Long thoracic nerve
Template:Infobox Nerve Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
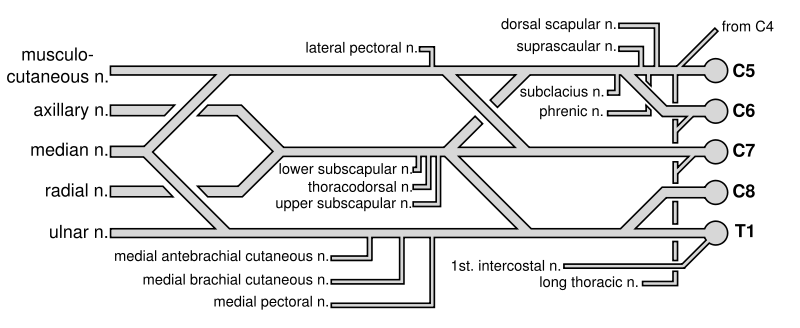
The long thoracic nerve (external respiratory nerve of Bell; posterior thoracic nerve) supplies the Serratus anterior. This nerve characteristically arises by three roots from the fifth, sixth, and seventh cervical nerves (C5-C7) but the root from C7 may be absent. The roots from C5 and C6 pierce the Scalenus medius, while the C7 root passes in front of the muscle.
The nerve descends behind the brachial plexus and the axillary vessels, resting on the outer surface of the Serratus anterior. It extends along the side of the thorax to the lower border of that muscle, supplying filaments to each of its digitations.
Damage
Due to its long, relatively superficial course, it is susceptible to injury either through direct trauma or stretch. Injury has been reported in almost all sports, typically occurring from a blow to the ribs underneath an outstretched arm. Surgically the long thoracic nerve can also be damaged during surgery for breast cancer, specifically radical mastectomies that involve removal of axillary lymph nodes.
Injuries to the nerve can result from carrying heavy bags over the shoulder for a prolonged time. There are also reports of isolated damage to this nerve as a variant of Parsonage Turner Syndrome, an autoimmune disease.
Symptoms are often minimal – if symptomatic, a posterior shoulder or scapular burning type of pain may be reported.
A lesion of the nerve paralyses the serratus anterior to produce scapula winging, which is most prominent when the arm is lifted forward or when the patient pushes the outstretched arm against a wall. However, even winging may not be evident until the trapezius stretches enough to reveal an injury several weeks prior.
Additional images
-
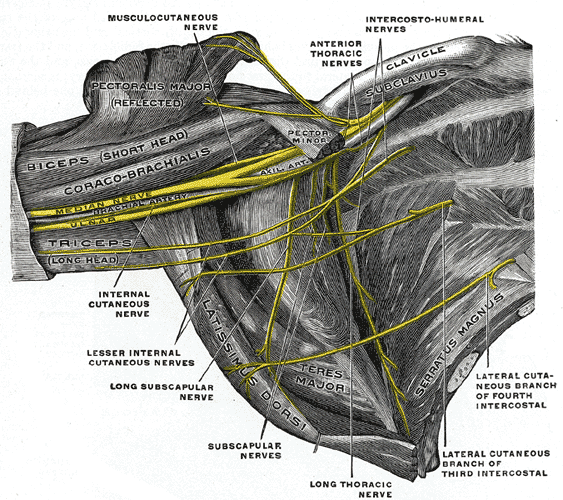
The right brachial plexus (infraclavicular portion) in the axillary fossa; viewed from below and in front.
-
Brachial plexus

External links
- Template:DukeOrtho
- Template:WhoNamedIt
- Template:EMedicineDictionary
- Template:SUNYAnatomyFigs - "The major subdivisions and terminal nerves of the brachial plexus."
de:Nervus thoracicus longus
id:Nervus thoracicus longus
sv:Nervus thoracicus longus