** It has been shown in rats that [[Neuron|neurons]] sometimes die completely 24 hours after the [[blood flow]] returns. Some claim that this delayed reaction is the result of the multiple [[Inflammation|inflammatory]] [[immune responses]] that occur during [[reperfusion]]. Such inflammatory reactions cause i[[Intracranial pressure|ntracranial pressure]], a pressure that leads to [[Cell disruption|cell damage]] and [[cell death]] in some cases. [[Hypothermia]] has been shown to help reduce [[intracranial pressure]] and thus decrease the adverse effects of inflammatory immune responses during [[reperfusion]]<ref>Adler, Jerry. "Back From the Dead." Newsweek. July 23, 2007</ref>. Besides that, reperfusion also increases [[Free-radical theory|free radical]] development. [[Hypothermia]] has also been shown to decrease the patient's development of deadly [[free radicals]] during [[reperfusion]]<ref name="pmid14767591">{{cite journal |vauthors=Polderman KH |title=Application of therapeutic hypothermia in the ICU: opportunities and pitfalls of a promising treatment modality. Part 1: Indications and evidence |journal=Intensive Care Med |volume=30 |issue=4 |pages=556–75 |date=April 2004 |pmid=14767591 |doi=10.1007/s00134-003-2152-x |url=}}</ref>.
** It has been shown in rats that [[Neuron|neurons]] sometimes die completely 24 hours after the [[blood flow]] returns. Some claim that this delayed reaction is the result of the multiple [[Inflammation|inflammatory]] [[immune responses]] that occur during [[reperfusion]]. Such inflammatory reactions cause i[[Intracranial pressure|ntracranial pressure]], a pressure that leads to [[Cell disruption|cell damage]] and [[cell death]] in some cases. [[Hypothermia]] has been shown to help reduce [[intracranial pressure]] and thus decrease the adverse effects of inflammatory immune responses during [[reperfusion]]. Besides that, reperfusion also increases [[Free-radical theory|free radical]] development. [[Hypothermia]] has also been shown to decrease the patient's development of deadly [[free radicals]] during [[reperfusion]].
*'''Hydrogen sulfide treatment'''
*'''Hydrogen sulfide treatment'''
** There are several preliminary studies in mice that seem to show that treatment with [[hydrogen sulfide]] ( H2S) could have a protective effect against [[reperfusion injury]]<ref>Elrod J.W., J.W. Calvert, M.R. Duranski, D.J. Lefer. "Hydrogen sulfide donor protects against acute myocardial ischemia-reperfusion injury." Circulation 114(18):II172, 2006</ref>
** There are several preliminary studies in mice that seem to show that treatment with [[hydrogen sulfide]] ( H2S) could have a protective effect against [[reperfusion injury]]
*'''Cyclosporine'''
*'''Cyclosporine'''
** In addition to its well-known [[Immunosuppression|immunosuppressive]] capabilities, the one-time administration of [[cyclosporine]] at the time of [[percutaneous coronary intervention]] (PCI) has been found to deliver a 40 percent reduction in [[infarct]] size in a small group proof of concept study of human patients with [[reperfusion injury]] published in The New England Journal of Medicine in 2008<ref name="pmid18669426">{{cite journal |vauthors=Piot C, Croisille P, Staat P, Thibault H, Rioufol G, Mewton N, Elbelghiti R, Cung TT, Bonnefoy E, Angoulvant D, Macia C, Raczka F, Sportouch C, Gahide G, Finet G, André-Fouët X, Revel D, Kirkorian G, Monassier JP, Derumeaux G, Ovize M |title=Effect of cyclosporine on reperfusion injury in acute myocardial infarction |journal=N. Engl. J. Med. |volume=359 |issue=5 |pages=473–81 |date=July 2008 |pmid=18669426 |doi=10.1056/NEJMoa071142 |url=}}</ref>.[[File:Myocardial Treatment In IRI.jpg|thumb|Treatment OF IRI]][[Cyclosporine]] has been confirmed in studies to inhibit the actions of [[Cyclophilin|cyclophilin D]], a protein which is induced by excessive [[Intracellular calcium-sensing proteins|intracellular calcium]] flow to interact with other pore components and help open the [[Mitochondrial membrane transport protein|MPT pore]]. Inhibiting [[Cyclophilin|cyclophilin D]] has been shown to prevent the opening of the MPT pore and protect the [[Mitochondrion|mitochondria]] and cellular energy production from excessive [[calcium]] inflows<ref name="pmid17595511">{{cite journal |vauthors=Javadov S, Karmazyn M |title=Mitochondrial permeability transition pore opening as an endpoint to initiate cell death and as a putative target for cardioprotection |journal=Cell. Physiol. Biochem. |volume=20 |issue=1-4 |pages=1–22 |date=2007 |pmid=17595511 |doi=10.1159/000103747 |url=}}</ref>.
** In addition to its well-known [[Immunosuppression|immunosuppressive]] capabilities, the one-time administration of [[cyclosporine]] at the time of [[percutaneous coronary intervention]] (PCI) has been found to deliver a 40 percent reduction in [[infarct]] size in a small group proof of concept study of human patients with [[reperfusion injury]] published in The New England Journal of Medicine in 2008.
**Cyclosporine works by inhibiting the action of Cyclophilin D which usually helps in opening Mitochondrial membrane transport protein ( MPT Pore). So once cyclophilin D action is inhibited, there is no more MPT pore opening and in turn saves the mitochondria from getting damaged.[[File:Myocardial Treatment In IRI.jpg|thumb|Treatment OF IRI]].
**The opening of MTP Pore results in major cell destruction by causing the influx of water into mitochondria and in turn impairing its function and ultimately leading to the collapse. The strategy to protect mitochondria is the most important thing associated with the treatment part.
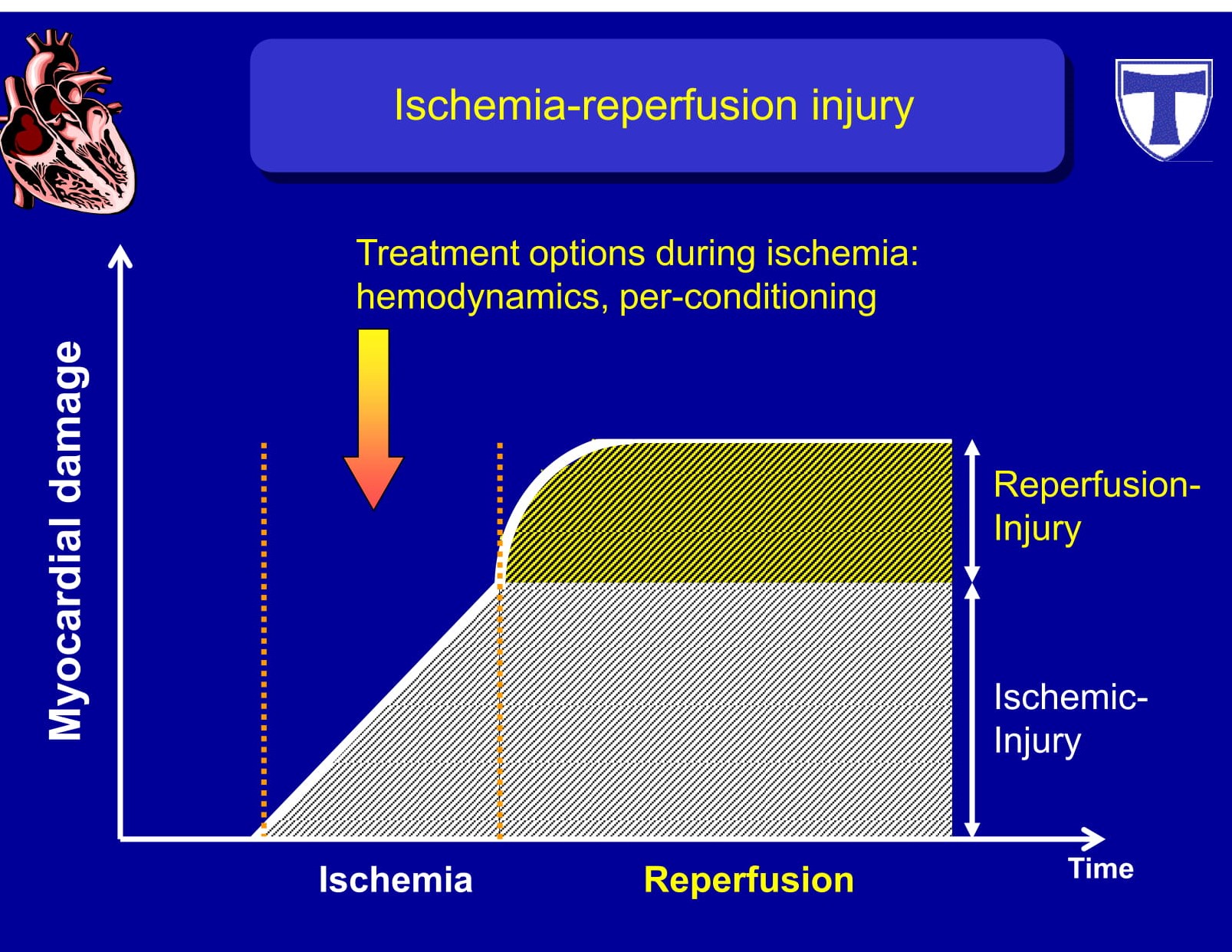
**[[Reperfusion]] leads to biochemical imbalances within the cell that lead to [[cell death]] and increased [[Infarct|infarct size]]. More specifically, [[calcium]] overload and excessive production of [[Reactive oxygen species|reactive oxygen]] species in the first few minutes after [[reperfusion]] set off a cascade of biochemical changes that result in the opening of the so-called [[Mitochondrial permeability transition|mitochondrial permeability transition pore]] (MPT pore) in the [[mitochondrial membrane]] of [[Heart|cardiac cells]].
**[[Reperfusion]] leads to biochemical imbalances within the cell that lead to [[cell death]] and increased [[Infarct|infarct size]]. More specifically, [[calcium]] overload and excessive production of [[Reactive oxygen species|reactive oxygen]] species in the first few minutes after [[reperfusion]] set off a cascade of biochemical changes that result in the opening of the so-called [[Mitochondrial permeability transition|mitochondrial permeability transition pore]] (MPT pore) in the [[mitochondrial membrane]] of [[Heart|cardiac cells]].
**<nowiki/>The opening of the MPT pore leads to the inrush of water into the [[mitochondria]], resulting in [[Mitochondrion|mitochondrial]] dysfunction and [[Collapse (medical)|collapse]]. Upon collapse, the [[calcium]] is then released to overwhelm the next [[Mitochondrion|mitochondria]] in a cascading series of events that cause [[Mitochondrion|mitochondria]]<nowiki/>l energy production supporting the cell to be reduced or stopped completely. The cessation of [[energy]] production results in [[cellular death]]. Protecting [[Mitochondrion|mitochondria]] is a viable [[cardio]] protective strategy<ref name="pmid26321103">{{cite journal |vauthors=Cung TT, Morel O, Cayla G, Rioufol G, Garcia-Dorado D, Angoulvant D, Bonnefoy-Cudraz E, Guérin P, Elbaz M, Delarche N, Coste P, Vanzetto G, Metge M, Aupetit JF, Jouve B, Motreff P, Tron C, Labeque JN, Steg PG, Cottin Y, Range G, Clerc J, Claeys MJ, Coussement P, Prunier F, Moulin F, Roth O, Belle L, Dubois P, Barragan P, Gilard M, Piot C, Colin P, De Poli F, Morice MC, Ider O, Dubois-Randé JL, Unterseeh T, Le Breton H, Béard T, Blanchard D, Grollier G, Malquarti V, Staat P, Sudre A, Elmer E, Hansson MJ, Bergerot C, Boussaha I, Jossan C, Derumeaux G, Mewton N, Ovize M |title=Cyclosporine before PCI in Patients with Acute Myocardial Infarction |journal=N. Engl. J. Med. |volume=373 |issue=11 |pages=1021–31 |date=September 2015 |pmid=26321103 |doi=10.1056/NEJMoa1505489 |url=}}</ref>.
**<nowiki/>The opening of the MPT pore leads to the inrush of water into the [[mitochondria]], resulting in [[Mitochondrion|mitochondrial]] dysfunction and [[Collapse (medical)|collapse]]. Upon collapse, the [[calcium]] is then released to overwhelm the next [[Mitochondrion|mitochondria]] in a cascading series of events that cause [[Mitochondrion|mitochondria]]<nowiki/>l energy production supporting the cell to be reduced or stopped completely. The cessation of [[energy]] production results in [[cellular death]]. Protecting [[Mitochondrion|mitochondria]] is a viable [[cardio]] protective strategy.
**[[Cyclosporine]] is currently in a phase II/III (adaptive) clinical study in Europe to determine its ability to [[ameliorate]] [[neuronal]] cellular damage in traumatic [[brain injury]]<ref name="pmid21142667">{{cite journal |vauthors=Sullivan PG, Sebastian AH, Hall ED |title=Therapeutic window analysis of the neuroprotective effects of cyclosporine A after traumatic brain injury |journal=J. Neurotrauma |volume=28 |issue=2 |pages=311–8 |date=February 2011 |pmid=21142667 |pmc=3037811 |doi=10.1089/neu.2010.1646 |url=}}</ref>.
**[[Cyclosporine]] is currently in a phase II/III (adaptive) clinical study in Europe to determine its ability to [[ameliorate]] [[neuronal]] cellular damage in traumatic [[brain injury]].
*'''TRO40303'''
*'''TRO40303'''
** TRO40303 is a new [[cardio]] protective compound that was shown to inhibit the [[Mitochondrial membrane transport protein|MP]]<nowiki/>[[Mitochondrial membrane transport protein|T pore]] and reduce [[infarct]] size after [[ischemia]]-[[reperfusion]]<ref name="pmid24507657">{{cite journal |vauthors=Le Lamer S, Paradis S, Rahmouni H, Chaimbault C, Michaud M, Culcasi M, Afxantidis J, Latreille M, Berna P, Berdeaux A, Pietri S, Morin D, Donazzolo Y, Abitbol JL, Pruss RM, Schaller S |title=Translation of TRO40303 from myocardial infarction models to demonstration of safety and tolerance in a randomized Phase I trial |journal=J Transl Med |volume=12 |issue= |pages=38 |date=February 2014 |pmid=24507657 |pmc=3923730 |doi=10.1186/1479-5876-12-38 |url=}}</ref>.
** TRO40303 is a new [[cardio]] protective compound that was shown to inhibit the [[Mitochondrial membrane transport protein|MP]]<nowiki/>[[Mitochondrial membrane transport protein|T pore]] and reduce [[infarct]] size after [[ischemia]]-[[reperfusion]].
*'''Stem cell therapy'''
*'''Stem cell therapy'''
** Recent investigations suggest a possible beneficial effect of [[Mesenchymal stem cell|mesenchymal stem cells]] on heart and kidney [[reperfusion injury]]<ref name="pmid21498423">{{cite journal |vauthors=van der Spoel TI, Jansen of Lorkeers SJ, Agostoni P, van Belle E, Gyöngyösi M, Sluijter JP, Cramer MJ, Doevendans PA, Chamuleau SA |title=Human relevance of pre-clinical studies in stem cell therapy: systematic review and meta-analysis of large animal models of ischaemic heart disease |journal=Cardiovasc. Res. |volume=91 |issue=4 |pages=649–58 |date=September 2011 |pmid=21498423 |doi=10.1093/cvr/cvr113 |url=}}</ref>
** Recent investigations suggest a possible beneficial effect of [[Mesenchymal stem cell|mesenchymal stem cells]] on heart and kidney [[reperfusion injury]]
<ref name="pmid24220681">{{cite journal |vauthors=Zhao JJ, Liu JL, Liu L, Jia HY |title=Protection of mesenchymal stem cells on acute kidney injury |journal=Mol Med Rep |volume=9 |issue=1 |pages=91–6 |date=January 2014 |pmid=24220681 |doi=10.3892/mmr.2013.1792 |url=}}</ref>
*'''Superoxide dismutase'''
*'''Superoxide dismutase'''
**[[Superoxide dismutase]] is an important [[antioxidant]] enzyme that transforms [[superoxide]] [[anions]] into water and [[hydrogen peroxide]]. Recent work has demonstrated important therapeutic effects on pre-clinical models of [[reperfusion]] damage following an [[ischemic stroke]]<ref name="pmid26928528">{{cite journal |vauthors=Jiang Y, Arounleut P, Rheiner S, Bae Y, Kabanov AV, Milligan C, Manickam DS |title=SOD1 nanozyme with reduced toxicity and MPS accumulation |journal=J Control Release |volume=231 |issue= |pages=38–49 |date=June 2016 |pmid=26928528 |doi=10.1016/j.jconrel.2016.02.038 |url=}}</ref><ref name="pmid26093094">{{cite journal |vauthors=Jiang Y, Brynskikh AM, S-Manickam D, Kabanov AV |title=SOD1 nanozyme salvages ischemic brain by locally protecting cerebral vasculature |journal=J Control Release |volume=213 |issue= |pages=36–44 |date=September 2015 |pmid=26093094 |pmc=4684498 |doi=10.1016/j.jconrel.2015.06.021 |url=}}</ref>.
**[[Superoxide dismutase]] is an important [[antioxidant]] enzyme that transforms [[superoxide]] [[anions]] into water and [[hydrogen peroxide]]. Recent work has demonstrated important therapeutic effects on pre-clinical models of [[reperfusion]] damage following an [[ischemic stroke]].
*'''Metformin'''
*'''Metformin'''
** A series of 2009 studies published in the Journal of [[Cardiovascular]] Pharmacology indicate that [[metformin]] may prevent injury to [[cardiac]] [[reperfusion]] by inhibiting Mitochondrial Complex I and opening up MPT pore and in rats<ref name="pmid19295441">{{cite journal |vauthors=Paiva M, Riksen NP, Davidson SM, Hausenloy DJ, Monteiro P, Gonçalves L, Providência L, Rongen GA, Smits P, Mocanu MM, Yellon DM |title=Metformin prevents myocardial reperfusion injury by activating the adenosine receptor |journal=J. Cardiovasc. Pharmacol. |volume=53 |issue=5 |pages=373–8 |date=May 2009 |pmid=19295441 |doi=10.1097/FJC.0b013e31819fd4e7 |url=}}</ref><ref name="pmid18080084">{{cite journal |vauthors=Bhamra GS, Hausenloy DJ, Davidson SM, Carr RD, Paiva M, Wynne AM, Mocanu MM, Yellon DM |title=Metformin protects the ischemic heart by the Akt-mediated inhibition of mitochondrial permeability transition pore opening |journal=Basic Res. Cardiol. |volume=103 |issue=3 |pages=274–84 |date=May 2008 |pmid=18080084 |doi=10.1007/s00395-007-0691-y |url=}}</ref>.
** A series of 2009 studies published in the Journal of [[Cardiovascular]] Pharmacology indicate that [[metformin]] may prevent injury to [[cardiac]] [[reperfusion]] by inhibiting Mitochondrial Complex I and opening up MPT pore and in rats.
*'''Cannabinoids'''
*'''Cannabinoids'''
** A research published in 2012 shows that the synthetic analog of phytocannabinoid [[tetrahydrocannabivarin]] (THCV), 8-Tetrahydrocannabivarin (THCV) and its 11-OH-8-THCV metabolite prevents [[hepatic]] ischemia/reperfusion injury by minimizing [[oxidative stress]] and [[inflammatory]] reactions through cannabinoid CB2 receptors, thereby lowering [[tissue]] damage and protective effects of [[inflammation]]. Pretreatment with a [[Cannabinoid receptor|CB2]] receptor antagonist, whereas a [[CB1]] antagonist appeared to strengthen it, attenuated the defensive effects of somewhere else<ref name="pmid21470208">{{cite journal |vauthors=Bátkai S, Mukhopadhyay P, Horváth B, Rajesh M, Gao RY, Mahadevan A, Amere M, Battista N, Lichtman AH, Gauson LA, Maccarrone M, Pertwee RG, Pacher P |title=Δ8-Tetrahydrocannabivarin prevents hepatic ischaemia/reperfusion injury by decreasing oxidative stress and inflammatory responses through cannabinoid CB2 receptors |journal=Br. J. Pharmacol. |volume=165 |issue=8 |pages=2450–61 |date=April 2012 |pmid=21470208 |pmc=3423240 |doi=10.1111/j.1476-5381.2011.01410.x |url=}}</ref>.
** A research published in 2012 shows that the synthetic analog of phytocannabinoid [[tetrahydrocannabivarin]] (THCV), 8-Tetrahydrocannabivarin (THCV) and its 11-OH-8-THCV metabolite prevents [[hepatic]] ischemia/reperfusion injury by minimizing [[oxidative stress]] and [[inflammatory]] reactions through cannabinoid CB2 receptors, thereby lowering [[tissue]] damage and protective effects of [[inflammation]]. Pretreatment with a [[Cannabinoid receptor|CB2]] receptor antagonist, whereas a [[CB1]] antagonist appeared to strengthen it, attenuated the defensive effects of somewhere else.
** An earlier study published in 2011 found that [[cannabidiol]] (CBD) also protects against [[hepatic]] ischemia/reperfusion injury by attenuating [[inflammatory]] signals and [[oxidative]] and nitrative stress response, resulting in [[cell]] death and [[tissue]] damage, but is independent of classic [[Cannabinoid receptor type 1|CB1]] and [[Cannabinoid receptor|CB]]2 receptors<ref name="pmid21362471">{{cite journal |vauthors=Mukhopadhyay P, Rajesh M, Horváth B, Bátkai S, Park O, Tanchian G, Gao RY, Patel V, Wink DA, Liaudet L, Haskó G, Mechoulam R, Pacher P |title=Cannabidiol protects against hepatic ischemia/reperfusion injury by attenuating inflammatory signaling and response, oxidative/nitrative stress, and cell death |journal=Free Radic. Biol. Med. |volume=50 |issue=10 |pages=1368–81 |date=May 2011 |pmid=21362471 |pmc=3081988 |doi=10.1016/j.freeradbiomed.2011.02.021 |url=}}</ref>.
** An earlier study published in 2011 found that [[cannabidiol]] (CBD) also protects against [[hepatic]] ischemia/reperfusion injury by attenuating [[inflammatory]] signals and [[oxidative]] and nitrative stress response, resulting in [[cell]] death and [[tissue]] damage, but is independent of classic [[Cannabinoid receptor type 1|CB1]] and [[Cannabinoid receptor|CB]]2 receptors.
==Therapies Associated with Improved Clinical Outcomes==
==Therapies Associated with Improved Clinical Outcomes==
There are several preliminary studies in mice that seem to show that treatment with hydrogen sulfide ( H2S) could have a protective effect against reperfusion injury
Cyclosporine
In addition to its well-known immunosuppressive capabilities, the one-time administration of cyclosporine at the time of percutaneous coronary intervention (PCI) has been found to deliver a 40 percent reduction in infarct size in a small group proof of concept study of human patients with reperfusion injury published in The New England Journal of Medicine in 2008.
Cyclosporine works by inhibiting the action of Cyclophilin D which usually helps in opening Mitochondrial membrane transport protein ( MPT Pore). So once cyclophilin D action is inhibited, there is no more MPT pore opening and in turn saves the mitochondria from getting damaged.Treatment OF IRI.
The opening of MTP Pore results in major cell destruction by causing the influx of water into mitochondria and in turn impairing its function and ultimately leading to the collapse. The strategy to protect mitochondria is the most important thing associated with the treatment part.
The opening of the MPT pore leads to the inrush of water into the mitochondria, resulting in mitochondrial dysfunction and collapse. Upon collapse, the calcium is then released to overwhelm the next mitochondria in a cascading series of events that cause mitochondrial energy production supporting the cell to be reduced or stopped completely. The cessation of energy production results in cellular death. Protecting mitochondria is a viable cardio protective strategy.
Cyclosporine is currently in a phase II/III (adaptive) clinical study in Europe to determine its ability to ameliorateneuronal cellular damage in traumatic brain injury.
A series of 2009 studies published in the Journal of Cardiovascular Pharmacology indicate that metformin may prevent injury to cardiacreperfusion by inhibiting Mitochondrial Complex I and opening up MPT pore and in rats.
Cannabinoids
A research published in 2012 shows that the synthetic analog of phytocannabinoid tetrahydrocannabivarin (THCV), 8-Tetrahydrocannabivarin (THCV) and its 11-OH-8-THCV metabolite prevents hepatic ischemia/reperfusion injury by minimizing oxidative stress and inflammatory reactions through cannabinoid CB2 receptors, thereby lowering tissue damage and protective effects of inflammation. Pretreatment with a CB2 receptor antagonist, whereas a CB1 antagonist appeared to strengthen it, attenuated the defensive effects of somewhere else.
An earlier study published in 2011 found that cannabidiol (CBD) also protects against hepatic ischemia/reperfusion injury by attenuating inflammatory signals and oxidative and nitrative stress response, resulting in cell death and tissue damage, but is independent of classic CB1 and CB2 receptors.
Therapies Associated with Improved Clinical Outcomes
Medical treatment in IRI
Therapies that have been associated with improved clinical outcomes include:
Post conditioning (short repeated periods of vessel opening by repeatedly blowing the balloon up for short periods of time).
One study in humans demonstrated an area under the curve (AUC) of creatine kinase (C) release over the first 3 days of reperfusion (as a surrogate for infarct size) was significantly reduced by 36% in the post conditioned versus a control group
Infarct size reduction by PCI postconditioning persisted 6 months after AMI and resulted in a significant improvement in left ventricular (LV) function at 1 year
Inhibition of mitochondrial pore opening by cyclosporine.
Specifically, the study by Piot et al demonstrated that administration of cyclosporine at the time of reperfusion was associated with a reduction in infarct size
Infarct size was measured by the release of creatine kinase and delayed hyperenhancement on MRI
Limitations to applying strategies that have demonstrated benefit in animal models are the fact that reperfusion therapy was administered prior to or at the time of reperfusion. In the management of STEMI patients, it is impossible to administer the agent before vessel occlusion (except during coronary artery bypass grafting). Given the time constraints and the goal of opening an occluded artery within 90 minutes, it is also difficult to administer experimental agents before reperfusion in STEMI.
Therapies Associated with Limited Success
Pharmacotherapies that have either failed or that have met with limited success in improving clinical outcomes include:
GIK (glucose-insulin-potassium infusion) (Studied in the Glucose-Insulin-Potassium Infusion in Patients With Acute Myocardial Infarction Without Signs of Heart Failure: The Glucose-Insulin-Potassium Study (GIPS)-II and other older studies
Sodium-hydrogen exchange inhibitors such as cariporide (Studied in the GUARDIAN and EXPEDITION trials)
Adenosine (Studied in the AMISTAD I and AMISTAD II trials as well as the ATTACC trial ). It should be noted that at high doses in anterior ST elevation MIs, adenosine was effective in the AMISTAD trial. Likewise, intracoronary administration of adenosine prior to primary PCI has been associated with improved echocardiographic and clinical outcomes in one small study.
FX06, an anti-inflammatory fibrin derivative that competes with fibrin fragments for binding with the vascular endothelial molecule VE-cadherin which deters migration of leukocytes across the endothelial cell monolayer (studied in the F.I.R.E. trial (Efficacy of FX06 in the Prevention of Myocardial Reperfusion Injury)
Magnesium, which was evaluated by the Fourth International Study of Infarct Survival (ISIS-4) and the MAGIC trial.
Hyperoxemia, the delivery of supersaturated oxygen after PCI (Studied in the AMIHOT II trial).
Bendavia studied in the EMBRACE STEMI trial
There are several explanations for why trials of experimental agents have failed in this area:
The therapy was administered after reperfusion and after reperfusion injury had set in
The greatest benefit is observed in anterior ST elevation myocardial infarctions (as demonstrated in the AMISTAD study), and inclusion of non anterior locations minimizes the potential benefit