The heart in Chagas' disease
For more information about Chagas disease, click here.
| The heart in Chagas' disease | |
 | |
|---|---|
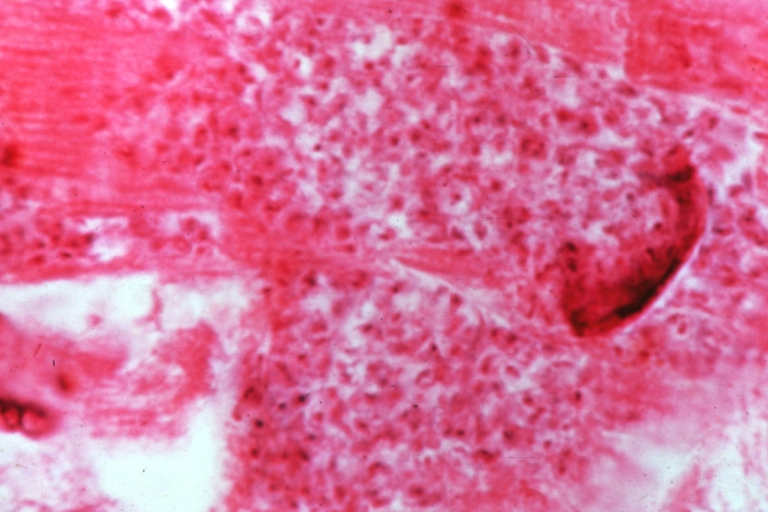
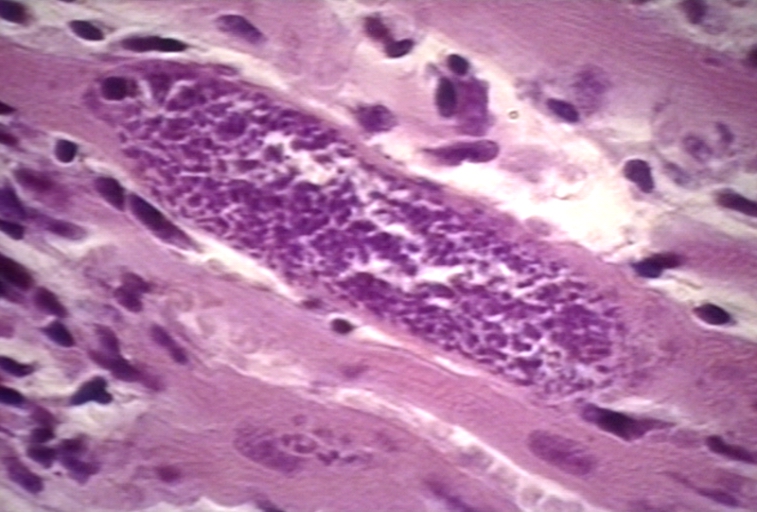
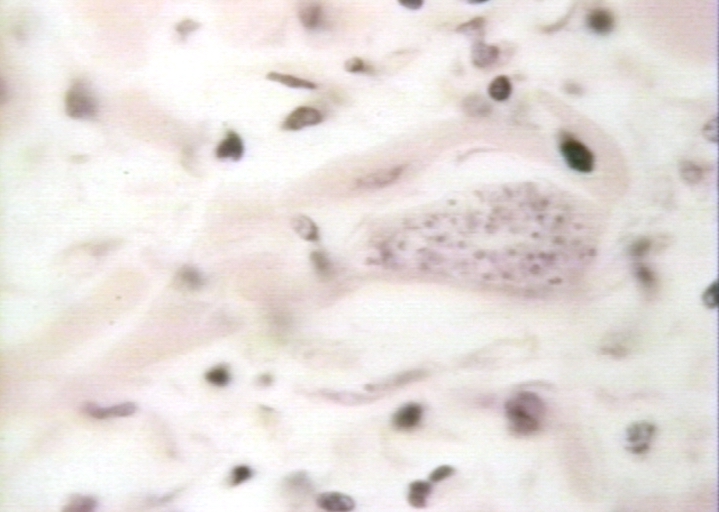
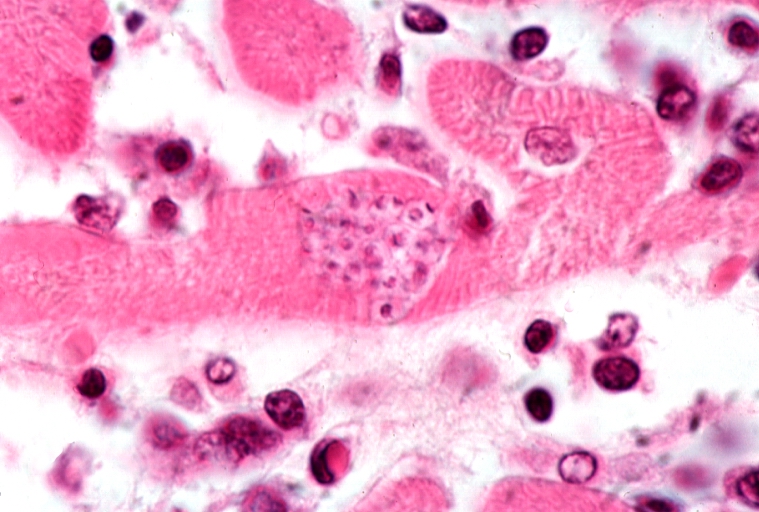
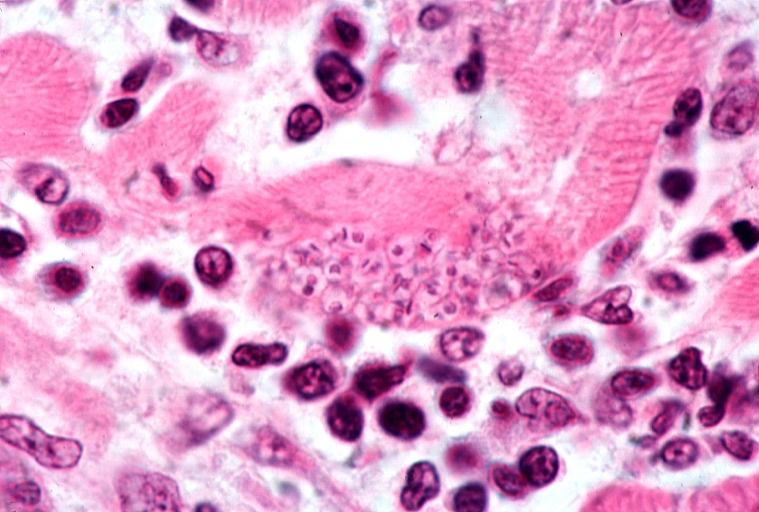
| This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. Note the T. cruzi amastigotes (arrows) within this longitudinal section of a myocyte. Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology |
|
Chagas disease Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
The heart in Chagas' disease On the Web |
|
American Roentgen Ray Society Images of The heart in Chagas' disease |
|
Risk calculators and risk factors for The heart in Chagas' disease |
Template:WikiDoc Cardiology News Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Chronic Chagas' disease leads to congestive heart failure. These patients commonly have right bundle branch block and/or other arrhythmias. These hearts are dilated and hypertrophied, have areas of fibrosis especially in the apex, and often contain mural thrombi. The myocardium is infiltrated with lymphocytes and macrophages and there is interstitial edema and fibrosis. This inflammatory reaction is most severe around the area of the right bundle branch. Patients may also develop megaesophagus and/or megacolon. [1] [2] [3]
Acute form of Chagas Disease
In a patient with diagnosed Chagas disease, cardiac damage is suspected if one or more following ECG findings occurs:
- Right bundle-branch block (RBBB),
- Left anterior fascicular block (LAFB),
- Atrio-Ventricular blocks
- Multifocal PVCs
- Sinus bradycardia
- Abnormal ST segment and / or T wave changes
- Abnormal T and / or Q waves
Myocarditis is infrequent, appearing in only 1-5% of patients whose having the acute phase of Chagas Disease (1-5 of every 10,000 infected subjects).
Chronic form of Chagas Disease
The histologic diagnosis of Chronic Chagas cardiomyopathy (CCM) consists of a diffuse and patchy chronic myocarditis, interstitial mononuclear cell infiltrates, and myocardial fiber destruction with fibrotic replacement. Grossly enlarged hearts have been found in autopsy studies in subjects with end stage of Chagas disease. Left ventricular apical aneurysms are also frequently found on autopsy.
The degree of myocardial fibrosis increases progressively from the mildest to the most severe disease stages. Additionally, myocardial fibrosis correlates inversely with left ventricular ejection fraction and clinical status.
Cardiac MRI may demonstrate myocardial involvement (hyperenhancement) among seropositive patients without clinical symptoms or left ventricular wall motion abnormalities.
Across groups A-D, coronary angiography is usually normal or shows minimally obstructive disease.
Case Example: Heart Involvement in Chagas Disease
Clinical Summary
A 12-year-old boy, whose family had recently emigrated from Brazil, presented to the emergency room with a three-day history of malaise, fever, anorexia, and edema of the face and upper extremities.
On physical examination the patient had generalized lymphadenopathy and hepatosplenomegaly.
The patient was tachycardic and dysgenic with signs of congestive heart failure.
A cardiac biopsy was performed which revealed an active myocarditis with leishmanial forms of parasitic organisms within cardiac myocytes.
Close examination of peripheral blood smears revealed occasional circulating trypomastigotes. A complement fixation test for antibodies to Trypanosoma cruzi was strongly positive.
-
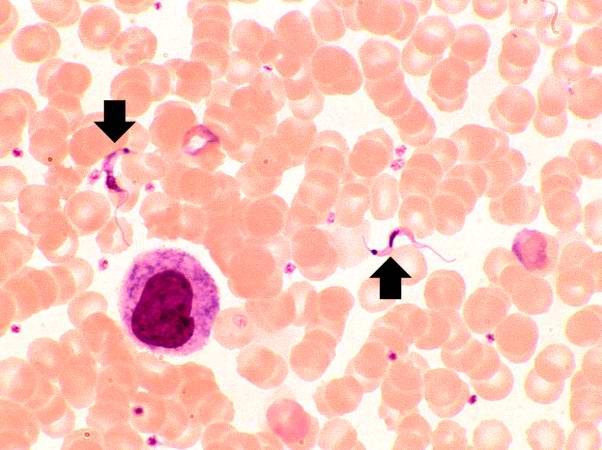
This peripheral blood smear from the patient shows two trypomastigotes of Trypanosoma cruzi.
-
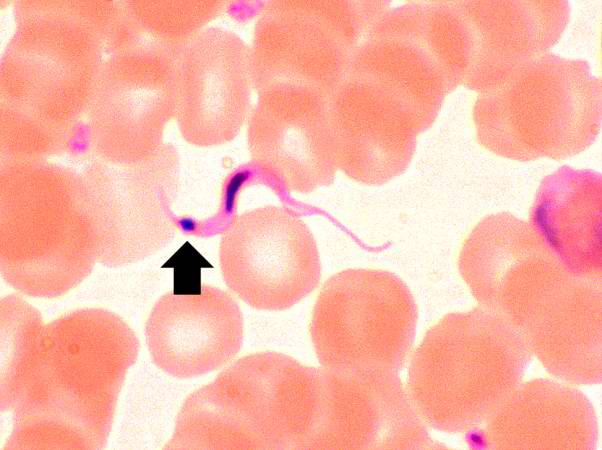
This peripheral blood smear from the patient shows a higher power view of a Trypanosoma cruzi trypomastigote. Note the prominent kinetoplast (arrow).


-
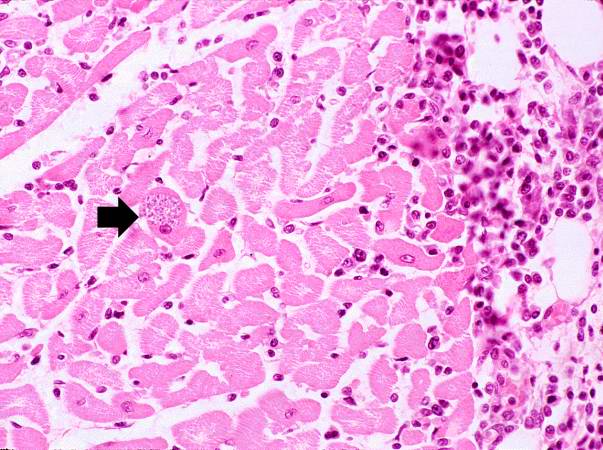
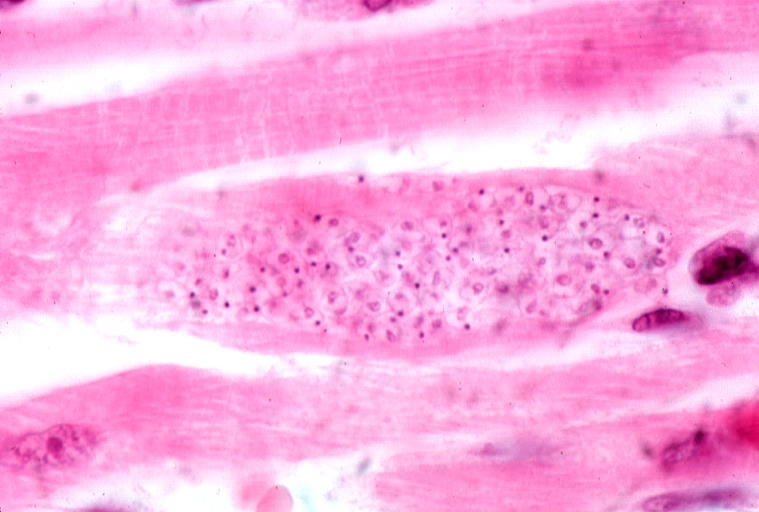
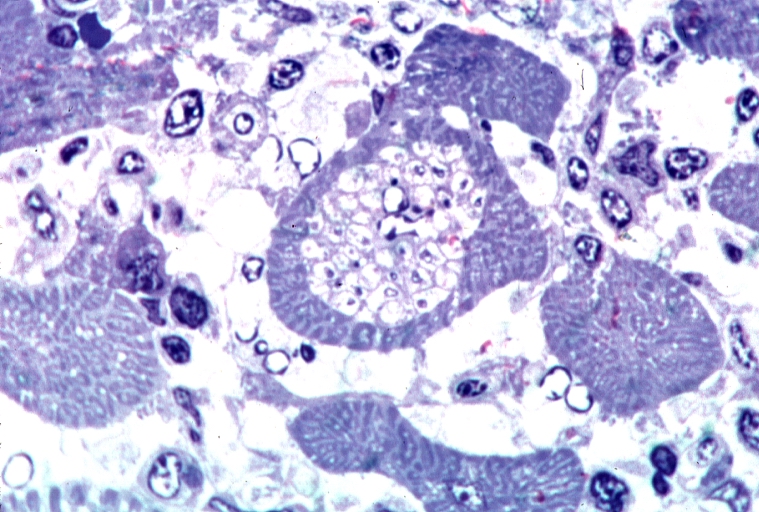
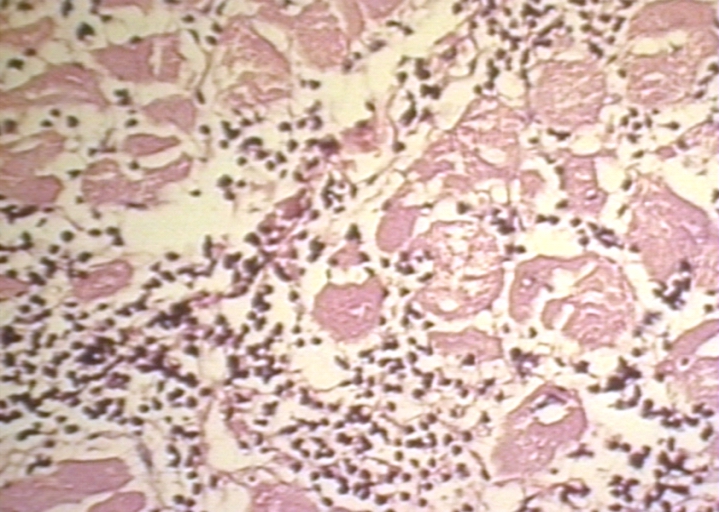
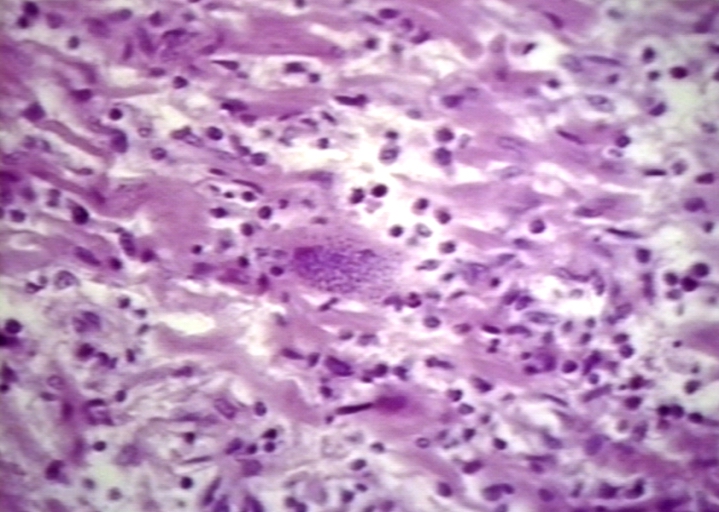
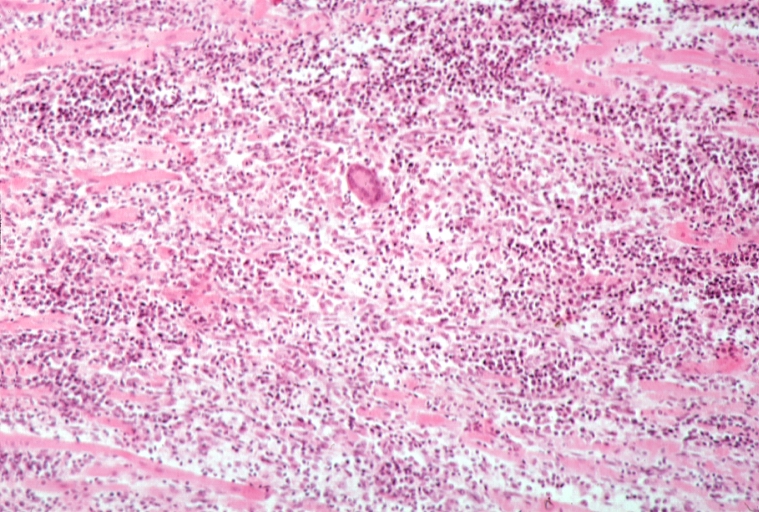
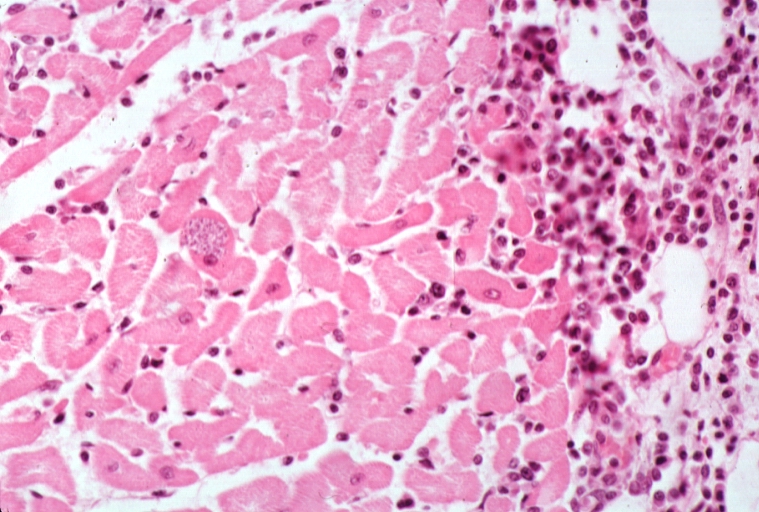
This is a low-power photomicrograph of an H & E stained section from the heart biopsy of this patient. Note the organisms within a myocyte (arrow) and the adjacent inflammatory response.
-
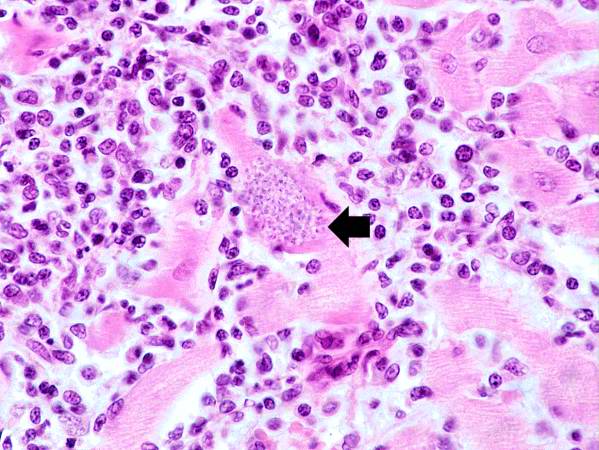
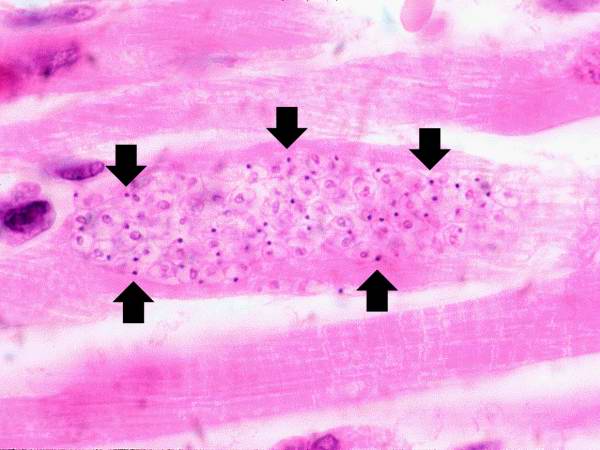
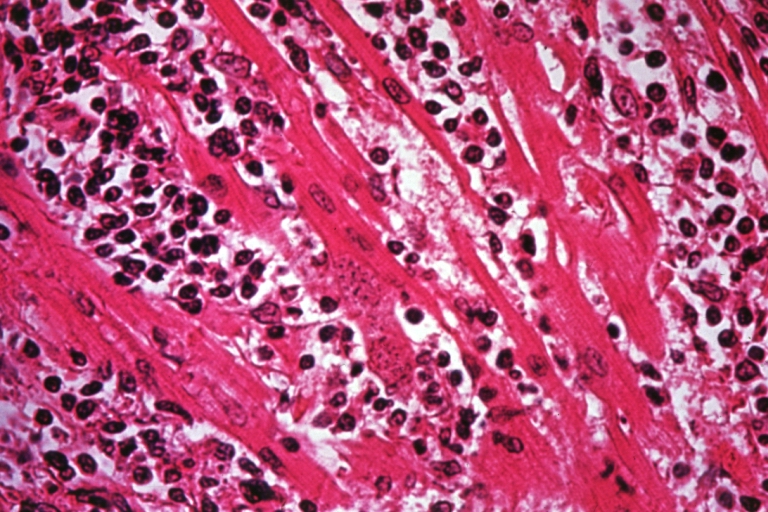
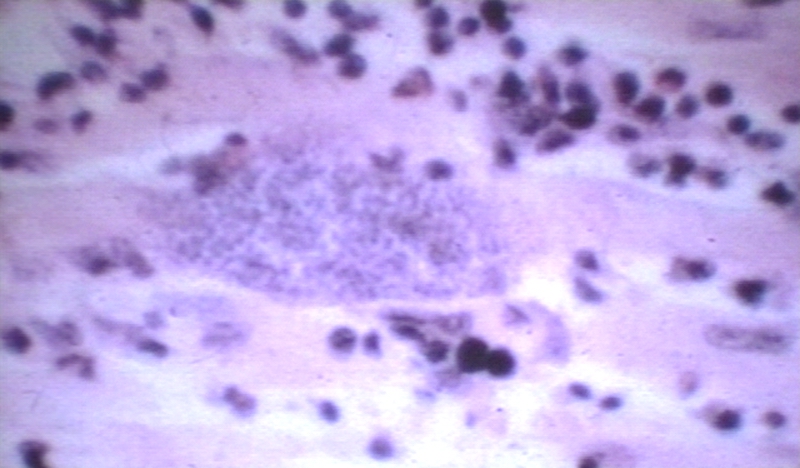
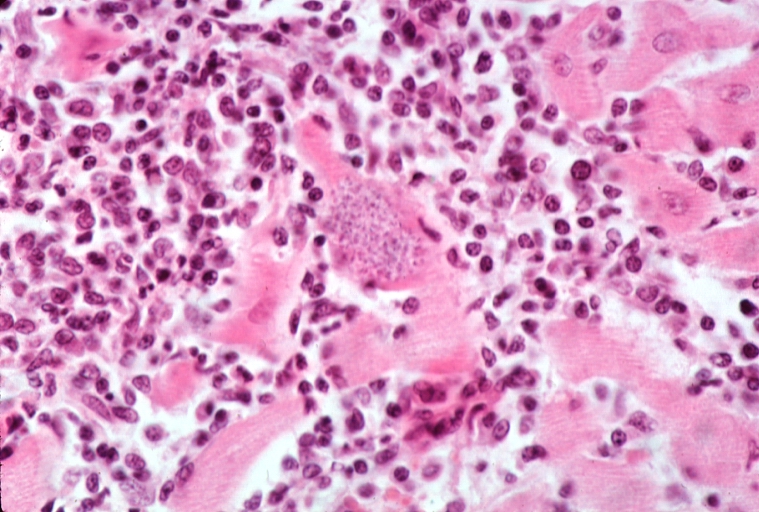
This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. Again, note the organisms within a myocyte (arrow) and the inflammatory response.


-
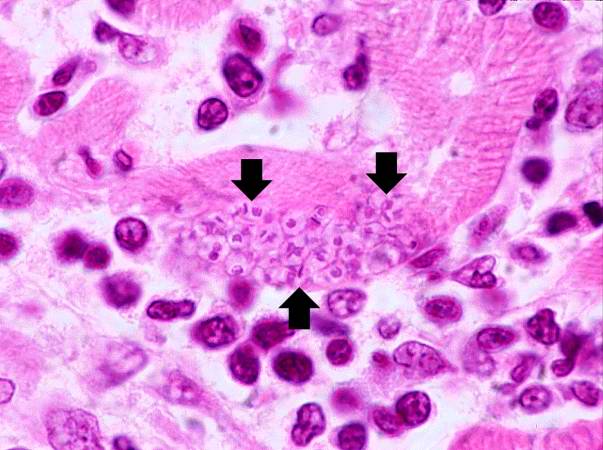
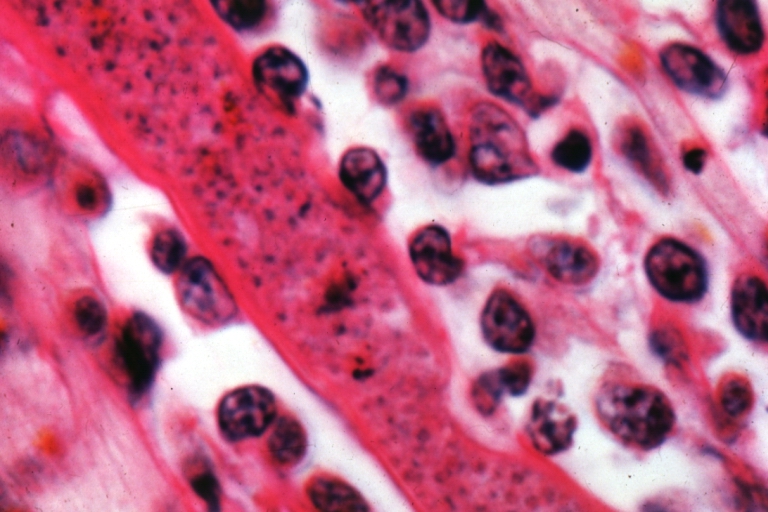
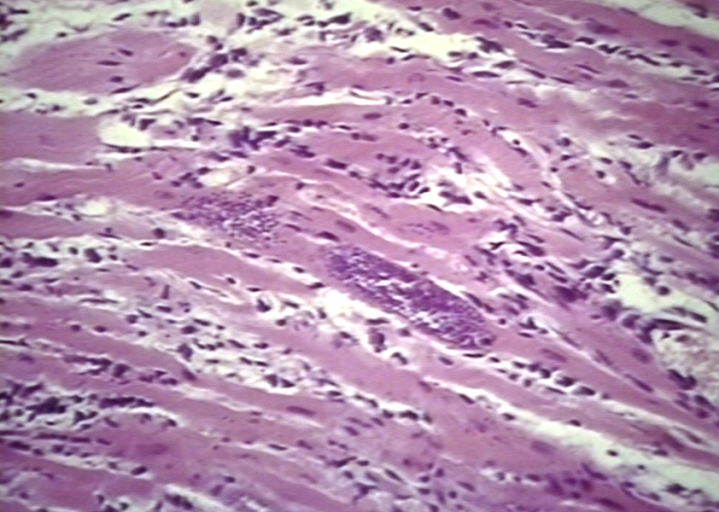
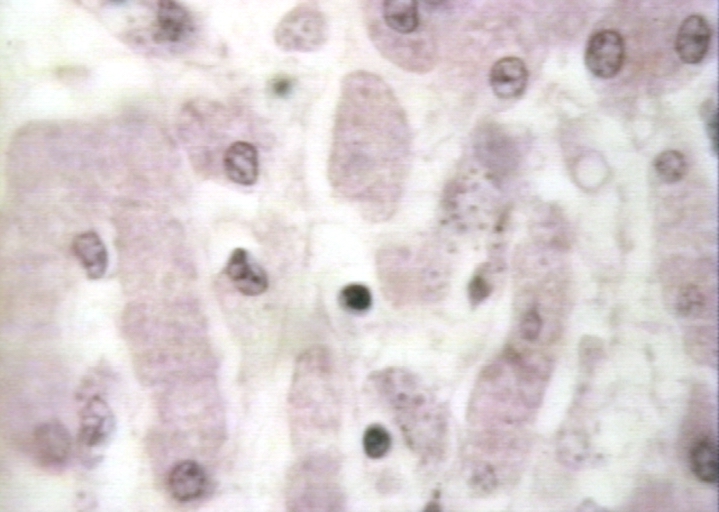
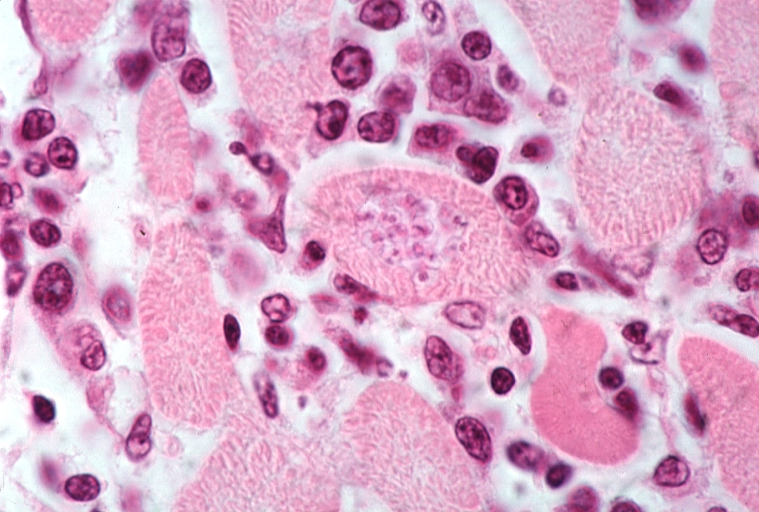
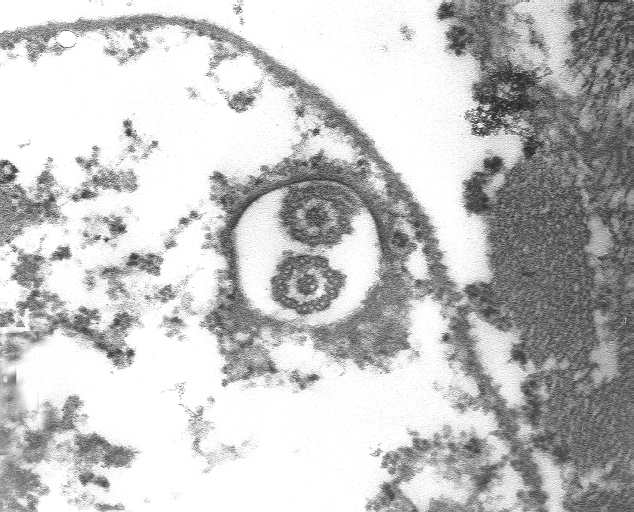
This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. At this magnification the organisms within a myocyte (arrows) and the adjacent inflammatory response are more clearly seen. The individual organisms within the myocyte are called amastigotes.
-
This is a higher-power photomicrograph of an H & E stained heart biopsy from this patient. Note the T. cruzi amastigotes (arrows) within this longitudinal section of a myocyte.

Additional Images
Microscopic Images
-

Heart: Chagas disease, acute
-
Heart: Chagas disease, acute


-
Heart: Chagas disease, acute, Trypanasoma cruzi, Geimsa stain
-
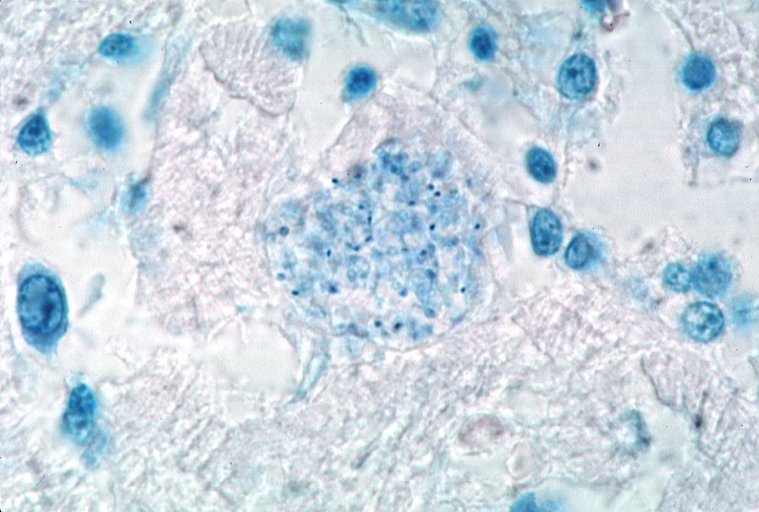
Heart: Chagas disease, acute, Trypanasoma cruzi, Geimsa stain


-
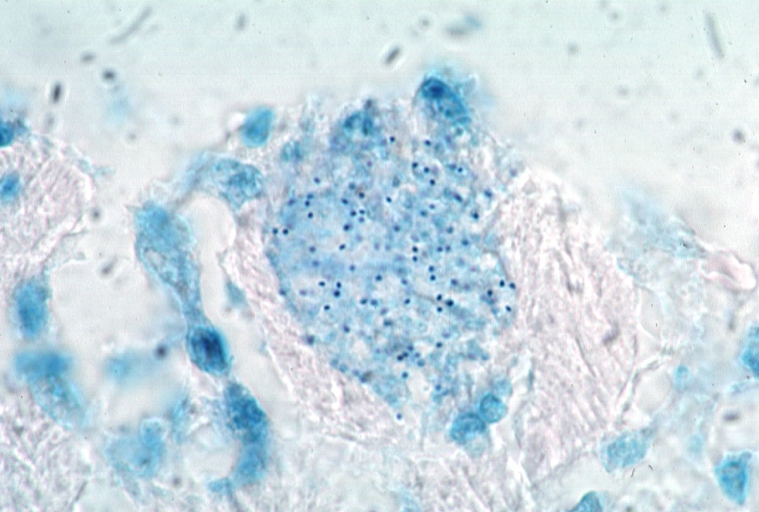
Heart: Chagas disease, acute, Trypanasoma cruzi, Geimsa stain
-
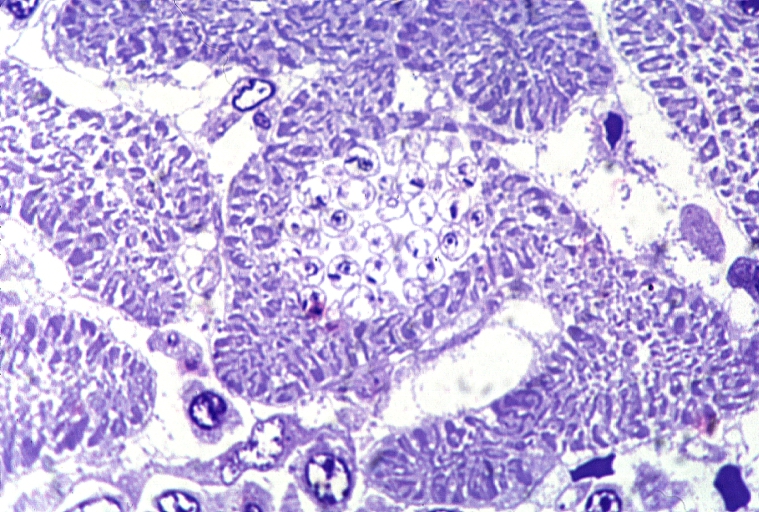
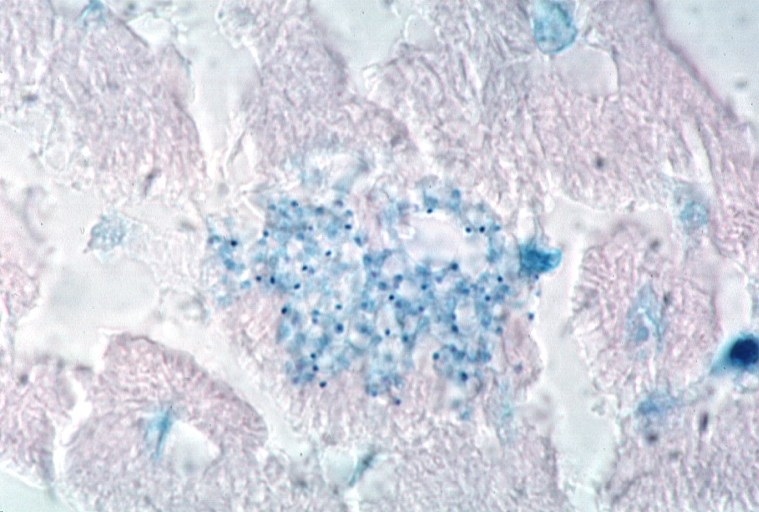
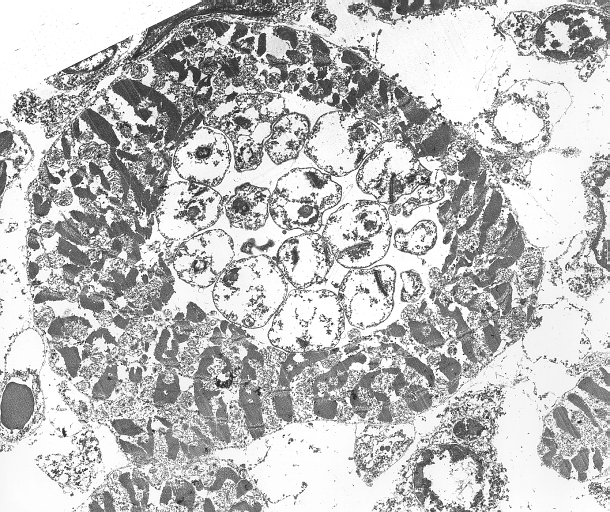
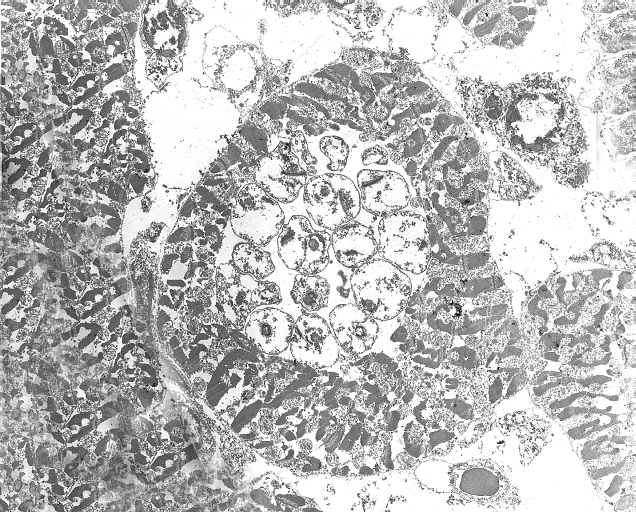
Heart: Chagas disease, acute, Trypanasoma cruzi, Toluidine blue, plastic section


-
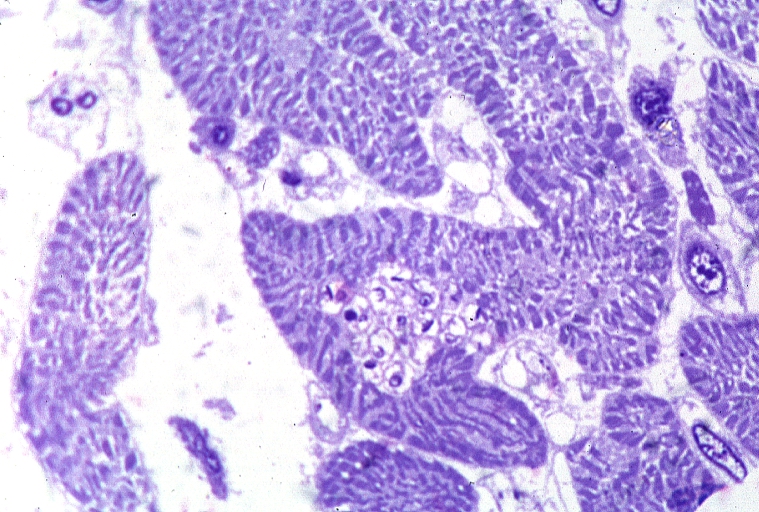
Heart: Chagas disease, acute, Trypanasoma cruzi, Toluidine blue, plastic section
-
Heart: Chagas disease, acute, Trypanasoma cruzi, Toluidine blue, plastic section


-
Heart: Chagas Disease, Leishmanial Forms
-
Heart: Chagas Disease, Leishmanial Forms


-
Heart: Chagas Disease, Leishmanial Forms
-
Heart: Myocarditis, Chagas Disease, Trypanosoma Cruzi


-
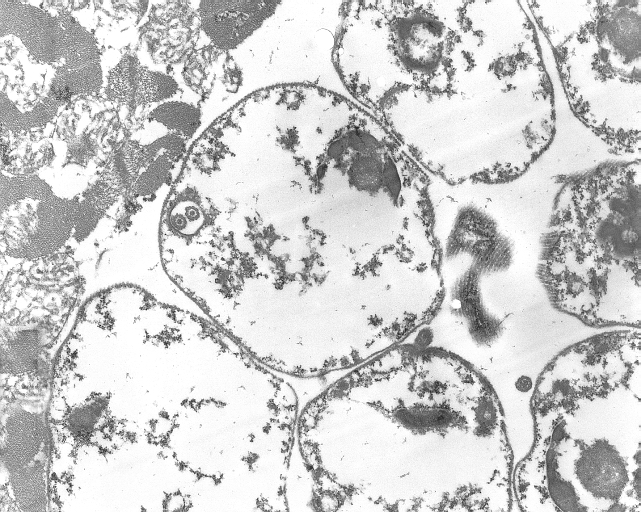
Heart: Trypanosoma Cruzi in Heart Muscle, Chagas Disease
-
Heart: Trypanosoma Cruzi in Heart Muscle, Chagas Disease


-
Heart: Trypanosoma Cruzi in Heart Muscle, Chagas Disease
-
Heart: Trypanosoma Cruzi in Heart Muscle, Chagas Disease


-
Heart: Chagas Disease
-
Heart: Chagas Disease


-
Heart: Acute Chagas Disease
-
Heart: Acute Chagas Disease


-
Heart: Acute Chagas Disease
-
Heart: Acute Chagas Disease


-
Heart: Acute Chagas Disease
-
Heart: Acute Chagas Disease


-
Chagas disease, acute, Trypanasoma cruzi
-
Chagas disease, acute, Trypanasoma cruzi


-
Chagas disease, acute, Trypanasoma cruzi
-
Chagas disease, acute, Trypanasoma cruzi


Gross Images
-
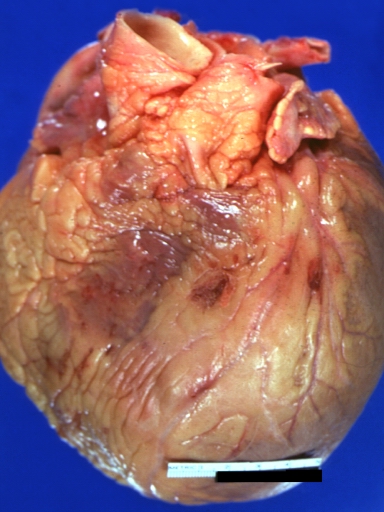
Heart: Gross, Natural Color, Acute Chagas Disease
-
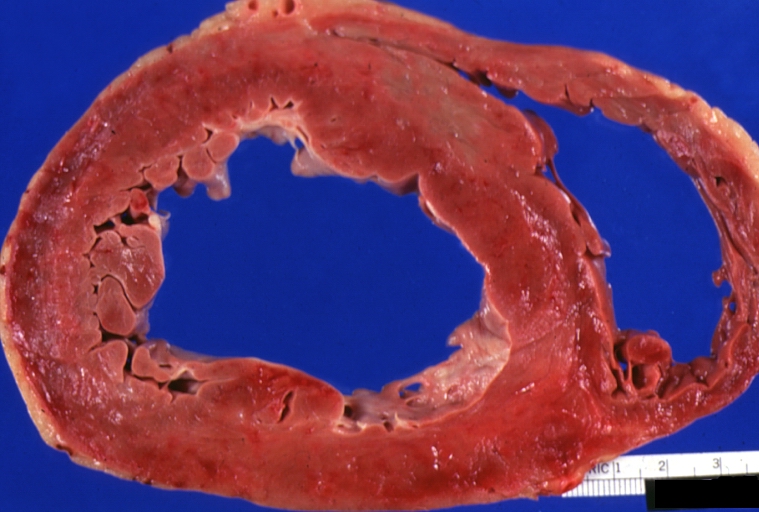
Heart: Gross, Natural Color, Acute Chagas Disease


References
- ↑ Acquatella H, Echocardiography in Chagas Heart Disease, Circulation. 2007;115:1124-1131
- ↑ Mady C, Ianni BM, Arteaga E, et al. Relation between interstitial myocardial collagen and the degree of clinical impairment in Chagas’ disease. Am J Cardiol 1999;84:354–6.
- ↑ Rochitte C. E., Oliveira P. F., Andrade J. M. et. al. Myocardial Delayed Enhancement by Magnetic Resonance Imaging in Patients with Chagas Disease; a Marker of Disease Severity. J Am Coll Cardiol 2005; 46: 1553-58