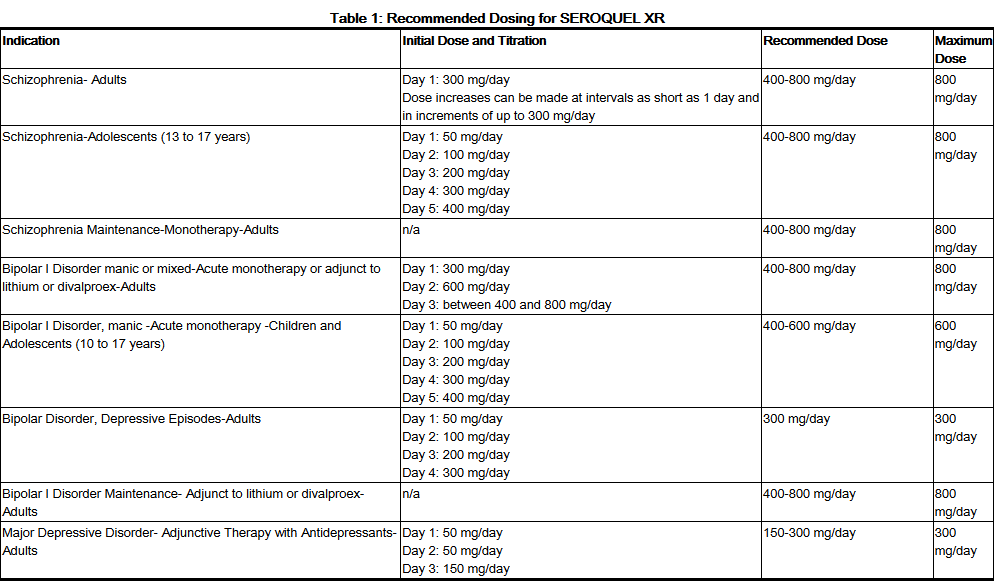
This image is provided by the National Library of Medicine.

- Maintenance Treatment for Schizophrenia and Bipolar I Disorder
- Maintenance Treatment
- Patients should be periodically reassessed to determine the need for maintenance treatment and the appropriate dose for such treatment.
- Maintenance Treatment
- Dose Modifications in Elderly Patients
- Consideration should be given to a slower rate of dose titration and a lower target dose in the elderly and in patients who are debilitated or who have a predisposition to hypotensive reactions [see Use in Specific Populations (8.5, 8.7) and Clinical Pharmacology (12)]. When indicated, dose escalation should be performed with caution in these patients.
- Elderly patients should be started on SEROQUEL XR 50 mg/day and the dose can be increased in increments of 50 mg/day depending on the clinical response and tolerability of the individual patient.
- Dose Modifications in Hepatically Impaired Patients
- Patients with hepatic impairment should be started on SEROQUEL XR 50 mg/day. The dose can be increased daily in increments of 50 mg/day to an effective dose, depending on the clinical response and tolerability of the patient.
- Dose Modifications when used with CYP3A4 Inhibitors
- SEROQUEL XR dose should be reduced to one sixth of original dose when co-medicated with a potent CYP3A4 inhibitor (e.g., ketoconazole, itraconazole, indinavir, ritonavir, nefazodone, etc.). When the CYP3A4 inhibitor is discontinued, the dose of SEROQUEL XR should be increased by 6 fold.
- Dose Modifications when used with CYP3A4 Inducers
- SEROQUEL XR dose should be increased up to 5 fold of the original dose when used in combination with a chronic treatment (e.g., greater than 7-14 days) of a potent CYP3A4 inducer (e.g., phenytoin, carbamazepine, rifampin, avasimibe, St. John’s wort etc.). The dose should be titrated based on the clinical response and tolerance of the individual patient. When the CYP3A4 inducer is discontinued, the dose of SEROQUEL XR should be reduced to the original level within 7-14 days [see Clinical Pharmacology (12.3) and Drug Interactions (7.1)].
- Reinitiation of Treatment in Patients Previously Discontinued
- Although there are no data to specifically address re-initiation of treatment, it is recommended that when restarting therapy of patients who have been off SEROQUEL XR for more than one week, the initial dosing schedule should be followed. When restarting patients who have been off SEROQUEL XR for less than one week, gradual dose escalation may not be required and the maintenance dose may be reinitiated.
- Switching Patients from SEROQUEL Tablets to SEROQUEL XR Tablets
- Patients who are currently being treated with SEROQUEL (immediate release formulation) may be switched to SEROQUEL XR at the equivalent total daily dose taken once daily. Individual dosage adjustments may be necessary.
- Switching from Antipsychotics
- There are no systematically collected data to specifically address switching patients from other antipsychotics to SEROQUEL XR, or concerning concomitant administration with other antipsychotics. While immediate discontinuation of the previous antipsychotic treatment may be acceptable for some patients, more gradual discontinuation may be most appropriate for others. In all cases, the period of overlapping antipsychotic administration should be minimized. When switching patients from depot antipsychotics, if medically appropriate, initiate SEROQUEL XR therapy in place of the next scheduled injection. The need for continuing existing extrapyramidal syndrome medication should be re-evaluated periodically.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
Condition1
- Developed by:
- Class of Recommendation:
- Strength of Evidence:
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Quetiapine in adult patients.
Non–Guideline-Supported Use
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Quetiapine in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding FDA-Labeled Use of Quetiapine in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
Condition1
- Developed by:
- Class of Recommendation:
- Strength of Evidence:
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Guideline-Supported Use of Quetiapine in pediatric patients.
Non–Guideline-Supported Use
Condition1
- Dosing Information
- Dosage
Condition2
There is limited information regarding Off-Label Non–Guideline-Supported Use of Quetiapine in pediatric patients.
Contraindications
- Hypersensitivity to quetiapine or to any excipients in the SEROQUEL XR formulation. Anaphylactic reactions have been reported in patients treated with SEROQUEL XR.
Warnings
|
INCREASED MORTALITY IN ELDERLY PATIENTS WITH DEMENTIA-RELATED PSYCHOSIS; and SUICIDAL THOUGHTS AND BEHAVIORS
See full prescribing information for complete Boxed Warning.
|
Precautions
Increased Mortality in Elderly Patients with Dementia-Related Psychosis
- Elderly patients with dementia-related psychosis treated with antipsychotic drugs are at an increased risk of death. Analysis of 17 placebo-controlled trials (modal duration of 10 weeks), largely in patients taking atypical antipsychotic drugs, revealed a risk of death in drug-treated patients of between 1.6 to 1.7 times the risk of death in placebo-treated patients. Over the course of a typical 10-week controlled trial, the rate of death in drug-treated patients was about 4.5%, compared to a rate of about 2.6% in the placebo group. Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. SEROQUEL XR is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning].
Suicidal Thoughts and Behaviors in Adolescents and Young Adults
- Patients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment. Pooled analyses of short-term placebo-controlled trials of antidepressant drugs (SSRIs and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18-24) with major depressive disorder (MDD) and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a reduction with antidepressants compared to placebo in adults aged 65 and older.
- The pooled analyses of placebo-controlled trials in children and adolescents with MDD, obsessive compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term trials of 9 antidepressant drugs in over 4400 patients. The pooled analyses of placebo-controlled trials in adults with MDD or other psychiatric disorders included a total of 295 short-term trials (median duration of 2 months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk differences (drug vs. placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 2.
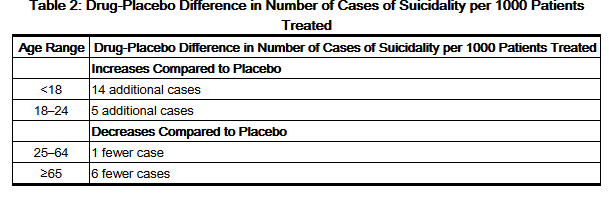
This image is provided by the National Library of Medicine.

- No suicides occurred in any of the pediatric trials. There were suicides in the adult trials, but the number was not sufficient to reach any conclusion about drug effect on suicide.
- It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, there is substantial evidence from placebo-controlled maintenance trials in adults with depression that the use of antidepressants can delay the recurrence of depression.
- All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases.
- The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with antidepressants for major depressive disorder as well as for other indications, both psychiatric and nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.
- Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset, or were not part of the patient's presenting symptoms.
- Families and caregivers of patients being treated with antidepressants for major depressive disorder or other indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to healthcare providers. Such monitoring should include daily observation by families and caregivers. Prescriptions for SEROQUEL XR should be written for the smallest quantity of tablets consistent with good patient management, in order to reduce the risk of overdose.
Screening Patients for Bipolar Disorder
- A major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled trials) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, including SEROQUEL XR, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression.
Cerebrovascular Adverse Reactions, Including Stroke, in Elderly Patients with Dementia-Related Psychosis
- In placebo-controlled trials with risperidone, aripiprazole, and olanzapine in elderly subjects with dementia, there was a higher incidence of cerebrovascular adverse reactions (cerebrovascular accidents and transient ischemic attacks), including fatalities, compared to placebo-treated subjects. SEROQUEL XR is not approved for the treatment of patients with dementia-related psychosis [see Boxed Warning and Warnings and Precautions (5.1)].
Neuroleptic Malignant Syndrome (NMS)
- A potentially fatal symptom complex sometimes referred to as Neuroleptic Malignant Syndrome (NMS) has been reported in association with administration of antipsychotic drugs, including quetiapine. Rare cases of NMS have been reported with quetiapine. Clinical manifestations of NMS are hyperpyrexia, muscle rigidity, altered mental status, and evidence of autonomic instability (irregular pulse or blood pressure, tachycardia, diaphoresis, and cardiac dysrhythmia). Additional signs may include elevated creatine phosphokinase, myoglobinuria (rhabdomyolysis) and acute renal failure.
- The diagnostic evaluation of patients with this syndrome is complicated. In arriving at a diagnosis, it is important to exclude cases where the clinical presentation includes both serious medical illness (e.g., pneumonia, systemic infection, etc.) and untreated or inadequately treated extrapyramidal signs and symptoms (EPS). Other important considerations in the differential diagnosis include central anticholinergic toxicity, heat stroke, drug fever and primary central nervous system (CNS) pathology.
- The management of NMS should include: 1) immediate discontinuation of antipsychotic drugs and other drugs not essential to concurrent therapy; 2) intensive symptomatic treatment and medical monitoring; and 3) treatment of any concomitant serious medical problems for which specific treatments are available. There is no general agreement about specific pharmacological treatment regimens for NMS.
- If a patient requires antipsychotic drug treatment after recovery from NMS, the potential reintroduction of drug therapy should be carefully considered. The patient should be carefully monitored since recurrences of NMS have been reported.
Metabolic Changes
- Atypical antipsychotic drugs have been associated with metabolic changes that include hyperglycemia/diabetes mellitus, dyslipidemia, and body weight gain. While all of the drugs in the class have been shown to produce some metabolic changes, each drug has its own specific risk profile. In some patients, a worsening of more than one of the metabolic parameters of weight, blood glucose, and lipids was observed in clinical studies. Changes in these metabolic profiles should be managed as clinically appropriate.
Hyperglycemia and Diabetes Mellitus
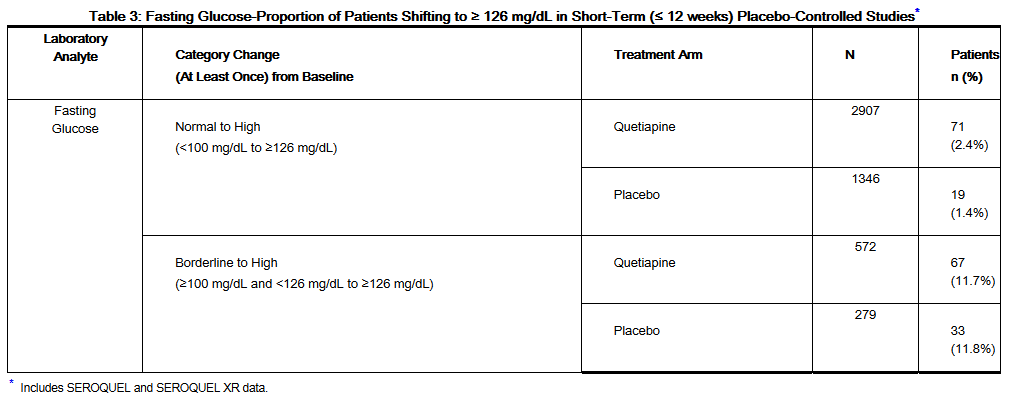
- Hyperglycemia, in some cases extreme and associated with ketoacidosis or hyperosmolar coma or death, has been reported in patients treated with atypical antipsychotics, including quetiapine. Assessment of the relationship between atypical antipsychotic use and glucose abnormalities is complicated by the possibility of an increased background risk of diabetes mellitus in patients with schizophrenia and the increasing incidence of diabetes mellitus in the general population. Given these confounders, the relationship between atypical antipsychotic use and hyperglycemia-related adverse reactions is not completely understood. However, epidemiological studies suggest an increased risk of treatment-emergent hyperglycemia-related adverse reactions in patients treated with the atypical antipsychotics. Precise risk estimates for hyperglycemia-related adverse reactions in patients treated with atypical antipsychotics are not available.
- Patients with an established diagnosis of diabetes mellitus who are started on atypical antipsychotics should be monitored regularly for worsening of glucose control. Patients with risk factors for diabetes mellitus (e.g., obesity, family history of diabetes) who are starting treatment with atypical antipsychotics should undergo fasting blood glucose testing at the beginning of treatment and periodically during treatment. Any patient treated with atypical antipsychotics should be monitored for symptoms of hyperglycemia including polydipsia, polyuria, polyphagia, and weakness. Patients who develop symptoms of hyperglycemia during treatment with atypical antipsychotics should undergo fasting blood glucose testing. In some cases, hyperglycemia has resolved when the atypical antipsychotic was discontinued; however, some patients required continuation of anti-diabetic treatment despite discontinuation of the suspect drug.
- Adults:
This image is provided by the National Library of Medicine.

- In a 24-week trial (active-controlled, 115 patients treated with SEROQUEL) designed to evaluate glycemic status with oral glucose tolerance testing of all patients, at week 24 the incidence of a treatment-emergent post-glucose challenge glucose level ≥ 200 mg/dL was 1.7% and the incidence of a fasting treatment-emergent blood glucose level ≥ 126 mg/dL was 2.6%. The mean change in fasting glucose from baseline was 3.2 mg/dL and mean change in 2 hour glucose from baseline was -1.8 mg/dL for quetiapine.
- In 2 long-term placebo-controlled randomized withdrawal clinical trials for bipolar I disorder maintenance, mean exposure of 213 days for SEROQUEL (646 patients) and 152 days for placebo (680 patients), the mean change in glucose from baseline was +5.0 mg/dL for quetiapine and –0.05 mg/dL for placebo. The exposure-adjusted rate of any increased blood glucose level (≥ 126 mg/dL) for patients more than 8 hours since a meal (however, some patients may not have been precluded from calorie intake from fluids during fasting period) was 18.0 per 100 patient years for SEROQUEL (10.7% of patients; n=556) and 9.5 for placebo per 100 patient years (4.6% of patients; n=581).
- Table 4 shows the percentage of patients with shifts in blood glucose to ≥ 126 mg/dL from normal baseline in MDD adjunct therapy trials by dose.
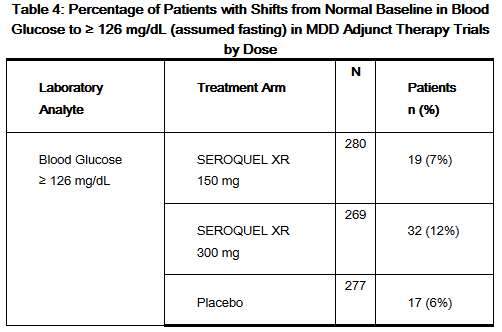
This image is provided by the National Library of Medicine.

- Children and Adolescents: Safety and effectiveness of SEROQUEL XR is supported from studies of SEROQUEL in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.2)]. In a placebo-controlled SEROQUEL XR monotherapy study (8 weeks duration) of children and adolescent patients (10 – 17 years of age) with bipolar depression, in which efficacy was not established, the mean change in fasting glucose levels for SEROQUEL XR (n = 60) compared to placebo (n = 62) was 1.8 mg/dL versus 1.6 mg/dL. In this study, there were no patients in the SEROQUEL XR or placebo-treated groups with a baseline normal fasting glucose level (< 100 mg/dL) that had an increase in blood glucose level ≥ 126 mg/dL. There was one patient in the SEROQUEL XR group with a baseline borderline fasting glucose level (≥ 100 mg/dL) and < 126 mg/dL) who had an increase in blood glucose level of > 126 mg/dL compared to zero patients in the placebo group.
- In a placebo-controlled SEROQUEL monotherapy study of adolescent patients (13–17 years of age) with schizophrenia (6 weeks duration), the mean change in fasting glucose levels for SEROQUEL (n=138) compared to placebo (n=67) was –0.75 mg/dL versus –1.70 mg/dL. In a placebo-controlled SEROQUEL monotherapy study of children and adolescent patients (10–17 years of age) with bipolar mania (3 weeks duration), the mean change in fasting glucose level for SEROQUEL (n=170) compared to placebo (n=81) was 3.62 mg/dL versus –1.17 mg/dL. No patient in either study with a baseline normal fasting glucose level (<100 mg/dL) or a baseline borderline fasting glucose level (≥100 mg/dL and <126 mg/dL) had a treatment-emergent blood glucose level of ≥126 mg/dL.
- Dyslipidemia
- Adults:
- Table 5 shows the percentage of patients with changes in cholesterol and triglycerides from baseline by indication in clinical trials with SEROQUEL XR.
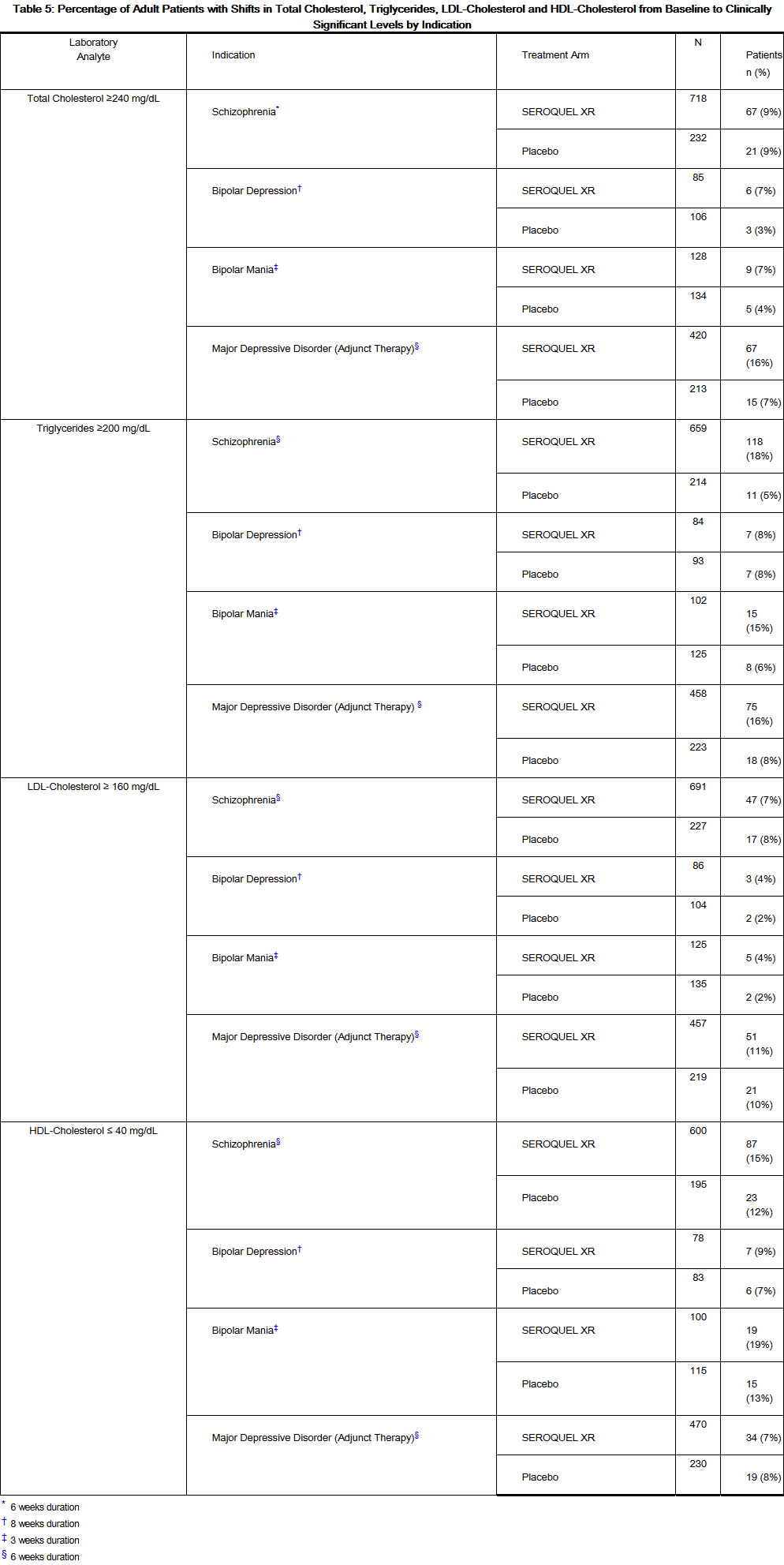
This image is provided by the National Library of Medicine.

- In SEROQUEL clinical trials for schizophrenia, the percentage of patients with shifts in cholesterol and triglycerides from baseline to clinically significant levels were 18% (placebo: 7%) and 22% (placebo: 16%). HDL-cholesterol and LDL-cholesterol parameters were not measured in these studies. In SEROQUEL clinical trials for bipolar depression, the following percentage of patients had shifts from baseline to clinically significant levels for the four lipid parameters measured: total cholesterol 9% (placebo: 6%); triglycerides 14% (placebo: 9%); LDL-cholesterol 6% (placebo: 5%) and HDL-cholesterol 14% (placebo: 14%). Lipid parameters were not measured in the bipolar mania studies.
- Table 6 shows the percentage of patients in MDD adjunctive therapy trials with clinically significant shifts in total-cholesterol, triglycerides, LDL-cholesterol and HDL-cholesterol from baseline by dose.
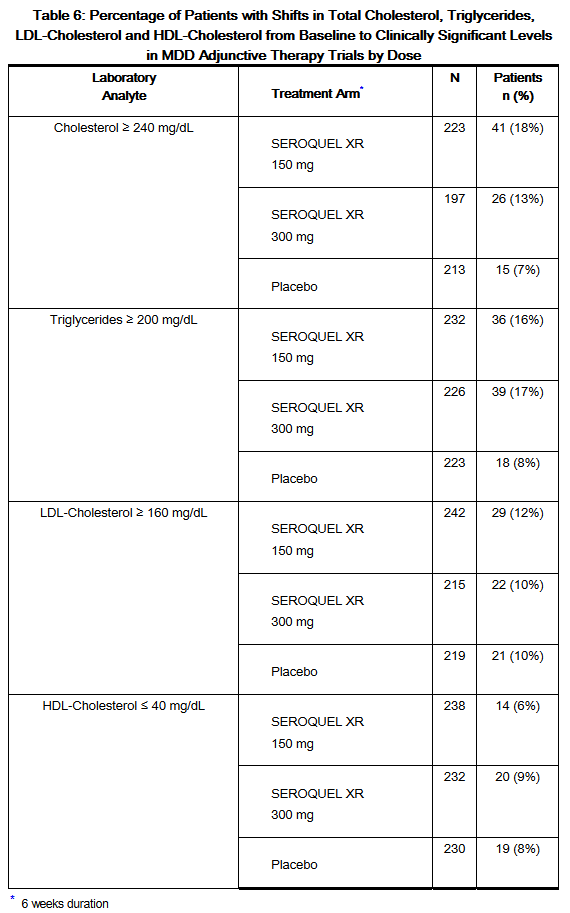
This image is provided by the National Library of Medicine.

- Children and Adolescents:
- Safety and effectiveness of SEROQUEL XR is supported by studies of SEROQUEL in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.1 and 14.2)].
- In a placebo-controlled SEROQUEL XR monotherapy study (8 weeks duration) of children and adolescent patients (10-17 years of age) with bipolar depression, in which efficacy was not established, the percentage of children and adolescents with shifts in total cholesterol (≥200 mg/dL), triglycerides (≥150 mg/dL), LDL-cholesterol (≥ 130 mg/dL) and HDL-cholesterol (≤40 mg/dL) from baseline to clinically significant levels were: total cholesterol 8% (7/83) for SEROQUEL XR vs. 6% (5/84) for placebo; triglycerides 28% (22/80) for SEROQUEL XR vs. 9% (7/82) for placebo; LDL-cholesterol 2% (2/86) for SEROQUEL XR vs. 4% (3/85) for placebo and HDL-cholesterol 20% (13/65) for SEROQUEL XR vs 15% (11/74) for placebo.
- Table 7 shows the percentage of children and adolescents with shifts in total cholesterol, triglycerides, LDL-cholesterol and HDL-cholesterol from baseline to clinically significant levels by indication in clinical trials with SEROQUEL in adolescents (13–17 years) with schizophrenia and in children and adolescents (10–17 years) with bipolar mania.
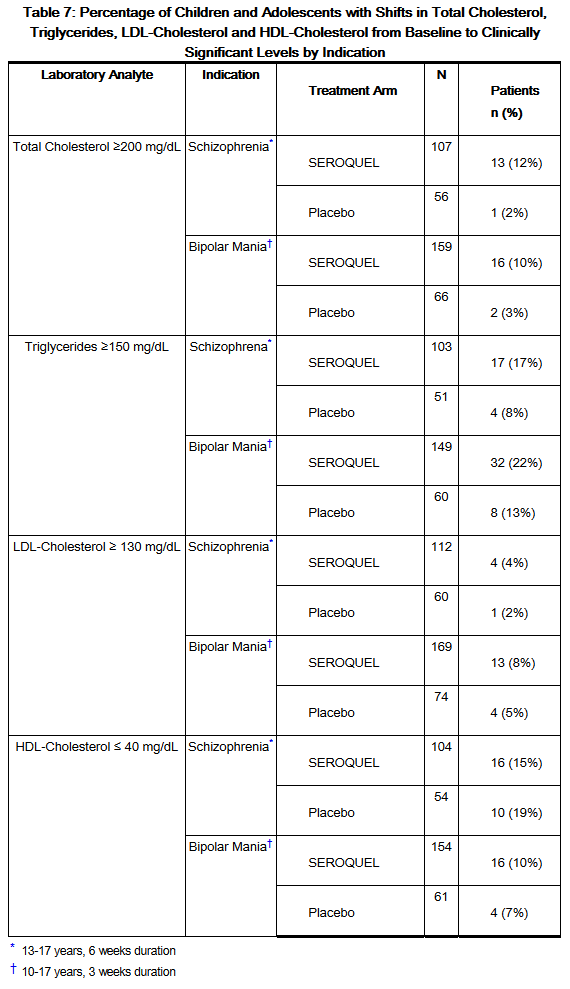
This image is provided by the National Library of Medicine.

- Weight Gain
- Increases in weight have been observed in clinical trials. Patients receiving quetiapine should receive regular monitoring of weight.
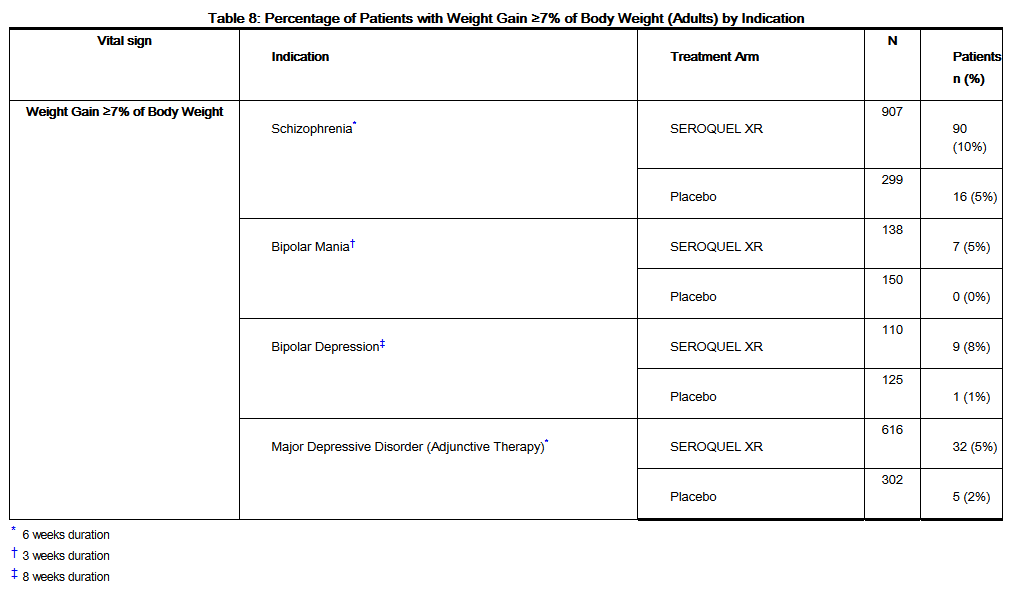
- Adults: Table 8 shows the percentage of adult patients with weight gain of ≥7% of body weight by indication.
This image is provided by the National Library of Medicine.

- In schizophrenia trials, the proportions of patients meeting a weight gain criterion of ≥7% of body weight were compared in a pool of four 3- to 6-week placebo-controlled clinical trials, revealing a statistically significant greater incidence of weight gain for SEROQUEL (23%) compared to placebo (6%).
- Table 9 shows the percentage of adult patients with weight gain of ≥7% of body weight for MDD by dose.
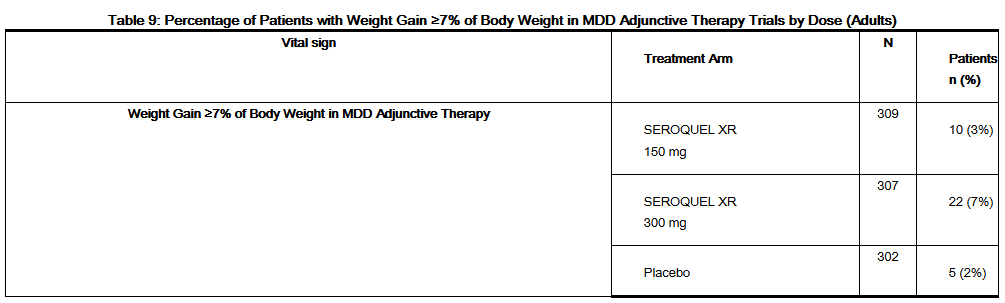
This image is provided by the National Library of Medicine.

- Children and Adolescents: Safety and effectiveness of SEROQUEL XR is supported by studies of SEROQUEL in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.1 and 14.2)]. In a clinical trial for SEROQUEL XR in children and adolescents (10-17 years of age) with bipolar depression, in which efficacy was not established, the percentage of patients with weight gain ≥7% of body weight at any time was 15% (14/92) for SEROQUEL XR vs. 10% (10/100) for placebo. The mean change in body weight was 1.4 kg in the SEROQUEL XR group vs. 0.6 kg in the placebo group.
- Weight gain was greater in patients 10-12 years of age compared to patients 13-17 years of age. The percentage of patients 10-12 years of age with weight gain ≥7% at any time was 28% (7/25) for SEROQUEL XR vs. 0% (0/28) for placebo. The percentage of patients 13-17 years of age with weight gain ≥7% at any time was 10.4% (7/67) for SEROQUEL XR vs. 13.9% (10/72) for placebo.
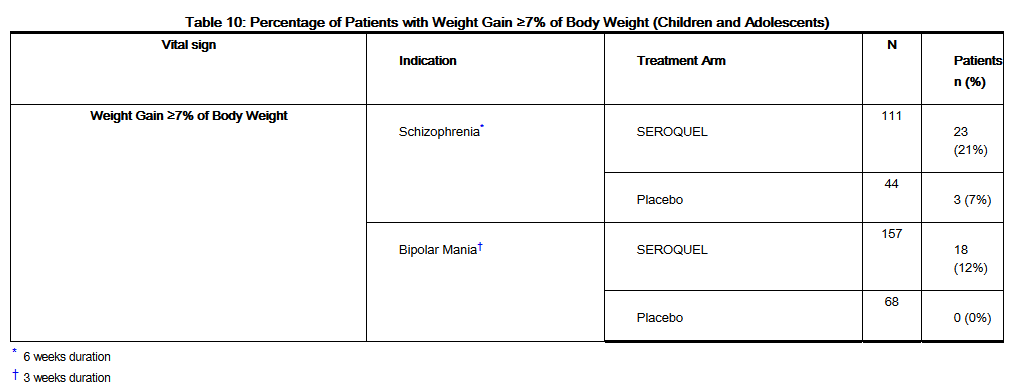
- Table 10 shows the percentage of children and adolescents with weight gain ≥7% of body weight in clinical trials with SEROQUEL in adolescents (13 – 17 years) with schizophrenia and in children and adolescents (10 – 17 years) with bipolar mania.
This image is provided by the National Library of Medicine.

- The mean change in body weight in the schizophrenia trial was 2.0 kg in the SEROQUEL group and -0.4 kg in the placebo group and in the bipolar mania trial it was 1.7 kg in the SEROQUEL group and 0.4 kg in the placebo group.
- In an open-label study that enrolled patients from the above two pediatric trials, 63% of patients (241/380) completed 26 weeks of therapy with SEROQUEL. After 26 weeks of treatment, the mean increase in body weight was 4.4 kg. Forty-five percent of the patients gained ≥ 7% of their body weight, not adjusted for normal growth. In order to adjust for normal growth over 26 weeks, an increase of at least 0.5 standard deviation from baseline in BMI was used as a measure of a clinically significant change; 18.3% of patients on SEROQUEL met this criterion after 26 weeks of treatment.
- When treating pediatric patients with SEROQUEL for any indication, weight gain should be assessed against that expected for normal growth.
Tardive Dyskinesia
- A syndrome of potentially irreversible, involuntary, dyskinetic movements may develop in patients treated with antipsychotic drugs including quetiapine. Although the prevalence of the syndrome appears to be highest among the elderly, especially elderly women, it is impossible to rely upon prevalence estimates to predict, at the inception of antipsychotic treatment, which patients are likely to develop the syndrome. Whether antipsychotic drug products differ in their potential to cause tardive dyskinesia is unknown.
- The risk of developing tardive dyskinesia and the likelihood that it will become irreversible are believed to increase as the duration of treatment and the total cumulative dose of antipsychotic drugs administered to the patient increase. However, the syndrome can develop, although much less commonly, after relatively brief treatment periods at low doses or may even arise after discontinuation of treatment.
- There is no known treatment for established cases of tardive dyskinesia, although the syndrome may remit, partially or completely, if antipsychotic treatment is withdrawn. Antipsychotic treatment, itself, however, may suppress (or partially suppress) the signs and symptoms of the syndrome and thereby may possibly mask the underlying process. The effect that symptomatic suppression has upon the long-term course of the syndrome is unknown.
- Given these considerations, SEROQUEL XR should be prescribed in a manner that is most likely to minimize the occurrence of tardive dyskinesia. Chronic antipsychotic treatment should generally be reserved for patients who appear to suffer from a chronic illness that (1) is known to respond to antipsychotic drugs, and (2) for whom alternative, equally effective, but potentially less harmful treatments are not available or appropriate. In patients who do require chronic treatment, the smallest dose and the shortest duration of treatment producing a satisfactory clinical response should be sought. The need for continued treatment should be reassessed periodically.
- If signs and symptoms of tardive dyskinesia appear in a patient on SEROQUEL XR, drug discontinuation should be considered. However, some patients may require treatment with quetiapine despite the presence of the syndrome.
Hypotension
- Quetiapine may induce orthostatic hypotension associated with dizziness, tachycardia and, in some patients, syncope, especially during the initial dose-titration period, probably reflecting its ά1-adrenergic antagonist properties. Syncope was reported in 0.3% (5/1866) of the patients treated with SEROQUEL XR across all indications, compared with 0.2% (2/928) on placebo. Syncope was reported in 1% (28/3265) of the patients treated with SEROQUEL, compared with 0.2% (2/954) on placebo. Orthostatic hypotension, dizziness, and syncope may lead to falls.
- Quetiapine should be used with particular caution in patients with known cardiovascular disease (history of myocardial infarction or ischemic heart disease, heart failure or conduction abnormalities), cerebrovascular disease or conditions which would predispose patients to hypotension (dehydration, hypovolemia and treatment with antihypertensive medications). If hypotension occurs during titration to the target dose, a return to the previous dose in the titration schedule is appropriate.
Increases in Blood Pressure (Children and Adolescents)
- Safety and effectiveness of SEROQUEL XR is supported by studies of SEROQUEL in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.1 and 14.2)].
- In a placebo-controlled SEROQUEL XR clinical trial (8 weeks duration) in children and adolescents (10-17 years of age) with bipolar depression, in which efficacy was not established, the incidence of increases at any time in systolic blood pressure (≥20 mmHg) was 6.5% (6/92) for SEROQUEL XR and 6.0% (6/100) for placebo; the incidence of increases at any time in diastolic blood pressure (≥10 mmHg) was 46.7% (43/92) for SEROQUEL XR and 36.0% (36/100) for placebo.
- In placebo-controlled trials in children and adolescents with schizophrenia (13-17 years old, 6-week duration) or bipolar mania (10-17 years old, 3-week duration), the incidence of increases at any time in systolic blood pressure (≥20 mmHg) was 15.2% (51/335) for SEROQUEL and 5.5% (9/163) for placebo; the incidence of increases at any time in diastolic blood pressure (≥10 mmHg) was 40.6% (136/335) for SEROQUEL and 24.5% (40/163) for placebo. In the 26-week open-label clinical trial, one child with a reported history of hypertension experienced a hypertensive crisis. Blood pressure in children and adolescents should be measured at the beginning of, and periodically during treatment.
Leukopenia, Neutropenia and Agranulocytosis
- In clinical trials and postmarketing experience, events of leukopenia/neutropenia have been reported temporally related to atypical antipsychotic agents, including quetiapine fumarate. Agranulocytosis (including fatal cases) has also been reported.
- Possible risk factors for leukopenia/neutropenia include pre-existing low white cell count (WBC) and history of drug induced leukopenia/neutropenia. Patients with a pre-existing low WBC or a history of drug induced leukopenia/neutropenia should have their complete blood count (CBC) monitored frequently during the first few months of therapy and should discontinue SEROQUEL XR at the first sign of a decline in WBC in absence of other causative factors.
- Patients with neutropenia should be carefully monitored for fever or other symptoms or signs of infection and treated promptly if such symptoms or signs occur. Patients with severe neutropenia (absolute neutrophil count <1000/mm3) should discontinue SEROQUEL XR and have their WBC followed until recovery.
Cataracts
- The development of cataracts was observed in association with quetiapine treatment in chronic dog studies [see Nonclinical Toxicology (13.2)]. Lens changes have also been observed in adults, children, and adolescents during long-term quetiapine treatment but a causal relationship to quetiapine use has not been established. Nevertheless, the possibility of lenticular changes cannot be excluded at this time. Therefore, examination of the lens by methods adequate to detect cataract formation, such as slit lamp exam or other appropriately sensitive methods, is recommended at initiation of treatment or shortly thereafter, and at 6-month intervals during chronic treatment.
QT Prolongation
- In clinical trials quetiapine was not associated with a persistent increase in QT intervals. However, the QT effect was not systematically evaluated in a thorough QT study. In post marketing experience there were cases reported of QT prolongation in patients who overdosed on quetiapine [see Overdosage (10.1)], in patients with concomitant illness, and in patients taking medicines known to cause electrolyte imbalance or increase QT interval.
- The use of quetiapine should be avoided in combination with other drugs that are known to prolong QTc including Class 1A antiarrythmics (e.g., quinidine, procainamide) or Class III antiarrythmics (e.g., amiodarone, sotalol), antipsychotic medications (e.g., ziprasidone, chlorpromazine, thioridazine), antibiotics (e.g., gatifloxacin, moxifloxacin), or any other class of medications known to prolong the QTc interval (e.g., pentamidine, levomethadyl acetate, methadone).
- Quetiapine should also be avoided in circumstances that may increase the risk of occurrence of torsade de pointes and/or sudden death including (1) a history of cardiac arrhythmias such as bradycardia; (2) hypokalemia or hypomagnesemia; (3) concomitant use of other drugs that prolong the QTc interval; and (4) presence of congenital prolongation of the QT interval.
- Caution should also be exercised when quetiapine is prescribed in patients with increased risk of QT prolongation (e.g., cardiovascular disease, family history of QT prolongation, the elderly, congestive heart failure and heart hypertrophy).
Seizures
- During short-term clinical trials with SEROQUEL XR, seizures occurred in 0.05% (1/1866) of patients treated with SEROQUEL XR across all indications compared to 0.3% (3/928) on placebo. During clinical trials with SEROQUEL, seizures occurred in 0.5% (20/3490) of patients treated with SEROQUEL compared to 0.2% (2/954) on placebo. As with other antipsychotics, quetiapine fumarate should be used cautiously in patients with a history of seizures or with conditions that potentially lower the seizure threshold, e.g., Alzheimer’s dementia. Conditions that lower the seizure threshold may be more prevalent in a population of 65 years or older.
Hypothyroidism
- Adults: Clinical trials with quetiapine demonstrated dose-related decreases in thyroid hormone levels. The reduction in total and free thyroxine (T4) of approximately 20% at the higher end of the therapeutic dose range was maximal in the first six weeks of treatment and maintained without adaptation or progression during more chronic therapy. In nearly all cases, cessation of quetiapine treatment was associated with a reversal of the effects on total and free T4, irrespective of the duration of treatment. The mechanism by which quetiapine effects the thyroid axis is unclear. If there is an effect on the hypothalamic-pituitary axis, measurement of TSH alone may not accurately reflect a patient’s thyroid status. Therefore, both TSH and free T4, in addition to clinical assessment, should be measured at baseline and at follow-up.
- In SEROQUEL XR clinical trials across all indications 1.8% (24/1336) of patients on SEROQUEL XR versus 0.6% (3/530) on placebo experienced decreased free thyroxine (<0.8 LLN) and 1.6% (21/1346) on SEROQUEL XR versus 3.4% (18/534) on placebo experienced increased thyroid stimulating hormone (TSH). About 0.7% (26/3489) of SEROQUEL patients did experience TSH increases in monotherapy studies. Some patients with TSH increases needed replacement thyroid treatment.
- In all quetiapine trials, the incidence of shifts in thyroid hormones and TSH were1: decrease in free T4 (<0.8 LLN), 2.0% (357/17513); decrease in total T4, 4.0% (75/1861); decrease in free T3, 0.4% (53/13766); decrease in total T3, 2.0% (26/1312), and increase in TSH, 4.9% (956/19412). In eight patients, where TBG was measured, levels of TBG were unchanged.
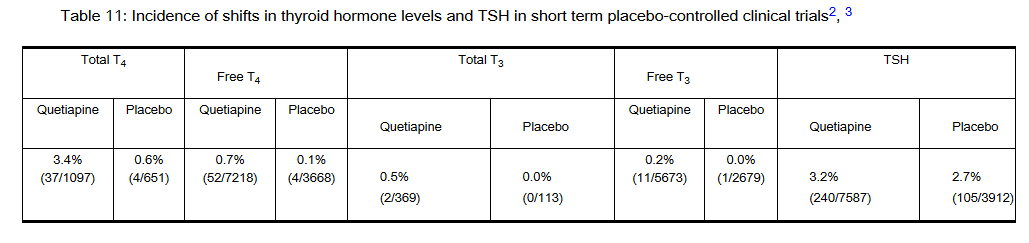
- Table 11 shows the incidence of these shifts in short term placebo-controlled clinical trials.
This image is provided by the National Library of Medicine.

- In short-term placebo-controlled monotherapy trials, the incidence of reciprocal shifts in T3 and TSH was 0.0 % for both quetiapine (1/4800) and placebo (0/2190) and for T4 and TSH the shifts were 0.1% (7/6154) for quetiapine versus 0.0 % (1/3007) for placebo.
- Children and Adolescents: Safety and effectiveness of SEROQUEL XR is supported by studies of SEROQUEL in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.1 and 14.2)].
- In acute placebo-controlled trials in children and adolescent patients with schizophrenia (6-week duration) or bipolar mania (3-week duration), the incidence of shifts at any time for SEROQUEL treated patients and placebo-treated patients for elevated TSH was 2.9% (8/280) vs. 0.7% (1/138), respectively and for decreased total thyroxine was 2.8% (8/289) vs. 0% (0/145), respectively. Of the SEROQUEL treated patients with elevated TSH levels, 1 had simultaneous low free T4 level at end of treatment.
- Based on shifts from normal baseline to potentially clinically important value at anytime post-baseline. Shifts in total T4, free T4, total T3 and free T3 are defined as <0.8 x LLN (pmol/L) and shift in TSH is > 5 mIU/L at any time.
- Based on shifts from normal baseline to potentially clinically important value at anytime post-baseline. Shifts in total T4, free T4, total T3 and free T3 are defined as <0.8 x LLN (pmol/L) and shift in TSH is >5 mIU/L at any time.
- Includes SEROQUEL and SEROQUEL XR data.
Hyperprolactinemia
- Adults: During clinical trials with quetiapine across all indications, the incidence of shifts in prolactin levels to a clinically significant value occurred in 3.6% (158/4416) of patients treated with quetiapine compared to 2.6% (51/1968) on placebo.
- Children and Adolescents: Safety and effectiveness of SEROQUEL XR is supported by studies of SEROQUEL in children and adolescent patients 10 to 17 years of age [see Clinical Studies (14.1 and 14.2)]. In acute placebo-controlled trials in children and adolescent patients with bipolar mania (3-week duration) or schizophrenia (6-week duration), the incidence of shifts in prolactin levels to a value (>20 µg/L males; > 26 µg/L females at any time) was 13.4% (18/134) for SEROQUEL compared to 4% (3/75) for placebo in males and 8.7% (9/104) for SEROQUEL compared to 0% (0/39) for placebo in females.
- Like other drugs that antagonize dopamine D2 receptors, SEROQUEL XR elevates prolactin levels in some patients and the elevation may persist during chronic administration. Hyperprolactinemia, regardless of etiology, may suppress hypothalamic GnRH, resulting in reduced pituitary gonadotrophin secretion. This, in turn, may inhibit reproductive function by impairing gonadal steroidogenesis in both female and male patients. Galactorrhea, amenorrhea, gynecomastia, and impotence have been reported in patients receiving prolactin-elevating compounds. Long-standing hyperprolactinemia when associated with hypogonadism may lead to decreased bone density in both female and male subjects.
- Tissue culture experiments indicate that approximately one-third of human breast cancers are prolactin dependent in vitro, a factor of potential importance if the prescription of these drugs is considered in a patient with previously detected breast cancer. As is common with compounds which increase prolactin release, mammary gland, and pancreatic islet cell neoplasia (mammary adenocarcinomas, pituitary and pancreatic adenomas) was observed in carcinogenicity studies conducted in mice and rats. Neither clinical studies nor epidemiologic studies conducted to date have shown an association between chronic administration of this class of drugs and tumorigenesis in humans, but the available evidence is too limited to be conclusive [see Nonclinical Toxicology (13.1)].
Potential for Cognitive and Motor Impairment
- Somnolence was a commonly reported adverse reaction reported in patients treated with quetiapine especially during the 3-day period of initial dose titration. In schizophrenia trials, somnolence was reported in 24.7% (235/951) of patients on SEROQUEL XR compared to 10.3% (33/319) of placebo patients. In a bipolar depression clinical trial, somnolence was reported in 51.8% (71/137) of patients on SEROQUEL XR compared to 12.9% (18/140) of placebo patients. In a clinical trial for bipolar mania, somnolence was reported in 50.3% (76/151) of patients on SEROQUEL XR compared to 11.9% (19/160) of placebo patients. Since quetiapine has the potential to impair judgment, thinking, or motor skills, patients should be cautioned about performing activities requiring mental alertness, such as operating a motor vehicle (including automobiles) or operating hazardous machinery until they are reasonably certain that quetiapine therapy does not affect them adversely. Somnolence may lead to falls.
- In short-term adjunctive therapy trials for MDD, somnolence was reported in 40% (252/627) of patients on SEROQUEL XR respectively compared to 9% (27/309) of placebo patients. Somnolence was dose-related in these trials (37% (117/315) and 43% (135/312) for the 150 mg and 300 mg groups, respectively).
Body Temperature Regulation
- Disruption of the body's ability to reduce core body temperature has been attributed to antipsychotic agents. Appropriate care is advised when prescribing SEROQUEL XR for patients who will be experiencing conditions which may contribute to an elevation in core body temperature, eg, exercising strenuously, exposure to extreme heat, receiving concomitant medication with anticholinergic activity, or being subject to dehydration.
Dysphagia
- Esophageal dysmotility and aspiration have been associated with antipsychotic drug use. Aspiration pneumonia is a common cause of morbidity and mortality in elderly patients, in particular those with advanced Alzheimer's dementia. SEROQUEL XR and other antipsychotic drugs should be used cautiously in patients at risk for aspiration pneumonia.
Discontinuation Syndrome
- Acute withdrawal symptoms, such as insomnia, nausea and vomiting have been described after abrupt cessation of atypical antipsychotic drugs, including quetiapine fumarate. In short-term placebo-controlled, monotherapy clinical trials with SEROQUEL XR that included a discontinuation phase which evaluated discontinuation symptoms, the aggregated incidence of patients experiencing one or more discontinuation symptoms after abrupt cessation was 12.1% (241/1993) for SEROQUEL XR and 6.7% (71/1065) for placebo. The incidence of the individual adverse reactions (i.e., insomnia, nausea, headache, diarrhea, vomiting, dizziness and irritability) did not exceed 5.3% in any treatment group and usually resolved after 1 week post-discontinuation. Gradual dose reduction is advised.
- The following adverse reactions are discussed in more detail in other sections of the labeling:
- Increased mortality in elderly patients with dementia-related psychosis
- Suicidal thoughts and behaviors in adolescents and young adults
- Cerebrovascular adverse reactions, including stroke in elderly patients with dementia-related psychosis
- Neuroleptic Malignant Syndrome (NMS)
- Metabolic changes (hyperglycemia, dyslipidemia, weight gain)
- Tardive dyskinesia
- Hypotension
- Increases in blood pressure (children and adolescents)
- Leukopenia, neutropenia and agranulocytosis
- Cataracts
- QT Prolongation
- Seizures
- Hypothyroidism
- Hyperprolactinemia
- Potential for cognitive and motor impairment
- Body temperature regulation
- Dysphagia
- Discontinuation Syndrome
Adverse Reactions
Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
- Adults
- The information below is derived from a clinical trial database for SEROQUEL XR consisting of approximately 3400 patients exposed to SEROQUEL XR for the treatment of Schizophrenia, Bipolar Disorder, and Major Depressive Disorder in placebo-controlled trials. This experience corresponds to approximately 1020.1 patient-years. Adverse reactions were assessed by collecting adverse reactions, results of physical examinations, vital signs, body weights, laboratory analyses and ECG results.
- The stated frequencies of adverse reactions represent the proportion of individuals who experienced, at least once, an adverse reaction of the type listed.
- Adverse Reactions Associated with Discontinuation of Treatment in Short-Term, Placebo-Controlled Trials
- Schizophrenia: There were no adverse reactions leading to discontinuation that occurred at an incidence of ≥ 2% for SEROQUEL XR in schizophrenia trials.
- Bipolar I Disorder, Manic or Mixed Episodes:
- There were no adverse reactions leading to discontinuation that occurred at an incidence of ≥ 2% for SEROQUEL XR in the bipolar mania trial.
- Bipolar Disorder, Depressive Episode: In a single clinical trial in patients with bipolar depression, 14% (19/137) of patients on SEROQUEL XR discontinued due to an adverse reaction compared to 4% (5/140) on placebo. Somnolence4 was the only adverse reaction leading to discontinuation that occurred at an incidence of ≥ 2% in SEROQUEL XR in the bipolar depression trial.
- MDD, Adjunctive Therapy: In adjunctive therapy clinical trials in patients with MDD, 12.1% (76/627) of patients on SEROQUEL XR discontinued due to adverse reaction compared to 1.9% (6/309) on placebo. Somnolence4 was the only adverse reaction leading to discontinuation that occurred at an incidence of ≥ 2% in SEROQUEL XR in MDD trials.
- Commonly Observed Adverse Reactions in Short-Term, Placebo-Controlled Trials:
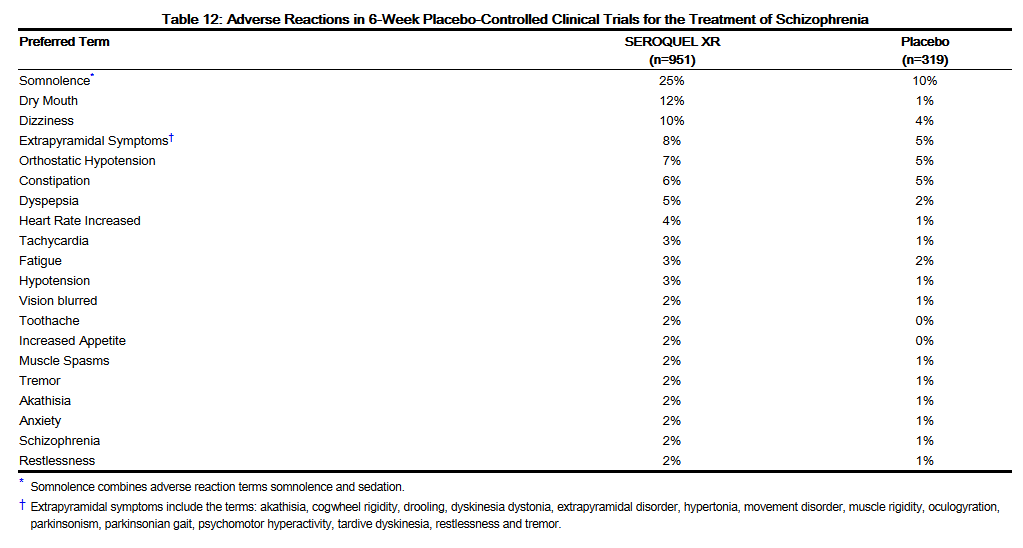
- In short-term placebo-controlled studies for schizophrenia the most commonly observed adverse reactions associated with the use of SEROQUEL XR (incidence of 5% or greater) and observed at a rate on SEROQUEL XR at least twice that of placebo were somnolence (25%), dry mouth (12%), dizziness (10%), and dyspepsia (5%).
- Adverse Reactions Occurring at an Incidence of 2% or More Among SEROQUEL XR Treated Patients in Short-Term, Placebo-Controlled Trials
- Table 12 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy of schizophrenia (up to 6 weeks) in 2% or more in patients treated with SEROQUEL XR (doses ranging from 300 to 800 mg/day) where the incidence in patients treated with SEROQUEL XR was greater than the incidence in placebo-treated patients.
This image is provided by the National Library of Medicine.

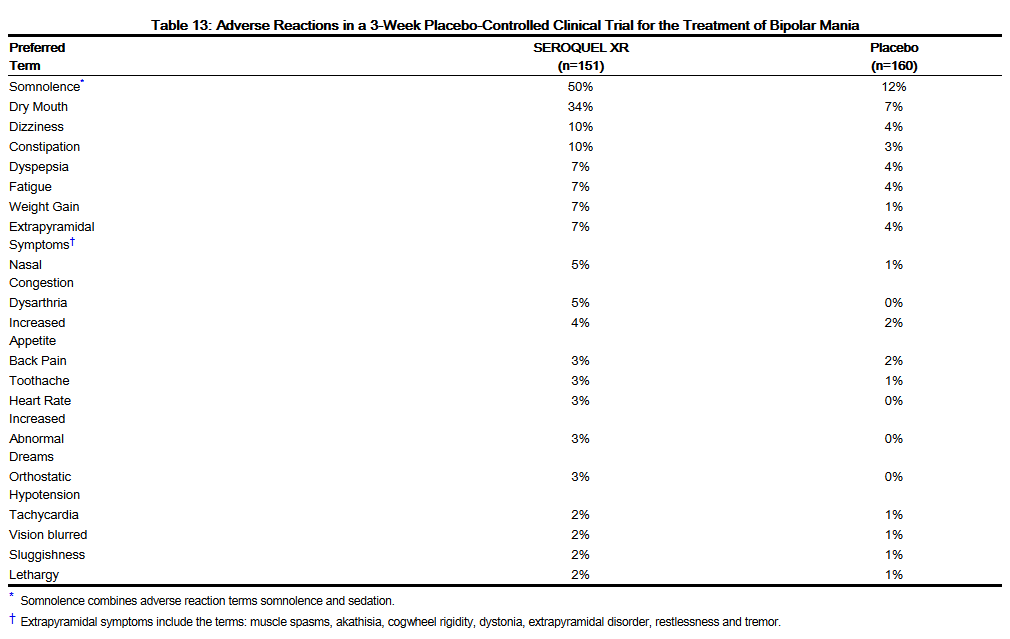
- In a 3-week, placebo-controlled study in bipolar mania the most commonly observed adverse reactions associated with the use of SEROQUEL XR (incidence of 5% or greater) and observed at a rate on SEROQUEL XR at least twice that of placebo were somnolence (50%), dry mouth (34%), dizziness (10%), constipation (10%), weight gain (7%), dysarthria (5%), and nasal congestion (5%).
- Table 13 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy of bipolar mania (up to 3 weeks) in 2% or more of patients treated with SEROQUEL XR (doses ranging from 400 to 800 mg/day) where the incidence in patients treated with SEROQUEL XR was greater than the incidence in placebo-treated patients.
This image is provided by the National Library of Medicine.

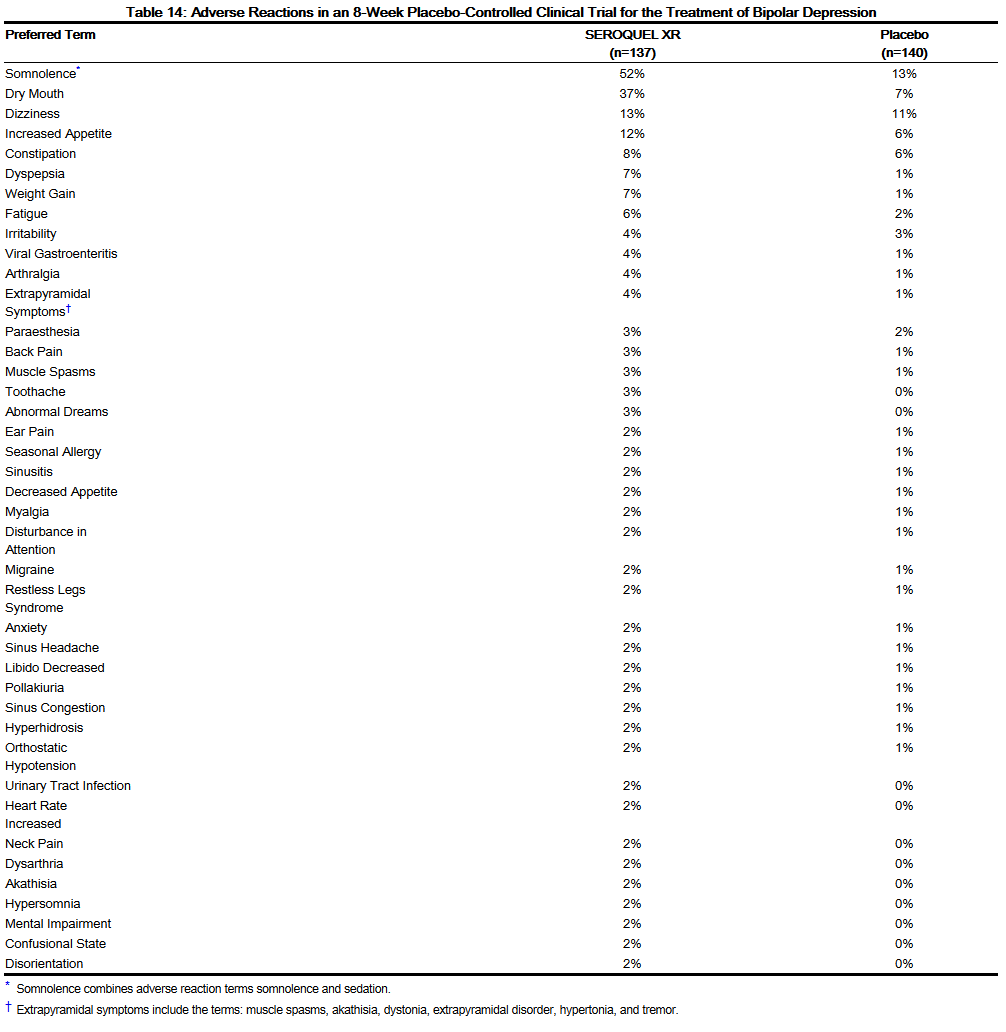
- In the 8-week placebo-controlled bipolar depression study in adults, the most commonly observed adverse reactions associated with the use of SEROQUEL XR (incidence of 5% or greater) and observed at a rate on SEROQUEL XR at least twice that of placebo were somnolence (52%), dry mouth (37%), increased appetite (12%), weight gain (7%), dyspepsia (7%), and fatigue (6%).
- Table 14 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during acute therapy of bipolar depression (up to 8 weeks) in 2% or more of adult patients treated with SEROQUEL XR 300 mg/day where the incidence in patients treated with SEROQUEL XR was greater than the incidence in placebo-treated patients.
This image is provided by the National Library of Medicine.

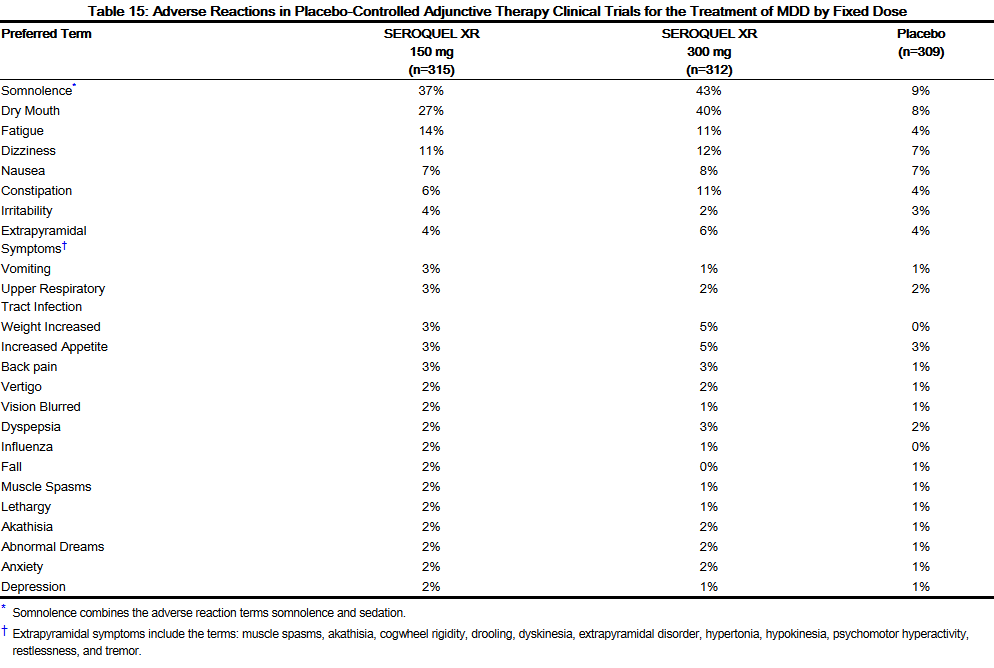
- In the 6-week placebo-controlled fixed dose adjunctive therapy clinical trials, for MDD, the most commonly observed adverse reactions associated with the use of SEROQUEL XR (incidence of 5% or greater and observed at a rate on SEROQUEL XR and at least twice that of placebo) were somnolence (150 mg: 37%; 300 mg: 43%), dry mouth (150 mg: 27%; 300 mg: 40%), fatigue (150 mg: 14%; 300 mg: 11%), constipation 300 mg only: 11%) and weight increased (300 mg only: 5%).
- Table 15 enumerates the incidence, rounded to the nearest percent, of adverse reactions that occurred during short-term adjunctive therapy of MDD (up to 6 weeks) in 2% or more of patients treated with SEROQUEL XR (at doses of either 150 mg or 300 mg/day) where the incidence in patients treated with SEROQUEL XR was greater than the incidence in placebo-treated patients.
This image is provided by the National Library of Medicine.

- Adverse Reactions in clinical trials with quetiapine and not listed elsewhere in the label:
- Pyrexia, nightmares, peripheral edema, dyspnea, palpitations, rhinitis, eosinophilia, hypersensitivity, elevations in gamma-GT levels, and elevations in serum creatine phosphokinase (not associated with NMS), somnambulism (and other related events), hypothermia, decreased platelets, galactorrhea, bradycardia (which may occur at or near initiation of treatment and be associated with hypotension and/ or syncope), and priapism.
- Extrapyramidal Symptoms (EPS):
- Dystonia
- Class Effect: Symptoms of dystonia, prolonged abnormal contractions of muscle groups, may occur in susceptible individuals during the first few days of treatment. Dystonic symptoms include: spasm of the neck muscles, sometimes progressing to tightness of the throat, swallowing difficulty, difficulty breathing, and/or protrusion of the tongue. While these symptoms can occur at low doses, they occur more frequently and with greater severity with high potency and at higher doses of first generation antipsychotic drugs. An elevated risk of acute dystonia is observed in males and younger age groups.
- Dystonia
Four methods were used to measure EPS: (1) Simpson-Angus total score (mean change from baseline) which evaluates Parkinsonism and akathisia, (2) Barnes Akathisia Rating Scale (BARS) Global Assessment Score, (3) incidence of spontaneous complaints of EPS (akathisia, akinesia, cogwheel rigidity, extrapyramidal syndrome, hypertonia, hypokinesia, neck rigidity, and tremor), and (4) use of anticholinergic medications to treat emergent EPS.
Adults: In placebo-controlled clinical trials with quetiapine, utilizing doses up to 800 mg per day, the incidence of any adverse reactions related to EPS ranged from 8% to 11% for quetiapine and 4% to 11% for placebo.
In three-arm placebo-controlled clinical trials for the treatment of schizophrenia, utilizing doses between 300 mg and 800 mg of SEROQUEL XR, the incidence of any adverse reactions related to EPS was 8% for SEROQUEL XR and 8% for SEROQUEL (without evidence of being dose related), and 5% in the placebo group. In these studies, the incidence of the individual adverse reactions (akathisia, extrapyramidal disorder, tremor, dyskinesia, dystonia, restlessness, and muscle rigidity) was generally low and did not exceed 3% for any treatment group.
At the end of treatment, the mean change from baseline in SAS total score and BARS Global Assessment score was similar across the treatment groups. The use of concomitant anticholinergic medications was infrequent and similar across the treatment groups. The incidence of extrapyramidal symptoms was consistent with that seen with the profile of SEROQUEL in schizophrenia patients.
In Tables 16-19, dystonic event included nuchal rigidity, hypertonia, dystonia, muscle rigidity, oculogyration; parkinsonism included cogwheel rigidity, tremor, drooling, hypokinesia; akathisia included akathisia, psychomotor agitation; dyskinetic event included tardive dyskinesia, dyskinesia, choreoathetosis; and other extrapyramidal event included restlessness, extrapyramidal disorder, movement disorder.
Body as a Whole
Cardiovascular
Digestive
Endocrine
Hematologic and Lymphatic
Metabolic and Nutritional
Musculoskeletal
Neurologic
Respiratory
Skin and Hypersensitivy Reactions
Special Senses
Urogenital
Miscellaneous
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Quetiapine in the drug label.
Body as a Whole
Cardiovascular
Digestive
Endocrine
Hematologic and Lymphatic
Metabolic and Nutritional
Musculoskeletal
Neurologic
Respiratory
Skin and Hypersensitivy Reactions
Special Senses
Urogenital
Miscellaneous
Drug Interactions
- Drug
- Description
Use in Specific Populations
Pregnancy
- Pregnancy Category
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Quetiapine in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Quetiapine during labor and delivery.
Nursing Mothers
There is no FDA guidance on the use of Quetiapine with respect to nursing mothers.
Pediatric Use
There is no FDA guidance on the use of Quetiapine with respect to pediatric patients.
Geriatic Use
There is no FDA guidance on the use of Quetiapine with respect to geriatric patients.
Gender
There is no FDA guidance on the use of Quetiapine with respect to specific gender populations.
Race
There is no FDA guidance on the use of Quetiapine with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Quetiapine in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Quetiapine in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Quetiapine in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Quetiapine in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
- Intravenous
Monitoring
There is limited information regarding Monitoring of Quetiapine in the drug label.
- Description
IV Compatibility
There is limited information regarding IV Compatibility of Quetiapine in the drug label.
Overdosage
Acute Overdose
Signs and Symptoms
- Description
Management
- Description
Chronic Overdose
There is limited information regarding Chronic Overdose of Quetiapine in the drug label.
Pharmacology
There is limited information regarding Quetiapine Pharmacology in the drug label.
Mechanism of Action
Structure
This image is provided by the National Library of Medicine.
Pharmacodynamics
There is limited information regarding Pharmacodynamics of Quetiapine in the drug label.
Pharmacokinetics
There is limited information regarding Pharmacokinetics of Quetiapine in the drug label.
Nonclinical Toxicology
There is limited information regarding Nonclinical Toxicology of Quetiapine in the drug label.
Clinical Studies
There is limited information regarding Clinical Studies of Quetiapine in the drug label.
How Supplied
Storage
There is limited information regarding Quetiapine Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Quetiapine |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Quetiapine |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
There is limited information regarding Patient Counseling Information of Quetiapine in the drug label.
Precautions with Alcohol
- Alcohol-Quetiapine interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- ®[1]
Look-Alike Drug Names
- A® — B®[2]
Drug Shortage Status
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Empty citation (help)
- ↑ "http://www.ismp.org". External link in
|title=(help)
{{#subobject:
|Page Name=Quetiapine |Pill Name=No image.jpg |Drug Name= |Pill Ingred=|+sep=; |Pill Imprint= |Pill Dosage= |Pill Color=|+sep=; |Pill Shape= |Pill Size (mm)= |Pill Scoring= |Pill Image= |Drug Author= |NDC=
}}
{{#subobject:
|Label Page=Quetiapine |Label Name=Quetiapine11.png
}}
{{#subobject:
|Label Page=Quetiapine |Label Name=Quetiapine11.png
}}